Revenue Cycle Management Benefits for Your Practice
The primary revenue cycle management benefits are faster cash flow, fewer claim denials, and stronger operational efficiency. Effective RCM also delivers eight documented benefits, including improved patient experience, shorter payment cycles, decreased administrative costs, increased cash flow, fraud reduction, and enhanced compliance.
That sounds obvious until you audit a real practice. The biggest leaks usually aren't dramatic. They're a missing authorization on a high-value visit, a modifier omitted on a procedural claim, an eligibility check skipped at intake, or a payment posted without anyone catching an underpayment. Small breakdowns at the front end become expensive A/R at the back end.
Practice owners are treating RCM as a strategic operating function for a reason. The global market was valued at $163.72 billion in 2025 and is projected to reach $472.42 billion by 2034, growing at 12.70% CAGR, according to Fortune Business Insights on the revenue cycle management market. When a market grows at that scale, it usually means the problem is bigger than billing software. It means practices have realized reimbursement discipline is tied directly to financial stability.
The Core Benefits of Revenue Cycle Management

RCM benefits show up where practice owners feel pain first. In the bank account, in staff workload, and in the aging report. A disciplined revenue cycle gets claims out cleanly, resolves exceptions faster, and prevents staff from spending their week reworking errors that should never have reached the payer.
That shift matters because growth in this category isn't driven by hype alone. It's driven by the recognition that reimbursement has become too complex to manage with disconnected front-desk habits and reactive billing. If you're comparing process improvements across industries, some of the same logic behind AR automation for professional services applies here: speed, accuracy, visibility, and fewer manual handoffs all improve collections performance.
What the benefit really is
The benefit isn't "better billing." That's too vague to manage.
The benefit is tighter control over a chain of events that determines whether a CPT code becomes cash, gets denied, or dies in follow-up. If a cardiology office bills 93306 without aligning diagnosis support and payer edits, or if an orthopedic group submits a post-op E/M during a global period without the right modifier logic, the problem isn't coding in isolation. The problem is a weak revenue cycle.
Where practices actually gain
A strong RCM program usually improves performance in these areas:
- Cash velocity: Claims move from charge entry to payer acceptance with fewer avoidable delays.
- Denial prevention: Teams catch front-end and coding defects before they become payer work.
- Administrative efficiency: Staff stop touching the same account multiple times.
- Financial visibility: Leaders can see where money is stuck, by payer, location, provider, and claim type.
- Scalability: Growth doesn't automatically create billing chaos.
Practical rule: If your billing team spends more time correcting submitted claims than preventing bad claims, your revenue cycle is underperforming.
For a deeper operational framework, review these revenue cycle management best practices. The main point is simple. Revenue cycle management benefits aren't abstract. They're the difference between a practice that controls reimbursement and one that reacts to it.
Understanding the Modern Revenue Cycle
Revenue cycle management starts before the visit and doesn't end when the claim is filed. It's the full financial workflow from scheduling through final payment, patient balance resolution, and denial appeal when needed. If any stage fails, the next stage inherits the damage.
Research published in the NIH library notes that effective RCM delivers eight key benefits: improved patient experience, reduced claim denials, shorter payment cycles, decreased administrative costs, increased cash flow, elimination of coding fraud, elimination of patient fraud, and enhanced compliance, as detailed in this PMC review of revenue cycle management benefits.
Front-end accuracy decides back-end pain
Most preventable losses begin before coding.
At pre-registration and registration, staff need correct demographics, active insurance, referral status when required, and authorization details when applicable. If the subscriber ID is wrong or coverage isn't verified, a clean CPT code still becomes a reject. For behavioral health, that often means a service like 90837 is technically documented and clinically appropriate, yet financially dead on arrival because the authorization wasn't secured or attached correctly.
Front-end discipline usually includes:
- Eligibility verification: Confirm active coverage before the date of service.
- Authorization control: Track payer rules for services that need pre-approval.
- Benefit review: Identify patient responsibility early so balances don't drift into bad debt.
- Referral validation: Confirm PCP referral requirements when payer plans still enforce them.
Coding, claim editing, and payment posting are one system
Charge capture and coding are where specialty knowledge earns its keep. CMS rules, payer policies, NCCI edit logic, modifier sequencing, and documentation support all matter. A procedural claim may need modifier 59, 25, 26, TC, QK, or another modifier depending on specialty and circumstance. The wrong modifier doesn't just reduce revenue. It creates rework, appeal time, and A/R drag.
Then comes claim scrubbing and submission. A claim should be checked for coverage conflicts, coding mismatches, demographic issues, and payer-specific edits before it leaves the practice management system. Once the remittance arrives, payment posting shouldn't be a blind "post and go" exercise. Teams need to catch denials, partial payments, and underpayments while the appeal window is still open.
A revenue cycle isn't a billing department task list. It's a control system for reimbursement.
For a grounded overview of each stage, this guide on what revenue cycle management is is a useful reference. Practices that treat intake, coding, claim editing, posting, and follow-up as separate silos usually create their own denial volume.
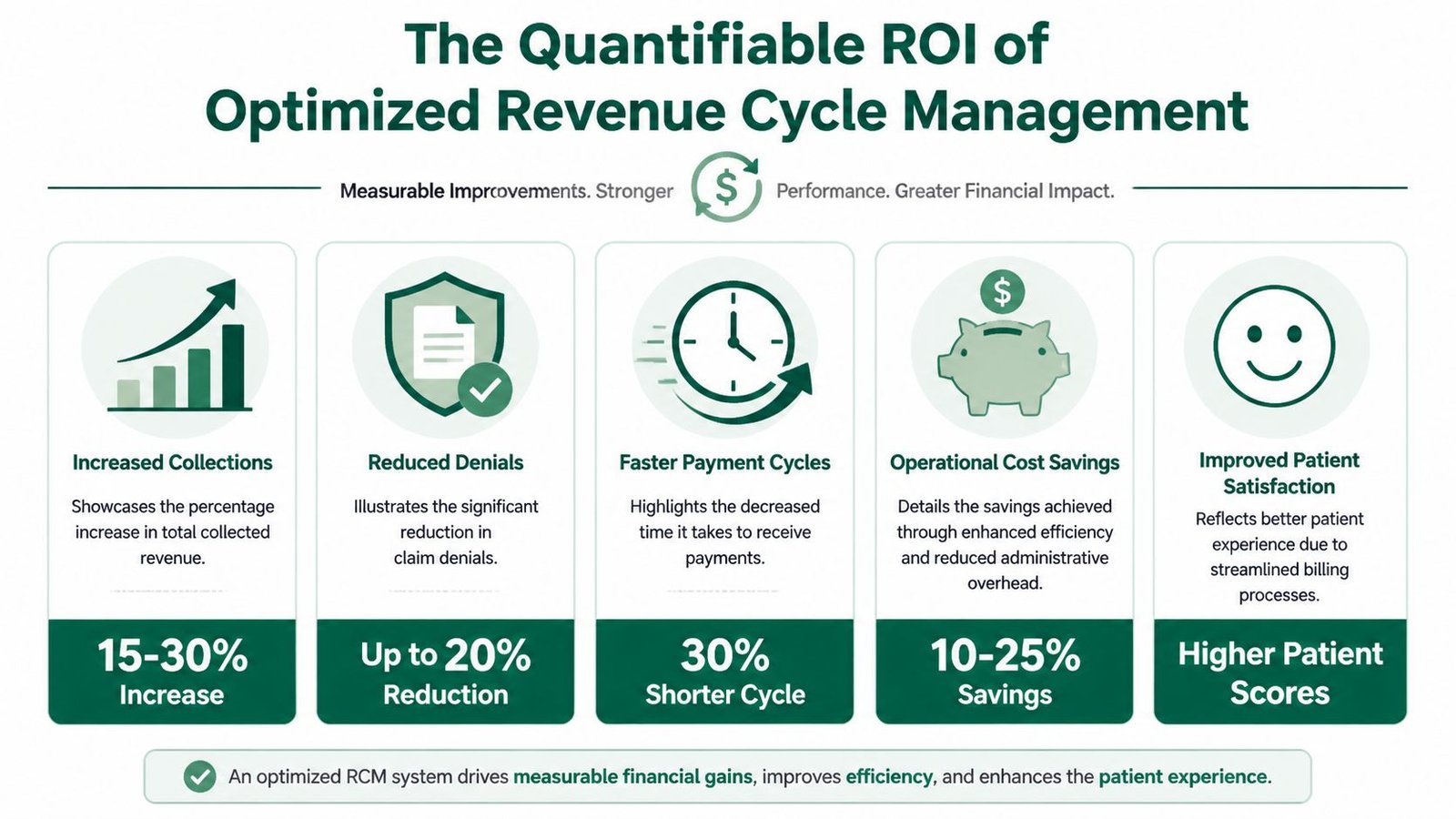
The Quantifiable ROI of Optimized RCM
If you want to measure revenue cycle management benefits properly, don't start with vendor demos. Start with three KPIs: first-pass clean claim rate, days in A/R, and denial rate. These numbers tell you whether your process is preventing rework or creating it.
First-pass clean claim rate
First-pass clean claim rate measures how many claims get accepted the first time without correction or resubmission. In practical terms, it's a test of whether your intake, coding, editing, and payer-rule controls are working before the claim leaves the building.
The strongest benchmark provided in the brief is above 95% for specialized practices. That matters because Plutus Health's discussion of RCM benefits states that about 90% of health insurance claim denials are tied to minor technical issues such as missing information, incorrect coding, or incomplete authorization data. The same source notes that the average hospital can increase annual revenue by $5 million through denial prevention alone.
A simple way to calculate it:
- FPCR formula: Clean claims accepted on first submission / total claims submitted
If your anesthesiology group repeatedly bills 00812 but misses an anesthesia modifier such as QK where medical direction rules apply, you don't have a payer problem first. You have a clean-claim problem.
Days in A/R
Days in A/R tells you how long charges sit before becoming cash. This is one of the clearest financial health signals in a practice because it exposes whether money is moving or aging.
A practical self-audit looks like this:
| KPI | What to review | What it tells you |
|---|---|---|
| Days in A/R | Aging by payer, provider, and location | Where cash is slowing down |
| FPCR | Rejections and edits by root cause | How much rework your team is creating |
| Denial rate | Denials by code family and payer reason | Which operational failures are recurring |
If you want a better framework for reading aging reports, this guide on days in A/R is worth keeping handy.
For claims leaders building better visibility, the OMOPHub guide on claims data analytics is also useful because it helps translate raw claims activity into operational signals.
Denial rate and cash impact
Denial rate is straightforward in concept but often poorly tracked. Separate clinical necessity denials from technical denials, timely filing denials, authorization denials, and coding denials. If you lump them together, you can't fix the actual cause.
Track denials by payer rule, not just by payer name. "Aetna denied it" isn't a root cause.
You don't need dozens of dashboards. You need disciplined measurement on the handful of indicators that tell you whether claims are leaving cleanly, paying quickly, and returning predictably.
How RCM Benefits Translate Across Medical Specialties
A generic RCM workflow sounds fine until you apply it to specialty billing. That's where most outsourced arrangements break down. The core mechanics are the same, but the failure points change by specialty, by code set, and by payer edit logic.
The practical value of automation is clearest in specialties with coding complexity. DrChrono's review of end-to-end RCM notes that automated eligibility verification, integrated billing systems, and real-time dashboards reduce days in A/R, and it specifically points to cardiology and orthopedics as examples where automation accelerates payment by improving coding and modifier accuracy at submission.
Anesthesiology
Anesthesia billing is one of the fastest ways to expose whether an RCM team understands specialty reimbursement. You aren't just billing a CPT code. You're billing base units, time units, physical status when supported, concurrency rules, and the correct modifier combination.
Take CPT 00812. If the case is medically directed, modifier choice matters. QK is not interchangeable with other anesthesia modifiers, and the documentation has to support the billing scenario. If time documentation is inconsistent, start and stop times don't reconcile, or concurrency isn't tracked properly, the claim may not deny immediately. It may underpay, suspend, or trigger downstream audit exposure.
For a specialty-specific view, see this resource on anesthesiology billing.
Mental health
Behavioral health revenue cycle problems are often authorization problems wearing a billing mask. A clinic may deliver 90837 appropriately, but if visit limits, payer authorization requirements, or telehealth billing conditions aren't checked before the encounter, the back office inherits avoidable denials.
What works in mental health is boring but effective. Tight intake scripts, authorization tracking tied to the appointment schedule, and claim edits that flag expired approvals before submission. What doesn't work is discovering after the session that the payer required an authorization update two visits ago.
Cardiology
Cardiology combines volume, diagnostic complexity, and payer scrutiny. A common example is 93306. On paper it's routine. In practice, payment depends on correct diagnosis support, place-of-service logic, and modifier use when components or related services create edit issues.
Cardiology groups also suffer when charge lag builds around diagnostic testing and interventional cases. The best RCM setups push claims quickly, track payer-specific edits, and show which code families are driving denials. That's where dashboards matter. Not because dashboards are fashionable, but because they show where the reimbursement pipeline is breaking.
A related operational guide is this piece on cardiology revenue cycle management.
Orthopedics
Orthopedic billing exposes a different kind of weakness. Global periods, postoperative edits, multiple procedure reductions, and modifier discipline all collide in the same claim inventory.
Consider 27447. That code brings global surgery rules into play. If the practice bills a post-op E/M without support for a separate service, the payer may deny it or bundle it. If a distinct procedural service is separately reportable, teams often reach for modifier 59 too casually or too late. The modifier only works when documentation supports distinctness under payer and coding rules. It isn't a universal override button.
In orthopedics, a bad global-period workflow can make a profitable surgical schedule look weak on paper.
The larger point is this. Revenue cycle management benefits are real, but they're not delivered by generic "medical billing support." They're delivered by people and systems that understand the claim-level rules that control reimbursement in your specialty.
Beyond Finance Operational and Compliance Advantages
The best revenue cycle improvements don't just raise collections. They remove friction from the practice.
When eligibility checks, charge review, claim status monitoring, and follow-up queues are organized properly, staff stop firefighting. Front-desk teams spend less time fixing insurance mistakes after the visit. Billers spend less time reopening avoidable denials. Managers spend less time guessing why one payer is aging badly and another isn't.
Operational lift is a real benefit
A well-run revenue cycle changes how the office functions day to day.
- Staff focus improves: Teams handle fewer preventable exceptions and more productive work.
- Scheduling becomes cleaner: Authorization and eligibility issues get caught before the patient is on the schedule for the wrong service.
- Patient billing gets clearer: Better statements and cleaner adjudication reduce confusion around balances.
- Leadership gets usable visibility: Aging, denial trends, and payer behavior become easier to act on.
The softer benefits matter because operational friction usually hits patient access and throughput before anyone names it an RCM issue. If a mental health practice keeps rescheduling visits because approvals aren't in place, or an anesthesia group keeps holding charges due to missing case details, the revenue cycle is affecting operations directly.
Compliance is where weak processes get expensive
RCM also protects the practice from self-inflicted compliance exposure. Coding needs to match documentation. Modifiers need to be supported. Payer rules need to be followed consistently. CMS guidance, CPT coding conventions, NCCI edits, and payer medical policies don't care whether a staff member was rushed that day.
That matters for codes with heavy scrutiny, but it also matters for ordinary workflows. An unsupported modifier 25 on an E/M claim, habitual misuse of modifier 59, or weak documentation around anesthesia medical direction creates risk beyond one denied claim. It creates a pattern.
Compliance problems usually enter the system as workflow shortcuts, not deliberate fraud.
Practices that invest in disciplined RCM tend to get a secondary advantage. Cleaner documentation habits, more consistent charge review, and fewer payment surprises for both payers and patients.
Evaluating and Choosing the Right RCM Partner
Most RCM vendors sound good in a demo. That's the easy part. The hard part is determining whether they can operate inside your specialty's billing reality, your EHR, and your payer mix without creating new friction.
The buying problem is bigger than feature comparison. Forrester's analysis of healthcare RCM decision-making points out that practices need transparent, specialty-segmented case studies and comparative performance data, and that basic questions about implementation time-to-value, hidden costs, and ROI across in-house versus outsourced models often go unanswered.
Questions that separate real operators from polished sales teams
Ask outcome questions, not branding questions.
- What is your first-pass clean claim performance by specialty? If they answer with general process language and no operating discipline, keep digging.
- What do you do with authorization-heavy services like 90837? You want workflow detail, not software buzzwords.
- How do you manage global-period claim edits around codes like 27447? The answer should mention documentation review, modifier logic, and payer-specific handling.
- How do you handle anesthesia concurrency and modifier scenarios such as QK on 00812? This exposes whether they understand real specialty billing.
- How do you identify underpayments after ERA posting? If they don't review remits analytically, they'll miss money.
What works and what doesn't
A strong partner usually has a few traits in common:
| What to look for | Why it matters |
|---|---|
| Specialty fluency | Generic teams miss code-level nuances |
| EHR compatibility | Workflow disruption kills adoption |
| Root-cause reporting | You need fixes, not denial summaries |
| Clear escalation paths | Complex payer issues need ownership |
What doesn't work is choosing based on vague AI promises, generic dashboards, or low headline pricing. If the partner can't explain how they prevent denials before submission, appeal complex payer denials, and monitor payer-specific reimbursement patterns, the cost savings usually evaporate into rework.
Buyer filter: Ask them to walk through one denied claim from intake to appeal. If they stay high level, they probably operate high level.
If you're weighing internal versus external support, this guide to outsourced revenue cycle management can help frame the decision. The best choice isn't always full outsourcing. Sometimes it's a hybrid model with tighter specialty oversight. What matters is measurable control over claims, cash, and accountability.
Frequently Asked Questions About RCM
What's the difference between medical billing and full revenue cycle management
Medical billing is one slice of the process. Full RCM includes eligibility, authorizations, charge capture, coding review, claim editing, submission, payment posting, denial work, patient collections, and financial reporting. If a practice only focuses on claim submission, it usually misses the front-end errors that cause denials in the first place.
Which KPI should a practice manager watch first
Start with first-pass clean claim rate, days in A/R, and denial rate. Those three metrics tell you whether claims are leaving cleanly, paying promptly, and returning with avoidable issues. After that, break performance down by payer and specialty-specific code families.
Is denial prevention more valuable than denial management
Usually, yes. Preventing a denial is cheaper and faster than correcting and appealing one after the fact. That's especially true when denials stem from technical issues like missing demographics, coding defects, modifier errors, or incomplete authorizations.
How should a practice vet an RCM vendor without getting distracted by AI claims
Ask for specialty-specific workflows, real operating examples, and clear accountability for claim outcomes. A credible partner should be able to discuss codes, modifiers, payer rules, remittance review, and denial root causes in detail. If the conversation stays at the level of automation, dashboards, and platform buzzwords, you're hearing marketing, not operations.
Happy Billing helps physician groups tighten revenue cycle performance without forcing an EHR migration. If your practice needs sharper denial prevention, specialty-specific billing support, or cleaner A/R execution in anesthesiology, mental health, cardiology, orthopedics, and other complex specialties, visit Happy Billing to see how a focused RCM partner approaches the work.