Mastering POS 21 in Medical Billing
POS 21 in medical billing designates Inpatient Hospital services for patients who are formally admitted, usually for an overnight stay or longer. It also determines the reimbursement pathway, including facility-based payment rules and, for Medicare, DRG bundled payment logic, so a simple POS error can turn a valid inpatient claim into an underpayment, denial, or audit problem.
The surprising part is how often practices lose money on POS 21 without realizing the root cause. Leaders tend to focus on CPT selection, modifier logic, and authorizations. But if the claim says the wrong place of service, the payer applies the wrong payment framework before it ever gets to the clinical nuance. In inpatient billing, that mistake hits harder because these claims sit in high-cost, high-scrutiny territory.
Procedural groups feel this most. An anesthesiology group can code the anesthesia CPT correctly and still create a denial if POS 21 conflicts with admission status or modifier use. A cardiology group can perform a hospital-based service on a patient who is physically in a procedural area and still need POS 21 because the patient’s status, not just the room, controls the billing outcome.
What Is POS 21 and Why It Matters for Your Bottom Line
POS 21 means Inpatient Hospital. It belongs on the professional or facility claim when services are furnished to a patient who has been formally admitted to the hospital and requires inpatient-level care.
That sounds basic. It isn't.
POS 21 acts like a reimbursement switch. It tells the payer that the service belongs in the inpatient hospital framework, not office billing, not outpatient hospital billing, and not emergency room billing. On CMS-1500 and UB-04 claims, that distinction affects how the payer evaluates the service, what edits fire, and whether the claim aligns with the admission record and hospital documentation.
Why finance teams should care
The financial stakes around inpatient billing are large. The shift toward POS 21 became more important alongside the Inpatient Prospective Payment System in 1983, and hospital expenses grew from $117 billion in 1990 to $1.3 trillion in 2022, according to the CMS place of service code set background. The same CMS-linked material also notes that a 2022 HFMA report found 12% of denials stemmed from POS inaccuracies, contributing to $265 billion annually in A/R leakage.
That’s why POS 21 belongs in the same conversation as denial prevention, charge capture, and clean-claim governance. If your team treats it as a clerical field, revenue leaks out long before anyone starts a formal appeal.
Practical rule: A correct CPT with the wrong POS still pays wrong, denies, or gets audited.
A strong revenue cycle management foundation has to control POS logic at the same level it controls diagnosis coding and modifier accuracy.
Where practices get hurt
The most common loss points aren't dramatic. They're routine:
- Admission-status mismatch: The physician billed an inpatient E/M, but the chart shows observation or outpatient status.
- Setting confusion: Staff sees “hospital” and assumes POS 21, even though the patient wasn't admitted.
- Late status updates: Admission changed after the encounter, but the claim wasn't corrected before submission.
- Procedure-first thinking: Teams focus on CPT codes such as 99231, 99232, 99233, or anesthesia coding details and miss the POS field entirely.
In other words, POS 21 is small on the claim and large in the ledger.
Correctly Identifying an Inpatient Hospital Setting
The mistake I see most often is confusing hospital location with inpatient status. POS 21 doesn't mean “the patient was in the hospital building.” It means the patient was a registered inpatient.

Think of POS 21 as a billing zip code. It routes the claim into a specific reimbursement system. If the patient is formally admitted, POS 21 tells the payer to process the service under inpatient rules. If the patient is in the ER and discharged, that route is different. If the patient is in outpatient surgery or observation, that route is different too.
The status test matters more than the room number
Use POS 21 when the record supports all of the following:
- Formal admission exists: There’s an inpatient admission order in the chart.
- Care extends beyond routine outpatient treatment: The stay is medically necessary and typically overnight or longer.
- Hospital resources are part of the service context: Nursing, surgical, diagnostic, or intensive inpatient resources support the episode.
- The claim aligns with the patient’s status for that date of service: Not what was expected. What was documented.
Under the billing guidance summarized in the inpatient hospital POS 21 explanation, POS 21 is reported on CMS-1500 or UB-04 claim forms to identify high-intensity inpatient care and trigger the correct reimbursement structure. That same source notes that, in major U.S. markets, inpatient hospital admissions under POS 21 represented about 34% of Medicare fee-for-service hospitalizations in 2020, totaling over 8 million stays, with average DRG payments exceeding $12,000 per case.
That’s exactly why payers scrutinize it.
For teams that need a refresher on where this field lives, the medical claim form guide is worth reviewing alongside your front-end and charge-entry workflow.
POS 21 versus POS 22 and POS 23
Here’s the clean operational distinction:
- POS 21 applies when the patient is an admitted inpatient.
- POS 22 applies when the patient receives hospital outpatient services but is not admitted as inpatient.
- POS 23 applies when the service belongs to the emergency room setting.
A useful example is a cardiology consult. If the cardiologist evaluates a patient after formal inpatient admission for acute illness or surgery-related management, POS 21 may be correct. If the same physician evaluates a patient in an outpatient hospital department before admission occurs, POS 22 is the safer answer. If the work happens during an ER encounter and the patient hasn't yet been admitted, POS 23 may be appropriate.
A hospital bed doesn't create inpatient status. The admission order does.
A simple verification sequence
Before the claim goes out, billing should confirm:
- Admission order date and time
- Patient class for the date of service
- Provider note tying the service to inpatient management
- CPT family consistent with inpatient care, such as hospital care or hospital discharge coding where applicable
- Modifiers and rendering details that match the specialty-specific service
If any one of those elements conflicts, stop the claim and resolve the status question first.
The Financial Impact of Facility vs Nonfacility Rates
The payer doesn't use POS only for location reporting. It uses POS to decide whether facility or nonfacility payment logic applies. That’s where many practices incur unnoticed financial losses.
Under AAPC’s discussion of CMS Transmittal 2563, POS 21 is the minimum required code when services are furnished to a registered inpatient, and the POS code determines whether the claim pays at the facility or nonfacility rate. The same guidance is blunt on the risk: if a practice misclassifies inpatient services with outpatient POS codes, the result is automatic underpayment. If the practice bills POS 21 for an outpatient service, the claim can deny.
What this means at the code level
Take physician E/M work. Codes such as 99231, 99232, and 99233 are hospital care services. Their payment context depends on the site-of-service logic tied to the claim. The same principle carries into diagnostic interpretation, consultations where applicable to payer policy, and physician professional services performed while the patient is an admitted inpatient.
That means your coders can't review CPT in isolation. They have to review:
- CPT code family
- patient class
- POS field
- date-of-service status
- payer-specific edits
If one piece breaks, the payment outcome breaks.
POS Code Impact on Reimbursement
| POS Code | Description | Typical Use Case | Reimbursement Implication |
|---|---|---|---|
| 21 | Inpatient Hospital | Physician services furnished to a registered inpatient | Applies facility rate logic and aligns with inpatient payment rules |
| 22 | Outpatient Hospital | Hospital-based care without formal inpatient admission | Using this for a true inpatient service can create automatic underpayment |
| 11 | Office | Professional services in a physician office setting | Using this for inpatient work can misstate the site of service and misprice the claim |
A disciplined RCM best-practices workflow should treat POS validation as a pre-bill edit, not a post-denial cleanup task.
Two expensive failure modes
The first is underpayment. Staff selects POS 22 because the service happened in a hospital department, but the patient had already been admitted. The payer prices the claim under the wrong logic. The claim may pay, but not correctly. Those are the hardest leaks to detect because they don't always show up as denials.
The second is hard denial. Staff bills POS 21 for a patient who was still outpatient or observation. The payer sees a mismatch between the claim and the hospital record and rejects it as inconsistent with place of service.
The dangerous claim isn't only the denied claim. It's the paid claim that paid under the wrong site-of-service logic.
What works in practice
Effective teams build edits around status verification before release. Weak teams rely on what the scheduler, provider, or encounter location “looked like” at the time. The first model protects cash. The second creates rework, appeal volume, and hidden underpayments.
Navigating POS 21 in Anesthesiology and Cardiology
Procedural specialties don't get tripped up on POS 21 because they don't understand the definition. They get tripped up because POS 21 intersects with modifier logic, unit reporting, procedural settings, and payer scrutiny all at once.
Anesthesiology risk points
In anesthesiology, the POS field has to line up with the rest of the professional anesthesia claim. That includes the anesthesia CPT, ASA base units, time units, and modifiers such as -AA and -QK. If that alignment breaks, the payer can treat the claim as improperly billed, duplicate the facility payment logic, or push it into audit review.
The specialty-specific warning is clear in the POS 21 procedural-specialty discussion. That source states that improper POS 21 pairing with base units can trigger 15-20% denial rates in high-stakes procedures, and anesthesiology inpatient claims with POS errors faced 18% higher audit flags compared to outpatient POS 11 in CMS 2025 reporting. It also notes a projected 12% rise in AI-driven audits targeting POS 21 in procedural specialties during 2025 to 2026.
A typical failure pattern looks like this:
- The case occurred during an inpatient stay.
- The anesthesia claim includes the correct anesthesia CPT.
- Time was reported.
- But the POS doesn't match inpatient status, or the modifier stack doesn't support the role of the anesthesiologist.
That combination invites denials and audit attention.
In anesthesiology, POS 21 isn't a standalone field. It's part of a four-part equation that includes CPT, units, and modifiers.
For groups running medical direction models, concurrency review should happen before claim release. If -QK is present, the file should also confirm that the status, timing, and provider role align with inpatient records. If the physician personally performed the service, -AA must be supported just as tightly.
Cardiology risk points
Cardiology gets messy for a different reason. The service may occur in a cath lab, procedural suite, or hospital department that staff instinctively associate with outpatient billing. But if the patient is already a registered inpatient, the physician’s professional service still points back to POS 21.
This is common around:
- Interventional cardiology procedures
- Inpatient consult follow-ups using 99231 to 99233
- Post-procedure management during admission
- Hospital-based diagnostic interpretation tied to inpatient status
The physical location can mislead coders. The patient may be in a procedural unit that looks outpatient from a workflow perspective, while the billing status is firmly inpatient.
For cardiology administrators trying to tighten this workflow, the operational issues overlap with broader cardiology revenue cycle management challenges such as hospital status tracking, procedural charge capture, and post-procedure documentation review.
What actually prevents leakage
The fix isn't more generic training. It’s targeted control points:
- Status pull from the hospital ADT feed or EHR
- Pre-bill logic that compares patient class against POS
- Modifier review for anesthesia claims
- Procedure-area exceptions list for cardiology and surgical services
- Manual audit on high-value inpatient cases before submission
Many groups fail at this stage. They audit denials after the fact instead of auditing status before the bill drops.
Common POS 21 Denials and How to Overturn Them
The fastest way to recover POS 21 revenue is to stop treating denials as “billing noise.” Most of these denials are traceable. If the team can identify whether the problem is status, code family, or documentation alignment, the appeal path is usually straightforward.
Denial pattern one with inconsistent place of service
Symptom on the EOB or portal: The payer indicates the service is inconsistent with the place of service billed.
What usually caused it: The patient was not formally inpatient on the date of service, or the claim used POS 22 or POS 11 when the patient was already admitted.
How to overturn it:
- Pull the admission order
- Confirm patient class for the exact date of service
- Compare the claim’s POS with the hospital registration record
- Submit a corrected claim if the original POS was wrong
- If the POS was correct, attach the admission documentation and provider note in the appeal
Denial pattern two with inpatient CPT but outpatient status
Symptom: The payer rejects the service because the CPT family doesn't match the reported status or setting.
This often shows up when a practice bills hospital inpatient E/M services such as 99231, 99232, 99233, or discharge management codes 99238 and 99239, but the underlying record reflects observation or outpatient care.
How to fix it: Reconcile the CPT family to the patient’s actual status first. If status was never inpatient, changing POS alone won't save the claim. The coding family may also need correction.
Fix the status conflict before you write the appeal letter. Otherwise you're defending the wrong claim.
Denial pattern three with missing support for specialty modifiers
This one is common in anesthesiology. The payer accepts that the patient was inpatient, but questions the professional claim because the units, modifier, and POS don't make sense together.
Look for these red flags:
- -AA reported, but documentation doesn't support personal performance
- -QK reported, but concurrency or medical direction support is incomplete
- Anesthesia time and POS point to inpatient care, but the claim lacks consistency across all fields
The cure is documentation assembly. Build the appeal with the anesthesia record, timing data, provider role support, and inpatient status proof.
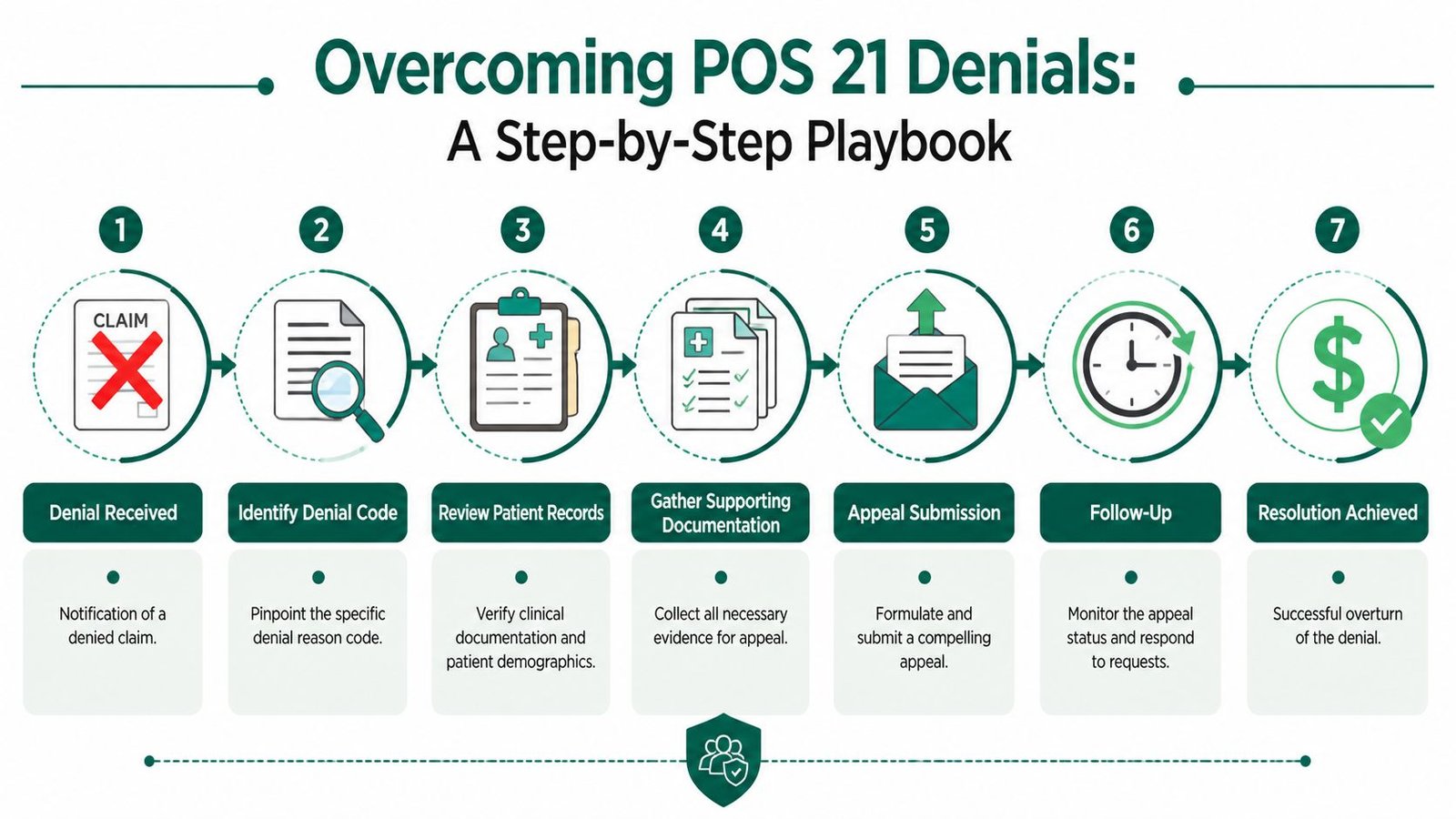
A practical appeal workflow
Teams that recover these claims consistently use a denial protocol, not one-off staff judgment:
- Read the denial text carefully
- Verify admission status on the date billed
- Review the CPT family and modifier set
- Compare claim data to chart data
- Correct and resubmit if the claim is wrong
- Appeal with documents if the payer is wrong
For practices struggling with rework volume, a tighter medical billing denial management process usually starts with denial categorization by root cause, not by payer alone.
Building a Leak-Proof Workflow for Inpatient Billing
Reactive denial work is expensive because every correction consumes labor after the claim should already have been paid. The better model is simple. Build controls that make a bad POS 21 claim hard to submit in the first place.

The minimum control set
A workable inpatient billing workflow has three checkpoints.
Front-end verification should confirm patient class as close to the date of service as possible. Schedulers and hospital liaisons shouldn't assume a planned admission became an actual admission.
Clinical documentation review should validate that the provider note supports inpatient management. If the record reads like outpatient or observation care, billing needs to stop and clarify before coding.
Pre-bill claim scrubbing should compare the POS against patient class, CPT family, and specialty-specific modifiers. For anesthesiology, that means checking units and modifier combinations. For cardiology, that means checking whether the patient was already inpatient when the procedure-area encounter occurred.
What strong teams do differently
Strong teams assign ownership.
- Registration or intake staff verify status.
- Providers document admission-linked care clearly.
- Coders select CPT and modifiers consistent with status.
- Billers run final edits against the claim and hospital record.
Weak teams spread responsibility so widely that no one owns the mismatch.
If nobody owns patient status verification, POS 21 errors become inevitable.
For a deeper dive into specialty workflows, see how complex inpatient and procedural claims are managed in cardiology billing operations.
A short audit checklist
Use this before claim release:
- Admission proof present
- Date-of-service status verified
- POS matches patient class
- CPT family fits inpatient care
- Modifiers support the physician role
- Discharge codes used only when documentation supports discharge work
- Any payer-specific rule exceptions documented
That checklist is more useful than a generic “quality review” because it targets the exact places where inpatient revenue leaks.
Frequently Asked Questions About POS 21
Is observation status billed with POS 21
No. Observation and outpatient status should not be treated as inpatient merely because the patient stayed in the hospital or occupied a bed. POS 21 is tied to formal inpatient admission status. If there’s no admission order and the patient remains observation or outpatient, billing POS 21 creates a status conflict that can trigger denial or repayment demand. The safest rule is to verify patient class in the hospital record for the exact date of service before coding the claim.
How should discharge services be billed for an inpatient stay
If the physician performs discharge management for a true inpatient discharge, the professional claim may use CPT 99238 or 99239, assuming documentation supports the discharge work performed. The key is consistency. The patient must be inpatient for that discharge date, and the provider note must support discharge management rather than a routine follow-up visit. If the patient was not inpatient, changing only the CPT or only the POS won't solve the claim issue.
Can a service performed in a hospital procedural area still use POS 21
Yes, if the patient is already a registered inpatient. This is a common source of confusion in cardiology, surgery, and anesthesiology. Staff often code based on the room or department where the service occurred. The payer, however, looks at patient status. A cath lab or procedural suite encounter can still require POS 21 when the patient was formally admitted before the service was rendered.
What should a practice do when a commercial payer applies its own POS rule
Start with the payer’s written policy and compare it to the patient’s status, the CPT family, and the claim form instructions. Some commercial plans apply edits differently from Medicare workflow, especially around hospital-based professional services. The safest process is to maintain a payer grid that lists POS requirements, accepted modifier combinations, and claim correction rules by plan. If a payer’s edit conflicts with the documented inpatient status, appeal with the admission order, hospital face sheet, and provider note that supports the billed service.
If your practice is losing time to inpatient denials, underpayments, or status-based claim rework, Happy Billing helps procedural and physician-led groups tighten POS logic, specialty coding, and denial prevention without forcing an EHR migration. Their team supports complex RCM workflows across high-stakes specialties, including anesthesiology and cardiology, with a model built around cleaner first-pass claims, faster A/R movement, and tighter control over revenue leakage.