Medical Claim Form: A Guide to Flawless Submissions
If you're dealing with repeat denials for something as simple as subscriber ID, diagnosis linkage, or a missing modifier, the medical claim form is the problem to fix first. It's the document, or electronic equivalent, that decides whether your practice gets paid correctly, gets paid late, or gets forced into rework that clogs A/R.
Practice managers usually don't need another generic explanation of boxes and fields. They need to know which entries break claims, which CPT and modifier combinations deserve extra scrutiny, and how to stop form errors from turning into cash flow problems.
The Critical Role of the Medical Claim Form
A medical claim form is your standardized bill to the payer. For physician and allied health services, that usually means the CMS-1500. For facility billing, it usually means the UB-04. Either way, the form is where patient demographics, diagnosis codes, procedure codes, provider identifiers, and charges get translated into payment.
That sounds administrative. It isn't. It is operational finance.
The U.S. medical claims market processes over 10 billion claims annually, which makes claims submission one of the largest transactional workflows in healthcare, according to Grand View Research's U.S. medical claim market benchmarking. At that volume, payers don't review claims like a human accountant reading an invoice. They apply automated edits first. If your medical claim form has bad data, the claim fails before anyone evaluates medical necessity or contract reimbursement.
What the form controls in real life
A flawed claim form usually creates one of three outcomes:
- Rejected claims: The payer or clearinghouse kicks the claim back for formatting or data mismatch issues.
- Denied claims: The payer accepts the claim into adjudication, then denies payment.
- Underpaid claims: The payer processes the claim, but the coding or modifier setup leaves money on the table.
In each scenario, the same practice has to spend staff time correcting work it already did once.
Practical rule: If the same denial reason appears more than once in a week, stop treating it as a one-off and audit the workflow that feeds the claim.
Why managers should care before billers do
Front office mistakes often show up as billing problems. A misspelled patient name, inactive plan, or wrong subscriber relationship can start at check-in and surface days later as a denial. Billing teams then waste time working denials that should've been prevented upstream.
That's why clean claim discipline matters. If you need a sharper operational definition, this overview of what a clean claim means in medical billing is the right benchmark. The medical claim form is where that benchmark gets won or lost.
CMS-1500 vs UB-04 The Two Pillars of Billing
Most physician owners know both forms exist. What often causes confusion is who should bill on which form when the patient encounter involves both the physician and the facility.
The shortest answer is this: CMS-1500 is for professional billing. UB-04 is for institutional billing. One describes the clinician's service. The other describes the facility's resources.
The practical distinction
Think of the CMS-1500 as the surgeon's or anesthesiologist's invoice for professional work. Think of the UB-04 as the hospital or ASC bill for the room, staff, supplies, and facility overhead tied to that encounter.
A single surgery can generate both forms without any duplication. That's normal.
For example, an orthopedic surgeon billing CPT 27447 for total knee arthroplasty generally bills the professional service on the CMS-1500. The hospital or ambulatory surgery center bills the institutional side on the UB-04. An anesthesiologist may separately bill anesthesia services on a CMS-1500 using the relevant anesthesia CPT and modifiers such as AA, QK, QX, or AD, while the facility still bills its own charges on the UB-04.
CMS-1500 vs. UB-04 At a Glance
| Attribute | CMS-1500 (Professional) | UB-04 (Institutional) |
|---|---|---|
| Primary use | Physician and allied health professional services | Hospital, facility, and institutional services |
| Typical biller | Physician group, independent practice, clinician | Hospital, ASC, facility, institutional provider |
| Focus | Who performed the service and what was done | Where the service occurred and facility resources used |
| Common coding elements | ICD-10-CM, CPT, HCPCS, modifiers, NPI | Diagnosis and institutional billing elements tied to facility reporting |
| Typical examples | Office visit 99213, psychotherapy 90837, interpretation with modifier 26 | Hospital stay, surgery center facility claim, outpatient facility charges |
| Common risk if misused | Professional service billed on wrong claim type or missing physician detail | Facility service missing institutional data or submitted through wrong channel |
Where managers get tripped up
The mistake isn't usually choosing the wrong form in isolation. It's failing to coordinate the professional and institutional stories so they align.
A few examples:
- Date mismatches: The surgeon bills one date of service and the facility bills another.
- Provider mismatch: The rendering provider on the professional claim doesn't match the documented operative or procedural record.
- Place of service confusion: The physician claim uses a place of service that conflicts with the facility record.
- Component billing errors: Cardiology and imaging groups bill a full test globally when they only performed the professional interpretation and should have appended modifier 26. If the facility owns the technical equipment and staff, the technical side typically belongs elsewhere, often with modifier TC on the appropriate claim.
If a payer sees two claims that describe the same event differently, it usually doesn't ask which one is right. It suspends, rejects, or denies until someone fixes it.
For practice managers overseeing physician billing inside a hospital or ASC environment, that's the key distinction. The CMS-1500 and UB-04 aren't competing forms. They're parallel billing tools, and your revenue depends on keeping them consistent.
Anatomy of a Perfect CMS-1500 Claim
Monday morning, a 20-claim batch clears your scrubber. By Friday, several of those claims are sitting in rejection or pended status for reasons that had nothing to do with medical necessity. One ortho postop visit used the wrong diagnosis pointer with modifier 24. One anesthesia line carried the wrong staffing modifier. One established patient visit had a subscriber ID that no longer matched the payer file after a plan rollover. The form looked complete. Cash still stalled.
That is the operational problem with the CMS-1500. Small field-level mistakes create front-end rejections, line-item denials, and quiet underpayments that sit in A/R until someone audits the remittance.
If your team needs a visual reference for staff training, this completed CMS-1500 form example helps. A usable training tool, however, is not the same as a clean claim standard. Managers need to know which boxes drive edits, pricing, and medical review.
Demographics and insurance fields decide whether the claim gets in the door
Boxes tied to patient and subscriber identity are still one of the fastest ways to create preventable rejections. Legal name, date of birth, sex, member ID, and relationship to insured must match the payer record closely enough to pass front-end validation.
The usual failure patterns are familiar:
- Nickname or shortened first name
- Member ID carried over from a prior plan year
- Subscriber and patient reversed
- COB issues caused by outdated address or policy order
- Inactive coverage because eligibility was not rechecked before the visit
A group can code a straightforward 99213 correctly and still get paid nothing if registration fed the wrong subscriber record into the claim. For many practices, fixing front-desk insurance discipline improves first-pass acceptance faster than another coder education session.
Provider identifiers matter more on specialist and ordered services
Specialty claims break when the provider fields do not match the chart, the referral, or the ordering record. The service may be documented correctly and still reject because the claim tells the payer the wrong provider story.
Practice managers should audit these situations closely:
- Cardiology diagnostics tied to an outside referral or ordering physician
- Pain procedures where the order and rendering provider must align
- Orthopedic consultations where payer policy expects referring provider data
- Behavioral health claims billed under a group but performed by an individual servicing clinician
A missing or misplaced NPI can stop the claim before the payer evaluates the CPT code. That is a workflow issue, not a coding issue, and it usually sits between scheduling, credentialing, and charge entry.
Box 21 and Box 24E control medical necessity at the line level
Diagnosis reporting is not just an ICD-10 list. It is the logic that connects each service line to a payable reason. CMS notes in its professional paper claim form guidance that fields 24A through 24J must be completed accurately. Errors in diagnosis pointers drive a large share of avoidable initial denials, and inaccurate modifier or unit reporting can also lead to underpayment.
Box 21 lists the diagnoses. Box 24E tells the payer which diagnosis supports each CPT or HCPCS line. If that pointer is wrong, the payer can read the service as unsupported even when the chart is fine.
A common orthopedic failure looks like this. The surgeon bills a postoperative office visit during the global period with modifier 24 because the visit is unrelated to the surgery. The coder appends the modifier correctly, but Box 24E points back to the postoperative diagnosis instead of the new unrelated condition. The payer sees a global visit and denies it. The note may support payment, but the form does not.
Use the same line-by-line logic on other services:
- A joint injection should point to the diagnosis that supports the injection, not a secondary chronic condition that happened to be listed.
- A diagnostic study should point to the symptom, condition, or follow-up diagnosis that justifies the test.
- An unrelated E/M service in a global period should point to the diagnosis that supports modifier 24, not the original surgical diagnosis.
Audit Box 24E at the service-line level. Many teams verify that diagnoses exist on the claim. Fewer verify that each line points to the diagnosis the payer expects for that exact service.
Box 24D and Box 24G are pricing fields, not just coding fields
Box 24D carries the CPT or HCPCS code and modifiers. Box 24G reports units. Those two fields often decide whether the claim pays correctly, partially, or below contract.
The trade-off is simple. Template-driven charge entry is faster, but it creates expensive mistakes in specialties where modifiers and units control payment logic.
Anesthesia is the clearest example. If the claim reports the correct anesthesia CPT but the wrong modifier in 24D, reimbursement can change even if the payer does not deny the claim. A line billed with AA tells the payer the anesthesiologist personally performed the case. A line billed with QK, QX, or QY tells a different medical direction story. If the staffing pattern in the record does not support the modifier sequence on the claim, payment can be reduced or flagged for review.
The same issue shows up in 24G. Units must match the billable unit structure supported by the record. In anesthesia, that means time and reporting logic must reconcile. In infusion or repeated service billing, incorrect units can create overbilling exposure or short-payments that erode margin one claim at a time.
What a clean CMS-1500 looks like in practice
A clean claim has internal consistency. Every field supports the same financial and clinical story.
Use this pre-submit standard:
- Patient and subscriber data match eligibility exactly.
- Billing, rendering, and referring provider data match the documentation and payer requirements.
- Each CPT or HCPCS line points to the correct diagnosis in 24E.
- Modifiers reflect the actual service circumstance, not a default template.
- Units in 24G match the record and the specialty's billing rules.
- Dates, charges, and place of service reconcile to the encounter documentation.
Teams that hold the CMS-1500 to that standard reduce more than denials. They cut rework, catch underpayments earlier, and shorten the path from claim submission to cash.
Specialty-Specific Nuances That Cause Denials
A surgery center closes the month with strong volume, yet cash still slips. The issue is not claim volume. It is specialty logic missed at the claim line level. An anesthesia modifier sequence does not match the staffing record. A post-op ortho visit is billed outside the global package without support. A cardiology study is billed globally even though the group only read the test. Each error looks small. Each one delays payment or creates a take-back.
Generic CMS-1500 guidance does not fix that kind of denial. Specialty claims fail for specialty reasons, and practice managers usually see the impact first in rising A/R, avoidable appeals, and staff time lost to rework.
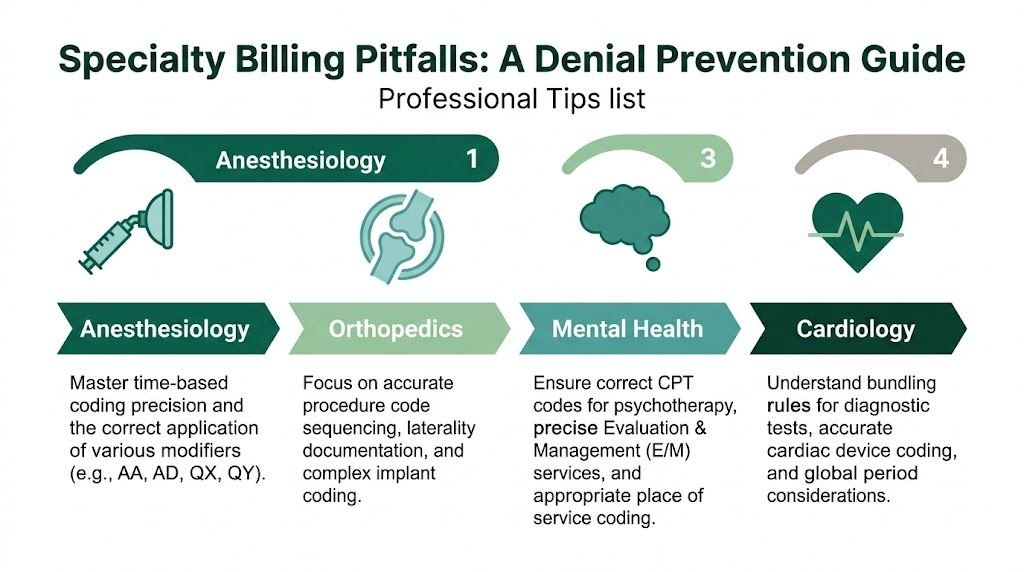
Anesthesiology
Anesthesia denials usually start where the clinical timeline and the claim line stop matching.
The risk points are familiar: 24D modifiers such as AA, AD, QK, QX, and QY, plus 24G units that must reconcile to the anesthesia record. If the record shows medical direction but the claim is built as personal performance, the payer has a clear reason to reduce or deny. If the minutes support one unit total and the submitted units show another, the claim can trigger both payment delay and audit exposure.
Physical status reporting can create another problem. If your payer expects a physical status modifier and the documentation supports it, omission can reduce reimbursement. If the modifier is added by habit without support in the record, the line becomes harder to defend.
I audit these claims by asking one question first: does the claim tell the same timeline as the anesthesia record? If the answer is no, the denial is usually justified.
If your team is tightening edits around specialty workflows, the operational issues outlined in this guide to revenue cycle technology for specialty claim editing and denial control are the right place to start. For a specialty-specific benchmark, the anesthesiology billing team page reflects the kind of operational focus these claims require.
Orthopedics
Orthopedic claims often go out with the correct CPT and still come back unpaid.
The problem is usually global surgery logic. Take 27447 for total knee arthroplasty. The surgery may be coded correctly on day one, but follow-up services during the 90-day global period need a separate review. A post-op visit tied to routine recovery belongs in the global package. An E/M service for a new, unrelated problem may support modifier 24, but only if the note makes that separation obvious.
Orthopedic denials also show up in these situations:
- Modifier 25 is attached to a same-day E/M without documentation that supports a significant, separately identifiable service
- laterality does not match across the operative note, diagnosis coding, and claim line
- multiple procedures are billed without correct sequencing or without handling NCCI edit risk
- fracture care, follow-up imaging, and cast or strapping charges are submitted without clear documentation of what is included versus separately billable
Margin gets squeezed. A denied post-op E/M is not just one missed payment. It creates chart pulls, coder review, appeal work, and slower follow-up on higher-value claims.
Mental health
Behavioral health denials are often blamed on authorization, but claim construction still drives a large share of avoidable rejections.
Codes such as 90834 and 90837 look straightforward until the submitted claim conflicts with payer setup. The wrong place of service, the wrong rendering clinician, or a mismatch between the authorization and the billed service is enough to stop payment. Telehealth has made this more sensitive because payers may require specific POS reporting, modifier use, or both.
Practice managers should review:
- place of service for office, telehealth, and facility encounters
- rendering provider identity versus the credentialed clinician who performed the service
- authorization details such as dates, units, and service type
- diagnosis coding that supports the treatment plan and billed service level
Psychiatry groups that bill both psychotherapy and E/M have another exposure point. If the documentation supports only therapy, billing an E/M in addition to psychotherapy invites denial and recoupment risk.
Cardiology
Cardiology claims break down where testing, interpretation, and ownership split.
A common example is diagnostic studies billed without a clean distinction between the professional and technical components. If the group provides only the interpretation, the claim may require modifier 26. If the group owns the equipment and provides the technical portion, TC may apply. Billing the service globally when the practice performed only one component creates an easy denial and can trigger refund requests after payment.
Other pressure points include:
- stress tests, echo studies, and vascular studies billed with the wrong component structure
- device interrogation or monitoring claims submitted without documentation that supports the billed service level
- procedure combinations that hit bundling edits because the coding team did not review NCCI logic before submission
- diagnosis coding that supports medical necessity for the test ordered, but not for the test billed
Cardiology groups feel these mistakes quickly because diagnostic volume is high. A small component-billing error repeated across a large batch of claims turns into a measurable cash flow problem by month-end.
What reduces denials in specialty billing is not generic advice. It is claim edits built around the CPTs, modifiers, global periods, component rules, and authorization rules that apply to the specialty submitting the form.
Electronic vs Paper Submission The 837P Transaction
The red CMS-1500 still dominates training manuals and desk references, but most practices don't submit paper forms anymore. What they submit is the electronic version of that same professional claim data.
For professional claims, the electronic standard is the ASC X12 837P (005010X222A1) under HIPAA. CMS ties the paper CMS-1500 to that electronic structure in its professional claim guidance. In practical terms, the paper form is the visual layout your staff recognizes. The 837P is the machine-readable transaction payers and clearinghouses process.
Think of it like file format, not different content
The simplest way to explain it to staff is this:
- The CMS-1500 is the print view.
- The 837P is the structured data file.
The diagnosis pointer logic, rendering provider data, CPT lines, modifiers, and units still have to be right. They move through loops and segments instead of appearing only in boxes on paper.
What the clearinghouse actually does
A clearinghouse isn't just a digital mailbox. It validates, reformats, and routes your claim file before the payer sees it. If the claim fails front-end edits there, you get a rejection faster than you would through manual payer handling.
That's why electronic submission improves control. The billing team can catch:
- invalid subscriber formatting
- missing NPIs
- diagnosis pointer mismatches
- modifier conflicts
- payer-specific formatting issues
before the claim sits unresolved in a payer queue.
A strong technology stack matters here. If you're evaluating workflow improvements, this overview of technology for revenue cycle operations gives a practical frame for how clearinghouse edits, PM systems, and billing controls should work together.
The 837P doesn't forgive bad claim logic. It exposes bad claim logic faster.
A Proactive Denial Prevention Checklist
Denial management starts long before a denial exists. The most reliable fix is to decide who owns prevention at the front desk and who owns it inside billing, then make both teams accountable.
If your current workflow is too reactive, this guide to medical billing denial management helps map the downstream process. Prevention still has to happen upstream.
Front office checklist
Front office errors often become "billing denials" that billing never really caused.
- Verify eligibility on every visit: Don't rely on last month's active coverage.
- Capture legal demographic data exactly: Use the payer-facing name, DOB, subscriber ID, and relationship as shown in eligibility.
- Confirm referral and ordering requirements before service: This matters for specialist and diagnostic claims.
- Check authorization status against the scheduled service: Especially important in behavioral health, high-cost diagnostics, and procedures.
- Match place of service to the actual encounter setting: Office, facility, and telehealth distinctions matter on the final claim.
- Flag registration discrepancies before checkout: Fixing them same day is easier than fixing rejections later.
Billing team checklist
Billing owns the last line of defense. That means reviewing for logic, not just speed.
- Scrub provider data: Billing provider, rendering provider, and referring provider fields should match documentation and payer expectations.
- Audit diagnosis pointers line by line: Especially in Box 24E logic for procedures, tests, and multi-diagnosis encounters.
- Review modifiers against documentation: Examples include 24, 25, 26, TC, AA, AD, QK, QX, and QY.
- Confirm units before submission: This is critical for anesthesia and any repeated service billing.
- Check global-period logic: Orthopedic and procedure-heavy groups should review postoperative E/M claims carefully.
- Validate charge entry against the note: CPT, date of service, units, and place of service all need to align.
- Monitor payer-specific edits by denial reason: If one payer repeatedly rejects the same field, build a front-end rule for it.
What doesn't work
Practices lose time when they rely on these habits:
- Posting denials and moving on: That tracks the problem but doesn't stop recurrence.
- Appealing weak claims: If the original form logic was wrong, the appeal usually just extends the cycle.
- Using one-size-fits-all charge review: Specialty claims need specialty edits.
- Trusting templates blindly: Templates help speed. They also replicate mistakes at scale.
A denial prevention checklist only matters if someone reviews it against actual claims each week. Otherwise, it becomes another document nobody uses.
From Claim Form to Cash Flow The RCM Partner Advantage
A strong medical claim form process doesn't just reduce clerical mess. It protects revenue timing.
When a practice gets claim construction right from registration through coding and submission, cash comes in with fewer interruptions. When it gets claim construction wrong, staff spend their days chasing eligibility fixes, corrected claims, missing modifiers, and appeal letters instead of managing growth.
That operational burden gets heavier in specialties where claim logic is unusually technical. Anesthesia groups need unit and concurrency discipline. Orthopedics needs global-period control. Cardiology needs precise component billing. Behavioral health needs authorization and provider-match rigor. Most in-house teams can do some of this well. Fewer can do all of it consistently while payer edits keep changing.
For many physician owners, the decision isn't whether billing matters. It's whether the organization has the time, oversight, and specialty knowledge to keep claim quality high every day. A dedicated RCM partner can enforce that discipline with tighter pre-submit edits, clearer work queues, and better follow-up rules.
If you're evaluating that model, this overview of RCM for physician practices is a practical starting point. The right partner should improve claim quality before submission, not just promise to clean up denials after the fact.
Frequently Asked Questions
What is the most important field on a medical claim form?
There isn't just one, but Box 24E on the CMS-1500 deserves special attention because it links each CPT or HCPCS line to the diagnosis that supports medical necessity. If that pointer is wrong, the claim can fail even when the diagnosis list and procedure code are both technically valid on their own.
In day-to-day operations, though, the biggest troublemakers are usually a combination of patient identity fields, provider fields, diagnosis pointers, modifiers, and units. The highest-value audit approach is to review the claim as a chain of logic, not a set of isolated boxes.
When should a practice use modifier 24 on the CMS-1500?
Use modifier 24 when the provider bills an unrelated E/M service during a postoperative global period. The key word is unrelated.
For example, an orthopedic surgeon who performed 27447 may later see the patient for a separate issue that isn't part of routine postoperative care. If the documentation supports that distinction, modifier 24 may be appropriate on the E/M line. If the visit is routine follow-up for the surgery, billing it separately will usually create denial risk.
Why do anesthesia claims get underpaid even when they aren't denied?
Because underpayment often comes from modifier and unit logic, not just medical necessity denial. If the claim uses the wrong anesthesia modifier, reports units inaccurately, or doesn't reflect the actual provider participation documented in the record, the payer may still process the claim and pay less than expected.
That's why anesthesia managers should reconcile the anesthesia record, staffing model, modifiers such as AA, AD, QK, QX, and QY, and the units reported in 24G before submission.
What should a practice do when electronic claims keep rejecting at the clearinghouse?
Don't just resubmit repeatedly. Start by identifying whether the rejection is tied to formatting, provider enrollment data, subscriber mismatch, diagnosis pointer logic, or a payer-specific rule. Then trace the issue to the source workflow.
A useful triage sequence is:
- Check registration data first
- Confirm provider identifiers and enrollment status
- Review CPT to diagnosis linkage
- Inspect modifiers and units
- Test whether the issue is payer-specific or system-wide
If the same clearinghouse rejection appears repeatedly, build a front-end edit in the PM system or claim scrubber so staff stop creating the same bad file.
Happy Billing helps physician practices turn claim quality into faster cash flow. If your team is dealing with recurring denials, underpayments, or specialty-specific billing complexity, Happy Billing provides full-cycle RCM support built for anesthesia, cardiology, orthopedics, mental health, and other high-stakes specialties.