CPT Code for Wound VAC: A Guide to Financial Impact
A surgeon finishes a wound VAC visit, the patient is treated correctly, and the chart closes. Thirty days later, the claim is denied or paid below expectation because the note did not clearly support the device type or wound size. The clinical work was real. The revenue loss was real too.
The CPT code for wound VAC often looks simple on the surface. In practice, small coding mistakes around 97605, 97606, 97607, and 97608 create a predictable financial drag. I see it in wound programs that stay full but still produce disappointing collections, rising rework, and avoidable write-offs.
For the physician-owner, this is a margin problem before it is a coding problem.
Negative pressure wound therapy billing turns on two facts: what kind of system was used and the total wound surface area treated. If either point is vague in the documentation, the billing team starts making judgment calls. That leads to two expensive outcomes. The claim gets denied because support is missing, or the service is billed conservatively and the practice gives up reimbursement it had every right to collect.
That pattern rarely shows up as one dramatic error. It shows up as a hundred small losses across repeat visits, multiple providers, and several payer policies. Over time, wound VAC coding becomes one of those quiet revenue leaks that owners feel in cash flow and A/R long before they see it in a report.
The goal here is straightforward: explain the billing rules in a way that helps you protect revenue, reduce denials, and spot where your current workflow is costing the practice money.
Your Guide to CPT Codes for Wound VAC Therapy
The billing framework for wound VAC therapy is narrower than most practices assume. The four primary CPT codes are 97605 and 97606 for NPWT using durable medical equipment, and 97607 and 97608 for disposable, non-durable systems. The split within each pair is the same: total wound surface area at or below 50 cm² versus more than 50 cm².
That sounds straightforward. In actual revenue cycle work, it often isn't.
Practices lose money on wound VAC claims in three common ways. First, they code the wrong device family. Second, they fail to capture total wound area clearly enough for the billed code. Third, they report NPWT in situations where the payer considers it part of routine dressing care rather than a separately payable service. Each one produces a different financial problem: underbilling, denial, or rework.
Practical rule: If your providers can't tell from the note whether the system was durable or disposable, and your billing team can't verify total wound area from the same encounter, you're relying on guesswork for payment.
For practice owners, this isn't reference material. It's operating margin. A wound service line can look productive on the schedule while leaking reimbursement in the back office. That's especially true in surgical groups and high-volume wound programs where repeated NPWT encounters stack up quickly. Practices with complex procedural workflows, including those in wound debridement billing scenarios, need this logic embedded in the visit workflow, not fixed later in A/R.
The Four Primary CPT Codes for Wound VAC Therapy
CMS billing guidance lays out the coding split clearly in its Medicare MLN article on NPWT coding. 97605 is for NPWT using durable medical equipment when the total wound surface area is 50 cm² or less. 97606 applies when the wound area is greater than 50 cm². For disposable, non-durable NPWT, 97607 applies when the total wound surface area is 50 cm² or less, and 97608 applies when it is greater than 50 cm².
The same CMS guidance also states that the disposable codes are per-session codes and include wound assessment and instructions for ongoing care. That matters financially because it defines what is already built into the code and helps you avoid billing logic that payers won't accept.
Wound VAC CPT code quick reference
| CPT Code | Device Type | Wound Size (Total Area) | Practice Revenue Note |
|---|---|---|---|
| 97605 | Durable medical equipment | ≤ 50 cm² | Correct when a DME system is used on smaller total wound area. If your note supports a larger area, this code leaves revenue behind. |
| 97606 | Durable medical equipment | > 50 cm² | Supports payment for larger total wound area with DME. Missing measurements often cause practices to bill lower than documentation should support. |
| 97607 | Disposable, non-durable NPWT | ≤ 50 cm² | Appropriate for smaller wounds with disposable systems. Using the wrong device family can trigger avoidable payer questions. |
| 97608 | Disposable, non-durable NPWT | > 50 cm² | The right code when disposable NPWT is used and the total area exceeds the threshold. This is where documentation gaps often turn into underpayments or denials. |
What owners should actually watch
The coding choice is driven by only two variables. That simplicity is useful because it gives you a short audit checklist for your own practice:
- Device verification: Was the system documented as durable or disposable?
- Area verification: Was the total wound surface area documented clearly enough to support the code?
- Single code logic: Did the billing team select the code based on the total treated area rather than treating each wound like a separate billing opportunity without support?
- Claim consistency: Does the clinical note match what was billed on the claim line?
A physician-owner doesn't need to inspect every encounter. But you should sample them. Pull a handful of paid and denied NPWT claims and compare the note against the code. If you see staff defaulting to the lower size code, coding from memory, or coding before measurements are finalized, that isn't a training issue alone. It's a revenue control failure.
DME vs Disposable Systems A Critical Revenue Fork
A physician-owner usually sees the problem after the money is already gone. The note says "wound vac change." The claim goes out with the wrong CPT family, or billing has to stop and chase the chart, the supply log, and the clinical team for clarification. One vague device entry can turn a straightforward NPWT encounter into avoidable rework, delayed cash, or a denial that should never have happened.

The financial fork is simple. A durable medical equipment NPWT system and a disposable NPWT system do not live in the same CPT family. Once the wrong device type is documented, charge capture drifts off course. Staff then try to repair the claim downstream, which is one of the most expensive places to fix a problem.
Owners should care because this is not a coder-only issue. It affects how your practice buys supplies, how nurses and MAs document the visit, how providers sign notes, and how quickly claims leave the queue. If any one of those steps uses different terminology for the same device, collections get less predictable.
Why practices lose money here
The common failure pattern is operational, not clinical. The provider performs appropriate care, but the chart does not clearly state whether the system was durable or disposable. Billing then guesses, defaults to a familiar code set, or holds the claim. None of those options are good for revenue.
The strongest wound care groups build one rule into the workflow. The procedure note must identify the device family before the encounter can be billed. That sounds small. In practice, it separates clean claims from claims that require chart audits and appeals.
A reliable process usually includes:
- One device naming standard: Clinical staff, purchasing, and billing use the same terms for durable and disposable NPWT systems.
- Template hard stops: The note requires device type selection before signature.
- Pre-bill validation: The selected CPT family is checked against the documented device before claim submission.
- Exception routing: If staff cannot confirm the device from the note, the claim goes back to the rendering team immediately instead of reaching A/R with a preventable error.
A wound VAC claim should be built from the procedure note, not reconstructed from memory and supply records.
That is the business case for tighter NPWT controls. A small documentation gap at the visit level multiplies into staff time, slower cash, and lower confidence in your wound care margin.
Practices that need specialized wound care billing support usually do not have a volume problem. They have a process control problem between the treatment room and the claim file. The same logic applies to records workflow more broadly. Groups that automate clinic documents with Zenfox.ai often reduce the back-and-forth that causes these coding mismatches in the first place.
Documentation That Defends Your Claims
A physician-owner usually sees the denial on the back end. The primary mistake happened much earlier, in a note that never gave billing enough to defend the code. With wound VAC claims, small omissions create expensive downstream work. A missing measurement, an undocumented device type, or a vague wound description can turn a payable service into rework, delay, or write-off.
For provider-applied NPWT, the claim has to stand on its own. Payers expect the record to show what was treated, how large it was, and what system was used. If your note forces a biller to guess, your revenue cycle is already exposed.
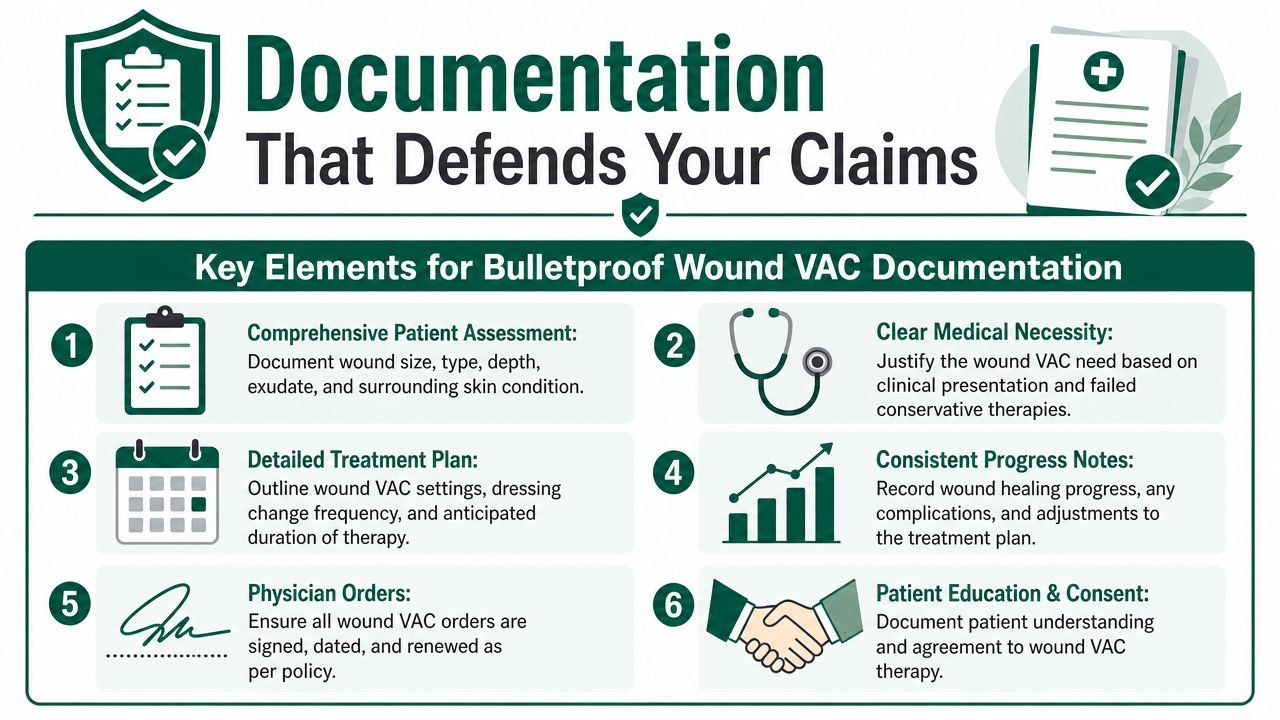
The minimum documentation standard
A defensible wound VAC note should answer the payer's questions without an appeal letter. At minimum, document:
- Wound dimensions: Record length and width in centimeters for each wound treated.
- Total surface area: If multiple wounds are treated in the same encounter, calculate the combined area used to support code selection.
- Device type: State whether the NPWT system was durable or disposable.
- Wound status: Describe the wound clearly enough to support medical necessity and code selection.
- Treatment details: Include the assessment, application details, and follow-up plan when those elements support the reported service.
- Diagnosis-to-procedure alignment: The diagnosis, wound description, and procedure note should support the same clinical story.
In this scenario, practices lose money. The chart may be clinically acceptable and still be weak for billing.
I see this often in multi-location groups. One provider documents measurements in the procedure note, another leaves them in a nursing flowsheet, and a third copies forward last week's size. Billing then spends time stitching together support that should have been obvious in one signed encounter. That is not a coder training issue. It is an operating model issue.
The fix is practical. Build the template so wound size, total area, and device type are captured in one predictable location before the note can close. If note variation is a problem across surgeons or clinics, tools that help automate clinic documents with Zenfox.ai can reduce record inconsistency before it reaches charge entry.
The note should answer the payer's question before the claim is sent.
Practice owners should also audit whether wound VAC encounters reach billing as a clean claim with complete supporting documentation. If wound measurements, device classification, and treatment details are not standardized before charge release, your denial team is absorbing preventable labor and your cash flow is paying for it.
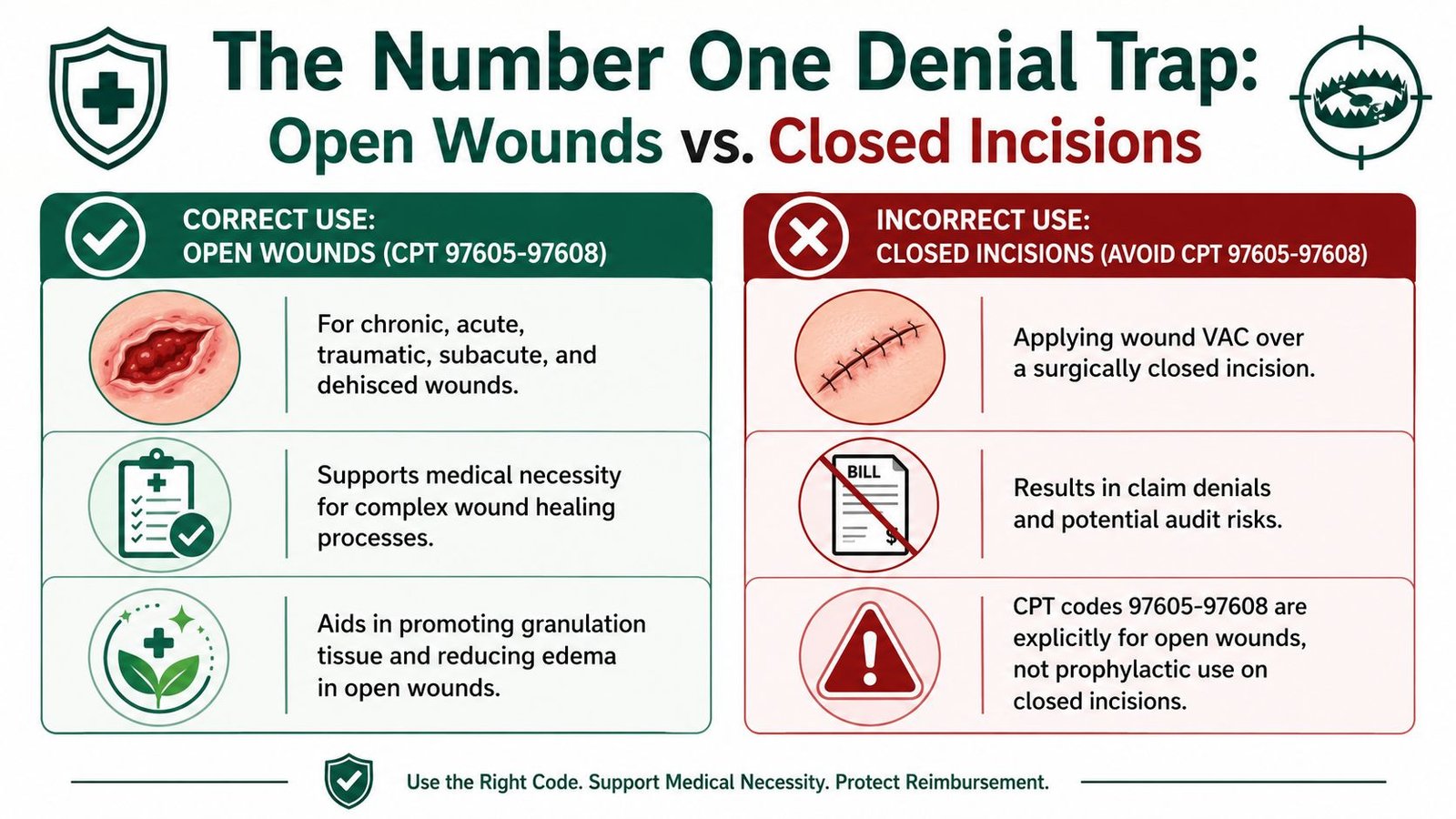
The Number One Denial Trap Open Wounds vs Closed Incisions
One rule causes more wound VAC confusion than almost anything else. Codes 97605 through 97608 are reportable only when the VAC is placed at an open wound site. If the device is used as a dressing over a closed surgical incision, billing guidance treats that as dressing care, not separately billable NPWT.
That distinction is spelled out in published wound VAC billing guidance. It states that wound VAC billing is not separately reportable when the device is used over a closed surgical incision, and that inappropriate reporting can trigger denials when documentation doesn't clearly show the wound remained open.
Why this mistake keeps costing practices money
A surgeon may clinically think, "We used a VAC." The payer asks a different question: "Was this an open wound or a closed incision?" If the chart doesn't answer that clearly, the claim is exposed.
Owners should challenge internal assumptions. If your billing staff tells you a wound VAC claim denied as bundled, ask one question first: was the therapy applied to an open wound, or was it placed over a surgically closed incision? That single distinction often explains the denial faster than any remittance code discussion.
The operational fix
Build a hard stop into documentation and charge entry:
- Require wound status: The note should identify whether the wound remained open.
- Avoid generic postoperative language: "VAC applied" is not enough.
- Review denial patterns: If bundled denials repeat, compare the underlying op note and procedure note.
- Escalate trend lines: Repeated denials of this type belong on your management dashboard, alongside your broader top denial categories in medical billing.
A practice that gets this rule wrong doesn't just lose one claim. It trains its staff into a repeatable denial pattern. That is how a technical coding misunderstanding turns into an ownership-level financial problem.
Navigating Modifiers and ICD-10 Pairings
Once the CPT code is right, the next issue is support. The payer still needs to understand why the service was necessary and whether anything billed on the same date is distinct enough to stand on its own. That's where modifiers and diagnosis pairing become financially important.
The problem for owners is that modifier misuse can create opposite failures. Some teams underuse them and accept avoidable bundling denials. Others overuse them and create audit risk. Neither approach is healthy for cash flow.
Modifier discipline matters
A common wound-care scenario is debridement performed on the same date as NPWT application. In some cases, a modifier such as 59 may be necessary when the services are distinct and separately supported in the record. But this isn't a modifier to use casually. If your team cannot point to separate work, separate documentation, and payer-acceptable rationale, the modifier won't rescue a weak claim.
If you want your physicians and administrators aligned on what that modifier is meant to do, review this practical guide to CPT modifier 59. It helps frame the issue the right way: as a compliance and reimbursement decision, not a shortcut around edits.
If your staff uses modifiers to "get claims through," you'll eventually pay for that in rework, refunds, or audit response time.
Diagnosis pairing should prove medical necessity
For wound VAC billing, the ICD-10 side should be specific enough to explain the wound condition being treated. The exact diagnosis code selection depends on the patient's documented condition, and that should be verified in the chart and against payer policy before claim submission. If your organization uses broad or unspecified diagnosis coding out of habit, expect more medical-necessity friction.
This matters even more in specialties with high procedural volume and postoperative complexity. Groups dealing with fractures, wound complications, and staged healing issues, such as those using orthopedic billing support, often see that the cleanest NPWT reimbursement comes from close alignment between procedure documentation, diagnosis specificity, and same-day service logic.
Owners don't need to memorize diagnosis options. You do need to ask whether your billing team is validating diagnosis specificity before the claim leaves the door. If they aren't, you're waiting to find out on the ERA.
How to Handle Common Payer Denials for Wound VAC
A common pattern looks like this. The physician documents good care, the patient improves, and the claim still comes back denied because the payer read the encounter as routine dressing management, an inclusive postoperative service, or an unsupported NPWT charge. That is not just a billing nuisance. It is a margin problem, because the same denial reason usually hits again until someone fixes the process upstream.
Owners should treat wound VAC denials as revenue diagnostics. A denial tells you where money is leaking out of the workflow, whether that leak starts in the note, charge selection, claim edits, or payer policy interpretation. If your team only works denials one claim at a time, they stay busy and the pattern stays expensive.
Read the denial by financial cause
Start with the reason code, then translate it into an operational failure:
- Bundled or inclusive service: The payer believes the NPWT service was part of another service already paid, often because the encounter looked postoperative or the documentation did not support separately billable work.
- Missing or conflicting chart detail: The claim lacks the facts the payer needs to validate the code. For wound VAC, that usually means wound measurements, device classification, treatment setting, or wound status.
- Medical necessity denial: The record did not connect the procedure to a diagnosis and clinical picture that met the payer's coverage rules.
- Frequency or utilization edit: The service pattern triggered a payer edit because repeat billing did not match its interval rules or prior authorization requirements.
That review belongs on a management report, not buried in a biller's work queue. If one denial category keeps repeating, you are looking at a broken rule in your operation.
Ask questions that expose the process gap
A physician-owner does not need to audit every chart. You do need answers to a few operational questions, fast.
- Can your team confirm wound measurements from the signed note before the charge is released?
- Can billing identify the device type from documentation alone, without calling the clinic back?
- Are denials clustering around postoperative encounters where the payer may view the service as inclusive?
- Are same-day procedure combinations reviewed before submission, instead of after the remittance advice arrives?
If those answers are slow, vague, or inconsistent, the problem is not a handful of bad claims. The process has no clear owner. I see this often in surgical and wound care groups. Staff are posting charges and reacting to denials, but nobody is managing the economic logic behind the claim.
Build a denial playbook, not a denial pile
The fix is a short, repeatable playbook. Route each denial type to a defined response. Bundling denials need note review and coding validation. Medical necessity denials need diagnosis and policy review. Missing-information denials usually point to a documentation template problem. Frequency denials require payer-specific billing rules that front-desk, clinical, and billing staff all follow.
That is how practices reduce rework and protect revenue. Clean wound VAC reimbursement comes from preventing predictable denials before the claim leaves your system.
Practice Owner FAQs for Wound VAC Billing
How often can we bill wound VAC CPT codes
A common revenue leak starts here. The practice sees repeated dressing activity and assumes each touchpoint can generate a bill. That is not how these codes work.
For provider-applied NPWT, billing usually follows the treatment encounter, supported by the note, wound details, device type, and the payer's frequency rules. Your team should not treat every supply change or routine dressing action as a separate charge opportunity. That approach creates denials, refund risk, and payer scrutiny.
If your reports show unusually high utilization, do not wait for accounts receivable to age out. Pull a payer-specific frequency review and compare actual billing patterns against your documentation and contract rules.
Should we always use the lower wound VAC code to be safe
Using the lower code "just to be safe" cuts revenue and does not reduce compliance risk. It usually signals that the practice does not trust its own documentation.
Bill the code the record supports. If the wound area meets the higher threshold, or the device falls into a different code family, code it correctly. The fix is not conservative coding. The fix is a note template and charge review process that gives billing enough detail to defend the claim the first time.
I see this mistake often in physician-owned groups. They lose money for months without realizing it, then wonder why wound care volume increased but collections did not.
Can we bill debridement and wound VAC on the same day
Yes, in some cases. The chart has to support separate work, and the payer has to allow separate reimbursement.
Weak habits become expensive. A standing rule to always append a modifier creates avoidable denials. A standing rule to never bill both services leaves money on the table. The right process is chart-based review before claim submission, with someone accountable for checking operative details, timing, wound status, and payer edits.
Ask your billing team for examples. Review one paid same-day claim and one denied same-day claim. In ten minutes, you can usually tell whether your process is disciplined or guesswork.
What is the most important chart detail for preventing wound VAC denials
There is no single detail. Claims hold up best when the note answers three questions clearly: what wound was treated, what size it was, and what device was applied.
For many practices, denials start when one of those facts is missing or buried in free text. If the wound measurements are incomplete, the code level becomes hard to defend. If the device type is vague, billing may choose the wrong code family. If the note does not clearly show treatment of an open wound when separate billing depends on that distinction, the payer has an easy path to deny.
That is not a coding problem alone. It is an operating problem.
If your practice performs wound care, post-surgical treatment, or NPWT regularly, the billing process needs the same discipline as the clinical workflow. Happy Billing helps physician-owned practices tighten documentation-to-claim workflows, reduce preventable denials, and recover revenue lost to coding ambiguity and weak follow-up.