A Guide to Urgent Care Billing for Max Revenue in 2026
Precise urgent care billing means achieving a first-pass clean claim rate of 98% or higher by mastering coding, payer rules, and documentation. This is not about working harder, but about implementing a framework that leverages code-level expertise and technology to prevent denials and capture full reimbursement. This guide provides that exact framework for practice managers and physician owners to optimize revenue.
Your Essential Framework for Urgent Care Billing
In the fast-paced world of urgent care, your financial health depends entirely on your billing framework. A weak process means constant cash flow problems, while a strong one ensures stability and growth. It's the difference between chasing down payments and focusing on patient care.

We've seen the shift firsthand. Simple fee-for-service billing is gone. Today, top-performing urgent care centers achieve first-pass clean claim rates of 98% or higher by using a combination of pre-claim scrubbing technology and specialized billing teams. It's the new standard for survival.
What Makes Up a Strong Billing Structure?
A bulletproof billing structure isn't complicated. It’s built on a few essential pillars that work together to prevent revenue leakage. Think of it as the core operating system for your clinic's financial health.
It all starts with getting the basics right, every single time.
Accurate Coding: This is your foundation. It means pairing the right CPT codes for Evaluation & Management (E/M) and procedures with specific ICD-10 codes that prove to payers why the service was necessary. For example, billing CPT 99214 requires moderate Medical Decision Making (MDM), and your documentation must justify that level of complexity.
Modifier Precision: Getting modifiers right is critical, especially Modifier 25. Per AAPC and CMS guidelines, using it correctly on a claim with both an E/M service and a procedure is key to getting fully paid—and a huge red flag for auditors when documentation is insufficient.
Payer Rule Adherence: Every payer plays by a different set of rules. Knowing the specific quirks of Medicare, Medicaid, and your top commercial insurers—like which ones recognize after-hours code 99050—is the only way to stop simple, preventable denials.
KPI Tracking: You can't fix what you can't see. Monitoring metrics like Days in A/R and your Net Collection Rate tells you exactly where your revenue cycle is strong and where it's breaking down. To dig deeper, you can learn how to streamline medical billing processes and get ahead of problems.
For more deep dives into billing for different medical fields, you can explore our other resources at happybilling.co/specialties/.
Core CPT Codes for Urgent Care Encounters
To build a solid billing foundation, you need to master the codes you'll use every day. Think of these as the building blocks of every claim you submit. While every visit is unique, most encounters will pull from a core set of CPT codes for E/M, procedures, and related services.
Here’s a quick-reference table of the CPT codes that form the backbone of urgent care billing.
| Code Category | CPT Code(s) | Description | Billing Note |
|---|---|---|---|
| E/M Services | 99202–99205 | New Patient Office/Outpatient Visit | Based on medical decision making (MDM) or total time. |
| E/M Services | 99212–99215 | Established Patient Office/Outpatient Visit | The workhorses of urgent care. Level selection is critical. |
| Procedures | 12001–12018 | Simple Laceration Repair | Codes vary by body part and length of the repair. |
| Procedures | 10060/10061 | Incision and Drainage (I&D) | 10060 for simple/single; 10061 for complicated/multiple. |
| Procedures | 30901/30903 | Control of Nosebleed | 30901 for simple anterior packing; 30903 for complex. |
| Ancillary | 81002/81003 | Urinalysis (Non-Automated/Automated) | 81002 is for dipstick; 81003 for automated without scope. |
| Ancillary | 87880 | Rapid Strep Test | Often bundled by some payers, so check their policies. |
| Ancillary | 71045/71046 | Chest X-Ray (1 view / 2 views) | Requires proper documentation of medical necessity for the image. |
Knowing these codes inside and out—and when to apply them—is the first step toward reducing errors and accelerating your collections. They provide the language you need to accurately communicate the value of the care you provide to payers.
Correctly Coding E/M Levels and Procedures
Think of Evaluation and Management (E/M) and procedural coding as the two main engines that drive your urgent care revenue. Getting them both right is non-negotiable. Since the 2021 AMA guideline changes, you can code office visits based on either total time spent or the level of Medical Decision Making (MDM). In the high-velocity world of urgent care, MDM is almost always the more practical and defensible choice.
This is a critical distinction for both new patient visits (CPT codes 99202-99205) and established ones (99212-99215). Billing a level 4 visit (99214), for example, requires moderate MDM, while a level 5 (99215) needs high MDM. The golden rule is simple: your clinical notes must tell a story that justifies the code you choose.
Distinguishing MDM Levels in Practice
Let’s make this real. A patient walks in with classic sinusitis symptoms. The visit involves a limited history and exam, maybe a prescription for antibiotics, and that's it. This encounter fits squarely into CPT 99213 (low MDM). There’s minimal data to review and a low risk of anything going wrong.
Now, contrast that with a patient who arrives with chest pain, shortness of breath, and a history of hypertension. This isn't a simple visit. It's an investigation. You're likely running an EKG (CPT 93000), a chest X-ray (CPT 71046), and labs (e.g., Troponin, CPT 84484), all while sorting through a list of possible diagnoses—from GERD to anxiety to acute coronary syndrome. The work and risk involved here clearly justify a CPT 99214 (moderate MDM) or even a 99215 (high MDM), depending on the complexity and final outcome.
The core principle is simple: your documentation must paint a clear picture that justifies the MDM level. Payers will scrutinize high-level codes, looking for detailed notes on the number and complexity of problems addressed, the amount of data reviewed, and the risk of complications.
Coding Procedures with E/M Services
Urgent care isn't just about exams; it's about doing things. This is where many practices stumble and lose revenue—when a procedure is performed on the same day as an E/M service.
Common procedures include:
- Laceration Repair: Coded from the 12001-12018 series, based on location and length.
- Fracture Care: Applying a splint (CPT 29105-29131) or cast (CPT 29000-29086).
- I&D: Billing for an Incision and Drainage (10060).
When you perform a procedure like these alongside a separate and significant E/M service, you absolutely must append Modifier 25 to the E/M code. Imagine a patient comes in for a severe ankle sprain (the E/M service), but you also spot a small, unrelated cut on their arm that you decide to stitch up (the procedure).
To get paid for both, you’d submit the E/M code with the modifier (e.g., 99214-25) and the laceration repair code (12001). If you forget Modifier 25, the insurance company will bundle the E/M service into the procedure and deny payment for your evaluation work. It's a costly mistake, and a huge portion of urgent care revenue is tied to getting this single modifier right.
For a deeper analysis, you can learn more about correct CPT Modifier 25 usage and its documentation requirements in our dedicated article.
Navigating Payer-Specific Rules and Modifiers
In urgent care, the same claim can mean a quick payment or an instant denial—it all depends on which payer’s rulebook you’re following. What gets you paid by UnitedHealthcare could get your claim kicked back by Medicare. Success isn’t just about knowing codes; it’s about speaking the distinct language of each payer.
Think of it this way: every payer has its own dialect. When you bill for two separate procedures on the same patient visit, your choice of modifier is critical. For years, Modifier 59 was the go-to signal for a "distinct procedural service." But CMS grew tired of its overuse and decided to demand more clarity.
Adopting X-Modifiers for CMS Compliance
To crack down on ambiguity, Medicare and many Medicaid plans now push for—or even require—the more specific X-modifiers (XE, XS, XP, XU). Using these tells a much clearer story and prevents payers from assuming you've bundled services incorrectly.
- XE – Separate Encounter: For a service happening in a different encounter on the same day.
- XS – Separate Structure: The service was performed on a different organ or part of the body (e.g., a cut on the arm and another on the leg).
- XP – Separate Practitioner: Another provider in your clinic performed the service.
- XU – Unusual Non-Overlapping Service: The service is distinct and doesn’t overlap with the main procedure.
A claim with 99214-25 and 12002-XS for an established patient who got a URI check-up and a leg laceration repair is crystal clear to a Medicare contractor. Just using Modifier 59 is a gamble. Commercial payers are catching on, so switching to X-modifiers now is a smart, forward-thinking move.
Billing for After-Hours and Special Services
Your center works nights and weekends. That creates opportunities to bill for extended service times, but these after-hours codes are a minefield of payer-specific rules.
The rule is simple: Always verify payer policy before billing. CPT codes 99050 (services during scheduled evenings/weekends) and 99051 (services when the office is normally closed) are valuable, but not everyone pays for them.
CMS, for example, flat-out does not reimburse for 99050 or 99051. They consider extended hours as business-as-usual for an urgent care. But many commercial plans like Aetna or Cigna will pay for these codes when attached to a primary E/M service. Just be sure your documentation clearly notes the time of service to prove it.
This is a classic example of where a little bit of payer knowledge prevents a lot of lost revenue. Sometimes, justifying these services requires the same level of detailed support as more complex procedures, similar to what's needed when you learn more about what prior authorization in healthcare entails.
Strategies for Preventing and Managing Claim Denials
Tackling claim denials isn’t about working harder; it’s about working smarter. The difference between a practice with a clean 5% denial rate and one hemorrhaging cash with a 15% rate is a shift from a reactive to a proactive game plan. It’s about catching errors before they ever leave your system, not just chasing them after the fact.
Let’s be honest: rising denials are a crisis. They’re driven by a few key culprits—coordination of benefits (COB) headaches, prior authorization failures, and constant fights over medical necessity. Staffing shortages and burnout only pour fuel on the fire. While automation is the clear solution, a staggering 42% of billers still haven't adopted it, often due to budget fears, creating a massive performance gap. You can read the full research about these medical billing pain points to see just how deep the problem runs.
Get to the Root Cause of Common Denials
You have to stop the bleeding at the source. The single biggest mistake we see is practices just resubmitting a denied claim without figuring out why it was rejected in the first place. Simply rebilling a claim denied for medical necessity without beefing up the documentation or adding a more specific ICD-10 code is a recipe for a second denial.
Coordination of benefits is another constant pain point. For example, a patient hands over a new insurance card, but your front desk doesn't verify if it’s primary or secondary. The claim gets sent to the wrong payer, and boom—you get a denial with remark code CO-22: This care may be covered by another payer per coordination of benefits.
The fix is a non-negotiable workflow: implement real-time eligibility and benefits verification at check-in for every single patient. This simple step confirms the primary payer and flags COB issues upfront, preventing a denial that could otherwise take weeks to untangle.
Stop Denials Cold with Pre-Claim Scrubbing
Automated pre-claim scrubbing is your single most powerful weapon against denials. Think of it as an instant quality control check for every claim, catching the silly mistakes that cost you time and money. Integrated with your EHR, this technology automatically scans each claim for:
- Demographic Errors: Simple but costly typos like misspelled names or wrong birthdates.
- Coding Mismatches: An ICD-10 diagnosis that doesn’t medically justify the CPT service code.
- Modifier Issues: A missing Modifier 25 or using the wrong X-modifier for a specific payer’s rules.
This process flow shows you exactly how to navigate payer-specific rules to sidestep those common tripwires.
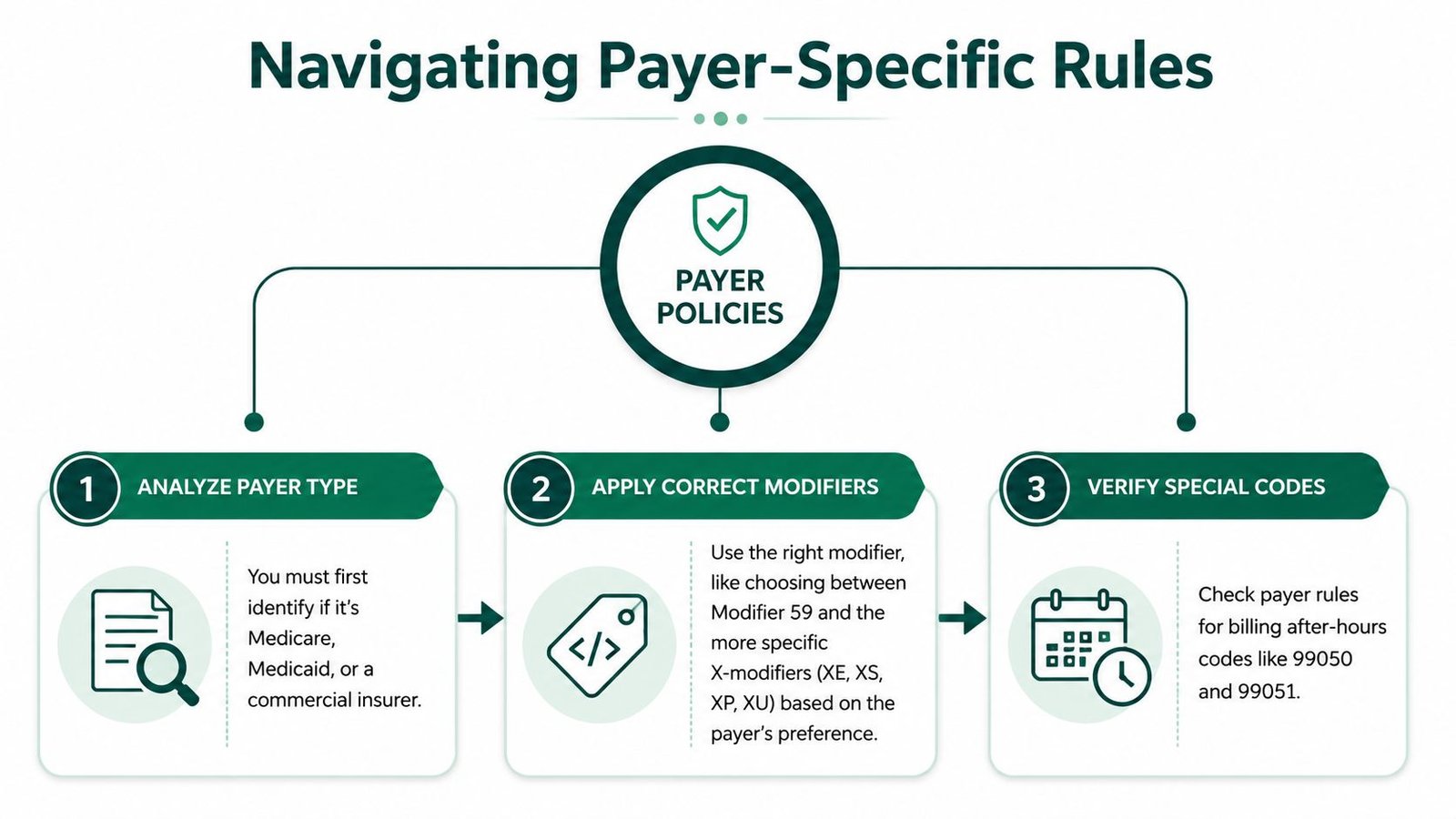
The workflow is simple but critical: identify the payer, apply the right modifiers, and verify any special codes. Systematizing this sequence builds a far more resilient revenue cycle. You can also learn more about medical billing denial management in our in-depth guide.
Build a Denial Management Machine
When a denial inevitably slips through, your team needs a structured playbook. Don't just throw them into a pile. Assign specific denial types to trained staff members. For instance, have one person become your expert on prior authorization denials (Denial Code 197) and another master all coding-related rejections (Denial Code 4). This specialization builds expertise fast and dramatically speeds up resolution times.
Your workflow absolutely must include tracking and trending your denial reasons. If you suddenly see a spike in denials for CPT 99214, you can run a quick audit of provider documentation for that specific code. This data-driven approach turns denial management from a reactive chore into a proactive quality improvement tool, strengthening your urgent care billing from the ground up.
Optimizing Your Patient Collections Process
The days of patient collections being an afterthought are over. With patient financial responsibility soaring, your urgent care's approach to collecting what you're owed is now a frontline issue that directly impacts your cash flow. If you're still relying on paper statements and surprise bills, you're not just creating a poor patient experience—you're actively slowing down your own revenue cycle.
The numbers don't lie. Between 2011 and 2024, the amount of money owed by patients shot up by a staggering 133%. This financial pressure is made worse by a massive transparency problem: only 22% of patients say they always know what a visit will cost them upfront. Yet, patients are telling us exactly how to fix this. A full 62% would rather pay online, and the use of eStatements has jumped by 243%. The takeaway is clear: convenience and clarity drive payments. You can get more details from the full JPMorgan report on healthcare payment trends.
Implement Upfront Cost Transparency
The collection process shouldn't start weeks after a visit with a confusing bill. It should start the moment a patient walks through your door. By using real-time eligibility (RTE) verification at the front desk, your staff can instantly see a patient’s insurance status, copay, and how much is left on their deductible. This isn't about guesswork; it's about providing a solid cost estimate right then and there.
Telling a patient their visit will involve a $75 copay and an estimated $150 toward their deductible completely changes the dynamic. It frames the payment as a routine part of the visit, not an unexpected shakedown a month later. This simple shift in communication makes collecting payment at the time of service far more likely.
When you provide clear cost estimates, you turn the payment conversation from a point of friction into a professional, expected part of the encounter. This doesn't just boost upfront collections; it builds patient trust.
Modernize Your Payment Options
Your patients expect to pay for healthcare with the same ease they order a pizza or a ride-share. Mailing paper statements and waiting for a check is a strategy from a bygone era, one that creates unnecessary delays and hurts your cash flow. A multi-channel payment strategy isn't just a "nice-to-have"—it's essential for any modern urgent care.
Give patients the convenient options they're already using everywhere else:
- Online Payment Portal: A secure, 24/7 portal on your website where patients can view their statements and settle balances on their own time.
- Text-to-Pay: Send a secure payment link directly to a patient’s phone for a fast, frictionless way to clear an outstanding balance.
- eStatements: Ditch the paper and postage. Emailing bills gets them to patients faster and cuts your overhead.
- Flexible Payment Plans: For larger balances, offering automated, structured payment plans is often the key to getting paid in full.
These digital tools meet patients where they are and make it easy for them to pay you. Improving this piece of your operation is fundamental to managing your financials, and our guide on accounts receivable in medical billing offers more strategies to get it right. A seamless payment experience is no longer a perk; it's a core component of a healthy revenue cycle.
Putting Technology to Work: Building a Smarter Revenue Cycle
A truly efficient revenue cycle isn't built on more staff working harder; it's built on smarter technology. By layering automation and artificial intelligence on top of your existing EHR, you can dramatically speed up cash flow and boost accuracy. The best part? No painful, costly system migration required. This is how you build a modern urgent care billing machine.

The impact is immediate. AI-powered coding tools can read clinical notes and suggest the right CPT and ICD-10 codes, saving your providers time and preventing common mistakes. It's a critical safety net, flagging potential mismatches between a diagnosis and a procedure before a claim even goes out the door. Of course, any tech, especially AI, must meet strict healthcare rules. For a deeper dive, check out this guide from SupportGPT on HIPAA for ChatGPT.
See Automation in Action
Beyond just coding, Robotic Process Automation (RPA) can take over the tedious, high-volume tasks that tie up your team all day. Imagine bots checking claim statuses on payer websites, posting payments, or verifying patient eligibility around the clock. This frees your expert billers to do what they do best: fight complex denials and analyze revenue trends.
This is the fundamental difference between basic practice management software and a true RCM partner. A partner provides a 24/7 global workforce that follows the sun, ensuring your claims are constantly being worked—not just from 9 to 5.
Hitting the Benchmarks That Matter
The point of all this tech isn't just to be more efficient; it's about hitting real numbers that pad your bottom line. A tech-forward workflow is how top-performing urgent care centers consistently hit these crucial KPIs:
- Days in A/R Under 35: By automating claim submission and follow-up, you secure payments faster, keeping your accounts receivable from getting old and stale.
- Clean Claim Rate of 98% or Higher: AI-driven pre-claim scrubbing acts like a spell-checker for billing, catching errors in codes, modifiers, and demographics before they can trigger a denial.
- Real-Time KPI Dashboards: Modern RCM platforms give you an instant, clear view of your financial health. You can spot a negative trend in the morning and take action to fix it by the afternoon.
Integrating the right tech turns your revenue cycle from a reactive, paper-pushing chore into a proactive, data-driven operation. It's the move you make when you're ready to stop just managing claims and start truly optimizing revenue.
How do I correctly bill an E/M service and a procedure together?
Append Modifier 25 to the Evaluation and Management (E/M) code (e.g., 99214-25) when you perform a "significant, separately identifiable" evaluation on the same day as a minor procedure. For instance, a patient presents for a severe cough and chest congestion (the E/M service), and during the exam, you also notice and remove a foreign body from their ear (the procedure, CPT 69200). Your documentation must clearly support the medical necessity for both services independently to satisfy payer requirements, especially those from auditors like CMS.
What are the most common CPT codes I should master for urgent care?
The workhorses of urgent care billing are the established patient E/M codes 99212-99215. Beyond that, you must be an expert in common procedure codes like simple laceration repairs (12001-12018), incision and drainage (10060), and rapid diagnostic tests such as for influenza (87804) or strep (87880). Mastering these, along with the correct application of modifiers like 25 and 59/X-series, is fundamental to a healthy revenue cycle.
What is the most common reason for urgent care claim denials?
The most frequent denials stem from front-end administrative errors. These include incorrect or incomplete patient demographic data, invalid insurance policy numbers, and failure to verify primary vs. secondary payers (Coordination of Benefits). Another major culprit is failing to obtain prior authorization when a specific payer policy requires it for services like high-level imaging. These denials are almost entirely preventable with robust front-desk processes and real-time eligibility verification technology.