Wound Debridement CPT Code Guide for Practice Revenue
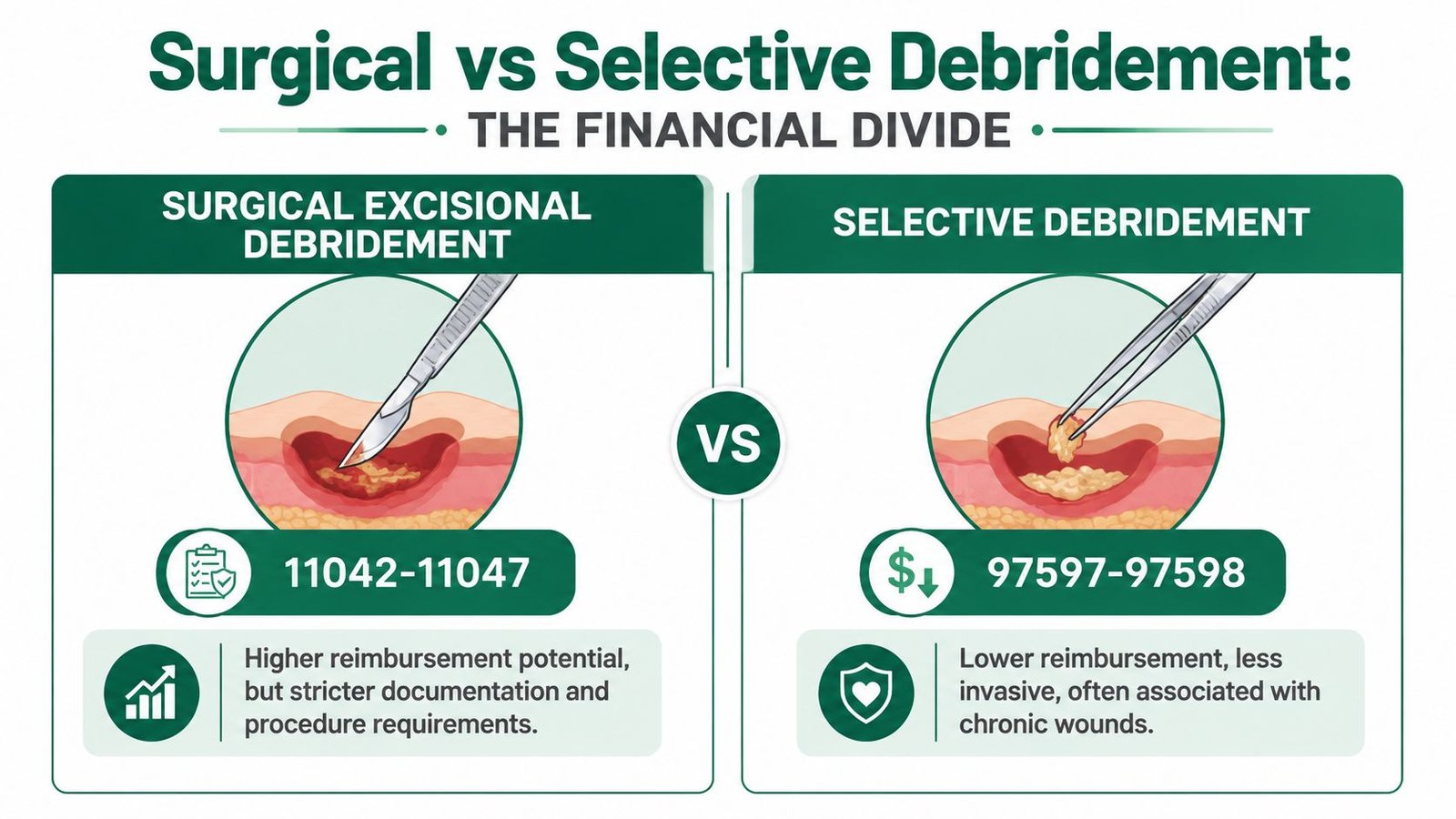
The primary wound debridement CPT codes split into two families. Surgical excisional debridement uses 11042 through 11047 based on tissue depth, and selective debridement uses 97597 through 97598 based on surface area for less deep wounds.
That sounds simple. It isn't. For a practice owner, the core issue is that wound debridement coding sits right at the intersection of reimbursement opportunity, denial exposure, and audit risk. If your note doesn't prove the depth debrided and the surface area debrided, you don't just have a coding problem. You have slower cash flow, more rework, and avoidable accounts receivable drag.
We've seen wound care claims fail for reasons physicians consider minor. A note says the wound "goes to bone," but bone wasn't removed. A provider documents wound size, not the area debrided. A selective debridement claim goes out with no clear proof that devitalized tissue was removed. Those aren't documentation quirks. They're revenue leaks.
Your Financial Risk in Wound Debridement Coding
Wound debridement coding can erode margin. One borderline note can turn a payable claim into a downcode, a denial, or an audit target.
The risk is not limited to obvious errors. It shows up in the gray-zone cases that practices send every day. A clinician documents a chronic ulcer and removes slough, but the note never makes clear whether the work supports 97597, 97598, or a surgical code such as 11042. A wound measures large, but the record fails to separate total wound size from the actual area debrided. A provider documents exposed bone, tendon, or muscle, yet never states that tissue at that depth was removed. Those are the claims payers challenge because they sit right on the line between valid reimbursement and overstatement.
That line matters financially. If your team defaults to the lower-paying selective family when the record supports excisional surgical debridement, you give up legitimate revenue. If the claim goes out with 11042 to 11047 and the note only proves superficial or selective work, you invite a downcode, refund demand, or post-payment review. Either way, your practice pays for the mistake through lost cash, staff rework, and slower collections.
The biggest exposure is operational. Billing staff often receive notes that describe the wound well enough for treatment but not well enough for payment. Payers want the debridement note to stand on its own. They want to see what tissue was removed, the method used, and the amount debrided that supports the billed code set. If any of those elements are vague, your claim enters the system already weakened.
Practical rule: If the note cannot show what tissue was removed, how much was debrided, and whether the work was selective or excisional, the claim is not ready to bill.
Practice owners should treat wound debridement the same way they treat any other high-variance service line. Monitor denial patterns by provider, compare billed codes to documentation quality, and fix the workflow before AR grows. The same discipline used in an RCM framework for physician practices applies here. Clean claims protect revenue. Borderline claims consume it.
Surgical vs Selective Debridement The Financial Divide
Payers don't treat all debridement the same, and your revenue shouldn't either. In wound debridement coding, you're really choosing between active wound care management and surgical debridement. Those are different payment lanes, different documentation burdens, and different audit profiles.
Why payers separate these services
Medicare and CPT guidance have long separated 97597 to 97598 from 11042 to 11047, routing epidermis and dermis only debridement to the selective family and deeper excisional work to the surgical family. Medicare contractors have also published measurement-focused billing guidance for these services since at least 2012, and the repeated 20 sq cm threshold remains central to both code families, as described in this overview of wound care CPT coding history and structure.
That history matters because payers built edits, review habits, and denial logic around it. They expect a selective service to read like selective debridement. They expect a surgical service to read like excisional removal of deeper tissue. If your documentation blurs that line, the payer will make the financial decision for you.
The expensive mistake owners miss
The expensive mistake isn't always overcoding. It's often inconsistency. A provider performs deeper work, but the note sounds superficial. Or the claim goes out as selective because staff rely on the setting or the instrument used instead of the tissue removed.
That mismatch creates three business problems:
- Wrong-code denials: The note doesn't support the code family billed.
- Downcoding risk: The payer pays the lower-level interpretation of the record.
- Audit exposure: Repeated inconsistency across visits makes the practice look undisciplined.
A wound that extends to bone doesn't justify bone debridement unless bone was actually removed. Coding follows the deepest tissue debrided, not the deepest tissue visible.
For owners, the takeaway is simple. Build one internal rule set around this divide and train every provider on it. If your current process can't reliably distinguish selective from surgical debridement, your wound care revenue is unstable. That's exactly why many groups use specialized wound care billing support instead of treating these claims like generic office procedures.
Coding Surgical Debridement 11042-11047 by Depth and Area
Surgical debridement revenue is lost in the borderline cases. The provider did real work, but the note fails to prove the deepest tissue removed, or the area math does not support the add-on code. That is where claims for 11042 to 11047 get cut, downcoded, or pulled into audit review.
These codes are paid by depth debrided and surface area debrided. They are not driven by how severe the wound looks, how deep the ulcer extends, or how dramatic the diagnosis sounds. If bone is exposed but only subcutaneous tissue is removed, billing 11044 invites a takeback.
The code set owners should know
Use this table as an operational rule, not a reference chart your team glances at after the visit:
| CPT Code | Tissue Depth Debrided | Surface Area |
|---|---|---|
| 11042 | Subcutaneous tissue | First 20 sq cm |
| 11045 | Subcutaneous tissue | Each additional 20 sq cm |
| 11043 | Muscle and/or fascia | First 20 sq cm |
| 11046 | Muscle and/or fascia | Each additional 20 sq cm |
| 11044 | Bone | First 20 sq cm |
| 11047 | Bone | Each additional 20 sq cm |
The payment risk is simple. If the note says only "sharp debridement performed," the payer has room to price the service lower than the physician intended, or deny it outright for lack of support.
The deepest-level rule is where practices lose money
For the same anatomic site, report only the deepest tissue level debrided. Do not stack subcutaneous and muscle debridement codes for one wound because both tissue layers were addressed. For wounds at the same depth across different sites, total the debrided surface area. Do not combine area across different depths.
That sounds straightforward until real charts hit the billing queue.
A common failure looks like this: one wound has 12 sq cm of subcutaneous debridement and a smaller 3 sq cm portion debrided down to muscle. The claim goes out with both 11042 and 11043 for the same site. That coding choice creates an easy denial because the record supports the deepest level for that site, not two primary surgical debridement codes layered together.
Another common mistake goes in the opposite direction. A provider debrides multiple subcutaneous wounds on the same date, but the note documents only individual wound sizes and never totals the debrided area by depth. Billing staff stop at 11042 and miss 11045. That is a pure revenue leak.
Borderline documentation decides whether 11042, 11043, or 11044 survives review
Owners should train providers to document the debrided tissue in plain language:
- What tissue was removed: subcutaneous tissue, muscle/fascia, or bone
- How much tissue was debrided: actual debrided area, not just overall wound dimensions
- Which wound received which depth: site-specific detail for each wound
- What made it surgical: excisional removal of devitalized tissue with the method documented
- What remained after debridement: a brief post-procedure status supports medical necessity and depth
The highest-risk charts are the ones with mixed signals. "Wound to bone" plus "debrided slough" does not support 11044 unless bone was removed. "Debrided with curette to healthy bleeding tissue" still fails if the note never names the deepest tissue excised. Payers deny those claims because they can.
A good wound template should force depth, area, and site into separate fields. If your template lets providers free-text the entire procedure in one box, your billing team is left guessing. Guessing produces denials. It also creates inconsistent claim submission on the medical claim form, which is how preventable coding errors turn into write-offs and audit exposure.
Owner's lens: Surgical debridement is not hard to bill. It is hard to bill consistently when providers document wound severity instead of tissue actually removed.
Treat this as a process-control issue. Review denied 11042 to 11047 claims by provider, compare billed depth to documented depth, and fix the template before you argue with the payer. That change protects both reimbursement and audit defensibility.
Coding Selective Debridement 97597-97598 for Active Wound Care
Selective debridement looks low risk because the code set is small. That's misleading. 97597 and 97598 are common denial magnets because practices bill them for services that payers classify as routine wound care, not billable debridement.
CMS guidance is direct. 97597 and 97598 require devitalized tissue, and superficial cleansing or dressing changes alone don't qualify, according to CMS's billing guidance for active wound care procedures. If the note doesn't prove removal of devitalized tissue, the claim is weak on arrival.
What qualifies and what doesn't
For selective debridement of skin only, CPT uses 97597 for the first 20 sq cm or less and 97598 for each additional 20 sq cm, as outlined earlier in the article's coding framework. The payment issue isn't just code selection. It's whether the record supports that the provider performed a covered service instead of cleaning the wound.
What usually supports a selective debridement claim:
- Documented devitalized tissue: Slough, fibrin, eschar, or similar nonviable tissue.
- A defined method: The note should say how the tissue was removed.
- Measured surface area: Without that, the code count is exposed.
What usually undermines the claim:
- Routine care language: "Wound cleaned" or "dressing changed."
- No tissue description: The payer can't tell what was removed.
- No distinction from surgical debridement: Confusion between code families leads to edits and denials.
Why these claims get denied so often
Selective debridement is where many practices let templates do too much work. The EHR may autopopulate a wound visit note, but a payer wants proof that the provider removed devitalized tissue and did more than maintenance care. If that proof isn't visible, the claim may be denied even when the treatment was clinically appropriate.
This is also where outpatient groups often miss the operational detail that these services can be performed by physicians, non-physician practitioners, or therapists acting within scope under current Medicare policy materials, as noted in the earlier discussion of the code family's operational use. If your practice involves multiple provider types, your documentation rules must be standardized across them.
Selective debridement is billable care. Routine cleansing is not. If your notes read the same for both, the payer will assume the lower-value interpretation.
Owners should audit these encounters for one thing above all else: whether the note would still support payment if someone unfamiliar with the patient read it cold. If the answer is no, you don't have a coding process. You have a hope-based process. The same discipline physicians already use with timed therapy services and rules like the 8-minute rule in billing should be applied here. Documentation must prove why the code belongs on the claim.
Critical Documentation That Prevents Debridement Denials
Weak debridement documentation costs money fast. It triggers downcoding, stalls cash, and hands auditors an easy target.
For wound debridement, the note has to prove exactly what tissue was removed, how deep the provider went, and how much tissue was debrided. Payers do not reimburse from assumptions. They reimburse from what the chart states. If your provider documents a 6 cm x 6 cm wound but fails to identify the debrided portion and post-debridement depth, your team may bill 11042 or 97597 confidently and still lose the claim on review.
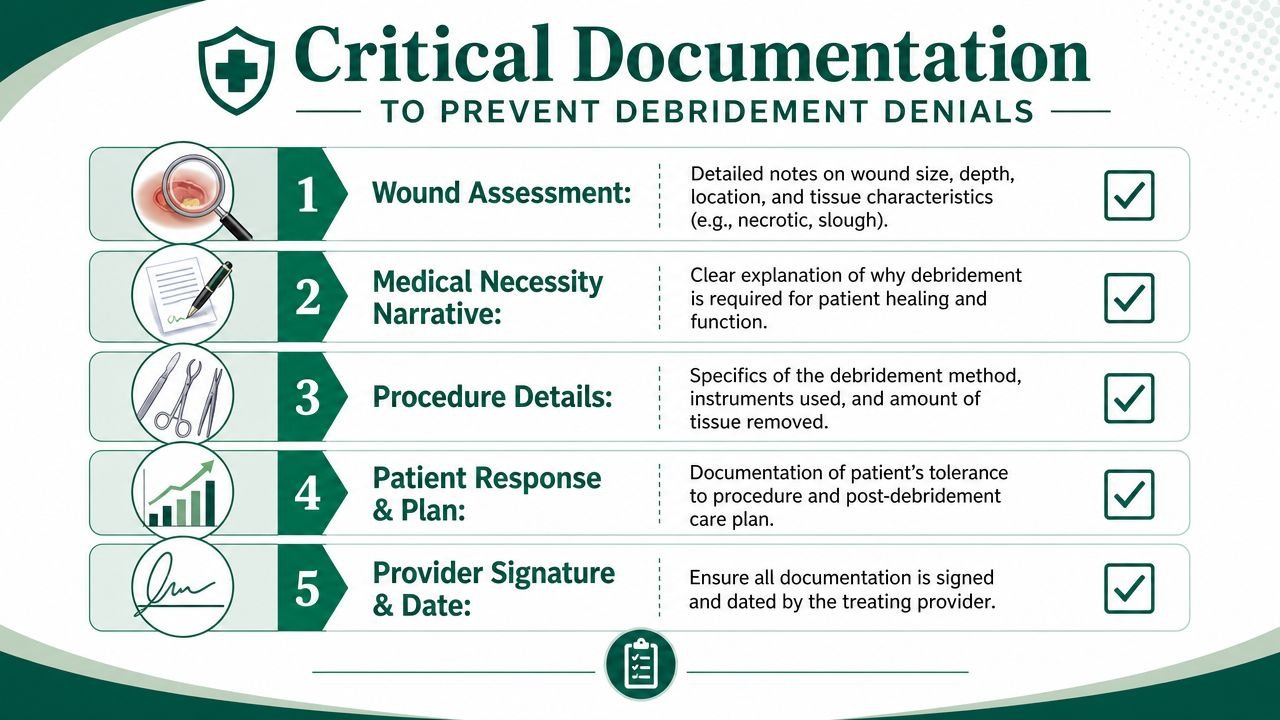
What the chart must prove
A paid claim usually comes down to whether the note answers the payer's real questions without forcing the biller to guess.
- Exact wound location. Document laterality and anatomical site. "Lower extremity ulcer" is weak. "Right lateral ankle ulcer" supports cleaner claim lines and cleaner appeals.
- Tissue removed. Name it. Slough, fibrin, necrotic subcutaneous tissue, nonviable muscle. "Debrided wound bed" is too vague and often gets read as routine wound care.
- Depth reached after debridement. This is the audit line between selective and surgical coding. If the note does not clearly support skin, subcutaneous tissue, muscle/fascia, or bone, expect a denial or downcode.
- Surface area debrided. Document the area treated, not just total wound size. That difference affects whether the claim supports only the base code or also an add-on code such as 11045, 11046, 11047, or 97598.
- Method and instruments used. Curette, scalpel, scissors, forceps. Payers look for evidence of a real procedure, not dressing change language copied from a nursing note.
- Clinical reason for debridement. Document devitalized tissue, delayed healing, infection risk, or other case-specific rationale. Without medical necessity, even a technically complete note can fail.
- Post-debridement wound description. Include the remaining wound measurements and wound bed condition after the procedure.
Borderline cases create the biggest revenue leaks. A provider may remove slough with a curette and document "to bleeding tissue" without stating whether subcutaneous tissue was debrided. That wording invites a payer to recast the service as 97597 instead of 11042. The payment gap is not academic. It directly affects margin, especially in high-volume wound programs.
The documentation standard your team should enforce
Do not let providers chart debridement in free text alone. Build a procedure template with required fields for tissue type, debrided area, depth after debridement, instrument used, and post-procedure assessment. If any field is blank, the chart should not be ready for claim submission.
That is a business rule, not a preference.
If your clinicians still start with handwritten wound logs, paper flow sheets, or bedside notes that get keyed in later, fix the intake process. A fragmented record creates omissions that payers use against you. A document workflow modeled on Smart Receipts business digitization helps practices convert scattered paper inputs into searchable records before those gaps turn into denials.
Owners should also audit these notes the same way they audit front-end claim accuracy. A debridement encounter is not ready just because the CPT code matches the visit superbill. It is ready when the documentation can support the code under payer review and pass your clean claim documentation standard.
One weak sentence can erase the value of the whole procedure.
Navigating Modifiers and Bundling Rules for Maximum Reimbursement
Payers use bundling edits to cut payment automatically. If your claims team doesn't know when a service is distinct, the software decides for them, and the software isn't trying to protect your margin.
The biggest problem areas in wound debridement are same-day debridement across different wounds, different depths, and encounters that include both debridement and an E/M service. In these cases, modifier 59 and modifier 25 are most critical.
When modifier 59 protects payment
The practical issue is separation. If distinct wounds at different sites or depths are treated in the same encounter, your claim may need modifier 59 to show the procedures are separate and not bundled together. Coding guidance aimed at wound care notes that modifiers are frequently discussed but often not explained in a way that helps practices avoid denials in multi-wound, multi-depth scenarios.
For owners, the key isn't memorizing every edit. It's requiring the chart to make distinction obvious. If the documentation doesn't identify separate sites, separate tissue depths, and separate measurements, your biller has nothing solid to defend.
A useful internal rule:
- Distinct site documented clearly: Consider whether modifier 59 is appropriate.
- Different-depth wounds documented separately: Support the claim line by line.
- One vague procedure note covering everything: Expect bundling trouble.
When modifier 25 earns its place
Modifier 25 belongs only when a significant, separately identifiable E/M service occurs on the same day as the debridement. This is another area where owners lose revenue from both sides. Some practices never bill the E/M because they're afraid of scrutiny. Others append modifier 25 automatically and invite denials.
The financial standard should be stricter than the coding habit. Ask one question: did the provider do meaningful evaluation work beyond the procedure itself, and is that work visible in the record?
If your same-day E/M note reads like prelude to the procedure, don't expect the payer to pay it separately.
Bundling edits aren't random. They are payer systems doing what they were designed to do. Your defense is precise documentation plus disciplined modifier use. When that system breaks repeatedly, A/R lengthens because your team keeps resubmitting claims that should have been right the first time.
Common Denial Reasons and How to Appeal Them
Many practices treat debridement denials as routine friction. That's a mistake. Most of them are predictable, and predictable denials are fixable.
Coding guidance focused on wound care points out a major gap in the market: borderline cases. Practices struggle with choosing between selective and surgical codes when the encounter includes different depths, different body sites, or debridement plus an E/M service. It also notes that denials often turn on exact record detail such as site, depth, tissue type, method, and whether cutting extended beyond the wound margin, as discussed in this analysis of wound care debridement coding problems.

The denial patterns that matter most
Most wound debridement denials fall into a few buckets:
- Insufficient documentation: The note doesn't prove depth, area, or devitalized tissue removal.
- Wrong code family: The payer reads the service as selective when you billed surgical, or the reverse.
- Bundling issues: Distinct wounds or same-day services weren't documented well enough to support separate payment.
- Medical necessity concerns: The note doesn't explain why debridement was needed at that visit.
The borderline cases create the most rework. A small amount of sharp removal doesn't automatically make the service surgical. But if the provider removed deeper tissue and documented it poorly, you still lose.
How to build an appeal that can win
An appeal should never sound emotional. It should read like a crosswalk between the denied claim and the chart.
Use this structure:
- State the code billed and the payer's denial reason.
- Point to the exact documentation that supports site, tissue depth, area, and method.
- Clarify whether the wound involved distinct sites or separate same-day E/M work.
- Request reconsideration based on the record, not a generic argument.
Sample appeal language a practice owner can require staff to use:
The medical record supports the billed debridement service because it identifies the wound site, the tissue removed, the depth of removal, the method used, and the measured area actually debrided. The procedure note documents the service performed rather than routine wound cleansing, and the claim should be reprocessed based on the documented procedure details.
If your team keeps fighting the same denial reason, stop treating each claim as an isolated event. That's a system failure. Review templates, provider habits, and charge review rules. And if debridement denials keep draining staff time, get an outside review through a free RCM audit for your practice before the problem hardens into permanent write-offs.
FAQs Wound Debridement Billing for Practice Owners
How do I know if my practice is undercoding wound debridement
Start by comparing procedure notes against billed CPT families. If providers document removal of deeper tissue but your claims consistently land in the selective family, you likely have undercoding. Owners should review whether the chart identifies the deepest tissue removed and the surface area debrided. If those fields are missing or buried in free text, your team will default to safer codes and lower collections.
Why do payers keep denying 97597 and 97598
Because these claims often read like routine wound care instead of billable selective debridement. CMS guidance requires devitalized tissue for 97597 and 97598, and superficial cleansing or dressing changes alone don't qualify. If the note doesn't clearly show removal of devitalized tissue and measured area, the payer has an easy denial path.
Can we bill debridement and an E M visit on the same day
Sometimes. The deciding factor is whether the E/M was significant and separately identifiable from the procedure itself. If your physician evaluated a broader problem, changed management, or addressed issues beyond the work normally tied to the debridement, the E/M may be defensible with modifier 25. If the note only supports the procedure, billing both just increases denial risk.
What should I audit first if wound care A R is rising
Audit documentation before you audit payment posting. Look at a sample of denied and paid claims and ask four questions: was the site clear, was the tissue removed named, was the depth explicit, and was the area debrided recorded? In our experience, those four fields expose most of the revenue leakage. If you want a benchmark for specialty-specific support, review the billing workflows used in areas such as orthopedic revenue cycle management, where procedure documentation and payer edits already demand tighter controls.
If wound debridement claims are slowing cash flow, increasing denials, or forcing your staff into repeated appeals, it's time to inspect the process instead of blaming the payer. Happy Billing helps independent practices tighten documentation-to-claim workflows, reduce revenue leakage, and correct the denial patterns that keep wound care A/R hanging open.