8 Minute Rule Billing: A Guide to CPT Code Units
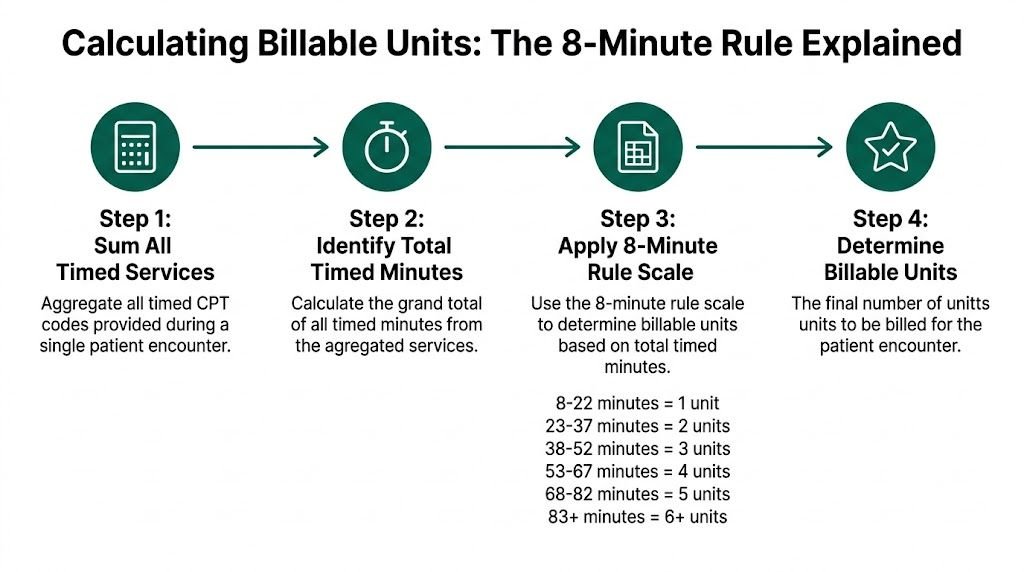
TL;DR: The 8 minute rule billing standard requires you to total all timed treatment minutes in one session, then bill by CMS thresholds, not by judging each CPT code on its own. Under Medicare, 8 to 22 minutes = 1 unit, 23 to 37 minutes = 2 units, 38 to 52 minutes = 3 units, 53 to 67 minutes = 4 units, 68 to 82 minutes = 5 units, 83 to 97 minutes = 6 units, 98 to 112 minutes = 7 units, and 113 to 127 minutes = 8 units.
Time reporting errors aren't a minor cleanup issue. 40 to 60% of PT claims are denied due to time-reporting errors, and underbilling affects 25% of practices, costing $5K to $10K annually per provider according to this 8-minute rule billing analysis.
If you're managing PT, OT, SLP, ortho rehab, pain, or any multi-payer therapy workflow, the expensive mistakes usually aren't in the definition. They happen in two places: when staff apply the wrong payer logic, and when mixed timed and untimed sessions aren't documented tightly enough to support the units billed.
Mastering the 8-Minute Rule for Maximum Reimbursement
One unit can be lost or overbilled on a single visit when the therapist documents “45 minutes” but the claim needs billable, code-level timed minutes. That gap is where revenue leakage and denials start, especially in clinics seeing a mix of Medicare, Medicare Advantage, and commercial plans on the same schedule.
Under Medicare’s 8-minute rule, timed units come from the total direct, one-on-one minutes across all timed CPT codes in the session, then converted into units using the CMS thresholds. The work is not hard. The operational reality is. You have to choose the right payer logic and reconcile sessions that include both timed and untimed services.
The two places practices bleed money
1) Payer rule mismatches (CMS vs. commercial “Rule of 8s”).
Teams often assume every payer follows CMS aggregation. Some commercial plans use a “Rule of 8s” approach that can change how units are counted across codes. If the front office verifies benefits but does not confirm the time rule, the billing team ends up fixing it after the fact through appeals or write-offs. Set a payer matrix in your billing SOPs that states, by payer and product, whether to aggregate timed minutes across codes (CMS style) or apply a different unit method.
2) Mixed timed and untimed sessions (the most common documentation failure).
A lot of real visits are not “all timed” therapy. They look like eval plus treatment, or timed ther-ex plus an untimed modality, with time split across multiple CPTs. Medicare timed examples include 97110, 97112, 97140, 97530, and 97535. Untimed services such as 97161-97163 (PT eval levels), 97165-97167 (OT eval levels), and common untimed modalities do not go into the timed-minute pool. If staff roll everything into one total, the claim can end up with the wrong unit count and the wrong risk profile.
What actually counts (and what does not)
Count only direct, skilled, one-on-one minutes tied to timed CPT codes. Do not count setup, rest breaks that are not skilled intervention, documentation time after treatment, or general supervision time. The cleanest operational standard is simple: the note should support (1) the total timed minutes, and (2) how those minutes were distributed across the billed timed codes.
Practical rule: If the note does not support timed minutes by billed code, expect denials on time-based edits and assume poor audit defensibility.
Build a process that survives real-world scheduling
The clinics that get paid cleanly treat time-based billing like a production workflow, not a memory test. Standardize three handoffs: the therapist captures timed minutes by code, the charge poster converts total timed minutes into units under the correct payer logic, and someone runs a same-day edit check for mixed timed and untimed visits before claims drop. That structure reduces corrected claims, keeps A/R aging from ballooning, and lowers the odds of recoupments tied to time documentation.
If you want a practical framework for tightening the handoff between clinical documentation, charge entry, and collections, use this overview of RCM operations for physician practices as a starting point.
Where the risk shows up most
| Specialty area | Common exposure |
|---|---|
| Physical therapy | High volume of 97110, 97112, 97140, 97530 |
| Occupational therapy | Frequent mixing of timed treatment and untimed evaluations |
| Speech-language pathology | Timed treatment workflows that need precise minute capture |
| Orthopedics and pain | Therapy-heavy ancillary services with mixed payer rules |
Calculating Billable Units from Total Timed Minutes
Small time-entry mistakes create outsized write-offs. In therapy billing, one wrong unit on high-volume codes like 97110, 97112, 97140, or 97530 can turn into recurring revenue leakage across hundreds of visits.
Under CMS methodology, the order matters. Total the timed treatment minutes for the session first. Convert that total into billable units second. Then assign those units to the timed CPT codes that account for the treatment time.
The CMS unit conversion chart
Use the session total, not separate 15-minute blocks by code.
| Number of Units | Total Timed Minutes |
|---|---|
| 1 unit | 8-22 minutes |
| 2 units | 23-37 minutes |
| 3 units | 38-52 minutes |
| 4 units | 53-67 minutes |
| 5 units | 68-82 minutes |
| 6 units | 83-97 minutes |
| 7 units | 98-112 minutes |
| 8 units | 113-127 minutes |
The calculation sequence that prevents underbilling and overbilling
Use the same five-step process on every timed visit:
- Identify only timed CPT codes in the encounter, such as 97110, 97112, 97140, and 97530.
- Remove non-billable minutes such as setup, rest breaks, note completion, and therapist time that is not direct one-on-one treatment.
- Add all billable timed minutes across the session.
- Match the total minutes to the CMS range for unit count.
- Distribute the units to the timed codes with the largest documented time if more than one code was performed.
A straightforward example:
- 97110 therapeutic exercise = 20 minutes
- 97140 manual therapy = 15 minutes
That visit has 35 total timed minutes. Under CMS, 35 minutes = 2 units.
Where staff usually miscalculate
The common error is treating each code like it must independently reach 15 minutes. CMS does not work that way. CMS looks at the session total first, then at how the minutes support the unit assignment.
For example, if a therapist documents:
- 97110 = 8 minutes
- 97140 = 8 minutes
The total timed treatment is 16 minutes, which supports 1 unit, not 2. Staff often overcode this visit because both services crossed 8 minutes. Under CMS aggregation, the session still supports only one timed unit. Unit assignment then has to match the code that best fits the documented minutes and payer logic.
That distinction matters even more in mixed-service visits, especially when untimed codes are also on the claim.
Mixed timed and untimed visits are where revenue leakage happens
A common therapy encounter includes one untimed service and several timed services. For example:
- 97010 hot/cold packs, untimed
- 97110 = 18 minutes
- 97530 = 12 minutes
Only the timed codes count toward the 8-minute calculation. The untimed code is billed separately if payer policy allows it, but its presence does not increase the timed unit count. In this example, the timed total is 30 minutes, which supports 2 units, plus the untimed service if covered and documented.
I see two failure points here in real operations. Some teams accidentally add untimed service minutes into the total and overbill. Others underbill because the biller hesitates to assign two timed units when the minutes are split across two codes. Both errors hurt margin. One creates refunds and audit risk. The other drains revenue insidiously.
Practical examples your charge team should know cold
| Timed services performed | Total timed minutes | Billable result |
|---|---|---|
| 97110 for 15 minutes | 15 | 1 unit |
| 97110 for 20 minutes + 97112 for 10 minutes | 30 | 2 units |
| 97110 for 24 minutes + 97140 for 14 minutes | 38 | 3 units |
| 97110 for 7 minutes 59 seconds | Under threshold | 0 units |
The last example is not trivial. If the documentation shows less than 8 minutes, the service does not support a timed unit under CMS.
Operational controls that keep claims clean
Do not ask billing staff to reconstruct minutes from a narrative note retrospectively. Require therapists to capture time by CPT code during the visit, or immediately after, while the session details are still accurate. Then run a front-end edit for three things: missing timed minutes, timed totals that do not match billed units, and claims where untimed services appear to have been folded into the timed total.
That edit logic improves first-pass resolution and reduces corrected claims. It also supports a stronger clean claim workflow in medical billing when your team is auditing therapy charges before submission.
Navigating Payer Variations The 8-Minute Rule vs The Rule of 8s
The costliest mistake in 8 minute rule billing is assuming every payer follows CMS logic. They don't.

Some commercial plans use Substantial Portion Methodology, often called the Rule of 8s. Under that approach, each timed CPT code is evaluated on its own rather than aggregated across the whole session.
Side-by-side logic
| Issue | CMS 8-minute rule | Rule of 8s / SPM |
|---|---|---|
| Primary calculation method | Aggregate all timed minutes in the session | Evaluate each timed code separately |
| 8-minute threshold | Applied to total session time | Applied per code |
| Best fit | Medicare and CMS-based payer logic | Some commercial payer contracts |
| Common risk | Underbilling or wrong unit assignment | Overlooking code-level thresholds |
The practical difference is huge.
- Scenario A
- 97110 = 7 minutes
- 97112 = 7 minutes
Under CMS, the total is 14 minutes, so you can bill 1 unit. Under a strict Rule of 8s, neither code reached 8 minutes, so you bill 0 units.
- Scenario B
- three timed services in a 45-minute session
According to this comparison of CMS and SPM methods, SPM can increase billable units by 10 to 20% for non-Medicare payers. The same source notes that a 45-minute session can produce different results depending on the payer methodology.
What works in real operations
A practice manager shouldn't leave this to therapist memory. Build a payer matrix and make it visible at scheduling, charge review, and claim scrub stages.
Use a simple internal policy:
- Medicare and Medicare-based plans: apply CMS aggregation logic.
- Commercial plans: verify whether the contract or provider manual uses CMS aggregation or per-code logic.
- If the payer language is unclear: confirm before claims go out. Don't let staff guess.
The same treatment note can be compliant under one payer and wrong under another. That's why payer setup is a billing control, not an education issue alone.
Where this hits multi-specialty groups
Orthopedic groups, pain clinics, and rehab-heavy physician practices feel this problem more than standalone therapy offices because therapy may be only one piece of the revenue cycle. That makes payer-rule drift easier to miss.
Mental health groups run into the same broader issue with time-based coding logic, even though the codes differ. If your team also handles psychotherapy time ranges, this explainer on mental health billing CPT 90837 vs 90834 is a good contrast in how payer time rules can vary by service family.
The trade-off
SPM can increase units in some commercial workflows. It can also create compliance exposure if staff apply it to a Medicare claim. CMS aggregation is simpler to standardize, but it may leave money on the table if a non-Medicare payer allows per-code billing.
That trade-off is why payer-specific governance matters more than memorizing one formula.
Bulletproof Documentation Your Best Defense in an Audit
Every 8 minute rule billing problem eventually becomes a documentation problem. Payers don't audit your intentions. They audit the note.

Mixed-service sessions are where revenue leaks hide. Existing guidance often leaves practices without a clear method for handling timed treatment alongside untimed services, and that ambiguity leads providers to underbill or overcorrect out of audit fear, especially in assessment-heavy workflows, as noted in this discussion of mixed-service session leakage.
What every timed note should include
A defensible note should show:
- Specific timed CPT codes such as 97110, 97112, 97140, 97530, or 97535
- Start and stop times for each timed service
- Total timed minutes for the session
- Clear separation between timed services and untimed services like 97161, 97164, 97165, or 97010
- Skilled intervention detail, not just “patient tolerated treatment well”
- Medical necessity and patient response
A note that says only “45 minutes of therapy performed” forces your billing team to infer the unit logic. That's exactly what you don't want during an audit.
Mixed timed and untimed sessions
Here, many clinics get conservative and lose earned revenue.
Example:
- 97161 PT evaluation
- 97110 therapeutic exercise
- 97140 manual therapy
- 97010 hot/cold pack
The evaluation and hot/cold pack are not part of the timed-unit calculation. Only the direct timed treatment belongs in the 8-minute math. But your note still needs to distinguish all four services clearly so the claim tells a coherent story.
A mixed session can be fully compliant and still get denied if the note blends untimed and timed work into one undifferentiated block of treatment time.
EHR controls that actually help
Don't rely on “remembering to document better.” Hardwire the process.
Build required fields
Configure the note template so therapists must enter:
- CPT code
- start time
- stop time
- minutes
- discipline
- assistant involvement when applicable
If any field is blank, the charge shouldn't move to final billing.
Separate services visibly
Timed and untimed services should live in different sections of the template. That prevents a common back-end error where staff accidentally count untimed activity toward unit thresholds.
Flag modifier logic
If the same encounter may also involve modifier decisions, your billers need that visible before submission. For practices that regularly work through modifier edits and encounter-level claim issues, this guide on CPT modifiers 25 is a useful reminder that documentation and modifier support have to align before the claim is released.
Avoiding Common Pitfalls and Costly Denials
A small unit-calculation error on high-volume therapy codes like 97110, 97112, 97140, and 97530 can turn into a steady write-off problem by month end. The denial usually starts upstream, in charge capture, note structure, or payer-rule mismatch.

The expensive mistakes are predictable. Staff count minutes that are not billable, apply CMS aggregation to a payer that uses a stricter Rule of 8s approach, or combine untimed and timed services in a way the documentation cannot support. Each one slows payment, raises rework, and pushes avoidable denials into A/R.
Pitfall one: counting non-direct time
Setup, cleanup, fetching supplies, and documentation after the patient leaves do not belong in timed treatment minutes.
Correct approach: count only direct one-on-one treatment time attached to a timed CPT code such as 97110, 97112, 97140, or 97530. If the note says 23 minutes of direct therapeutic exercise and 12 minutes of non-billable activity, the billable total is 23, not 35.
Pitfall two: forcing units that the minutes do not support
A claim with 7 minutes of 97140 billed as 1 unit will not hold up under review. The same problem shows up when staff round 22 minutes of 97110 to 2 units without checking the rest of the timed services in the session.
Correct approach: apply the payer's actual unit methodology every time. Under CMS-style aggregation, total timed minutes across eligible codes determine the number of units, then those units are assigned to the services performed. Under a commercial Rule of 8s policy, each individual code may need to clear its own 8-minute threshold. That difference drives denials more often than practices expect.
Pitfall three: blending timed and untimed services
A session that includes 97161 and 97110 needs two different billing logics. The evaluation is service-based. The exercise code is time-based.
Correct approach: bill the evaluation separately and calculate units only from the timed treatment minutes. If a therapist performs an untimed eval, 15 minutes of 97110, and 10 minutes of 97140, only the 25 timed minutes belong in the unit calculation. Mixing all activity into one total creates revenue leakage in both directions. You either overbill and invite denials, or underbill and give away earned revenue.
Pitfall four: assistant modifier errors
Assistant involvement is where documentation weakness becomes a payment problem fast. Guidance for the 2026 rule changes is expected to emphasize accurate use of CQ and CO modifiers, along with clear support for who furnished each portion of care and for how long.
That matters for:
- CQ when a PTA is involved
- CO when an OTA is involved
If the note does not separate therapist time from assistant time, billers end up guessing which units need modifier treatment and whether the payment reduction applies. That is how clean claims turn into corrected claims, takebacks, and avoidable staff rework.
Assistant modifier compliance is not a billing-office fix. It starts with minute-level treatment documentation.
Pitfall five: no payer-rule audit
The same clinician can treat a Medicare patient at 9:00 and a commercial patient at 11:00 with similar services, then require two different unit calculations. Practices that do not audit by payer usually find the problem only after denials hit.
Correct approach: review claims by payer and by code family, not just by provider. Pull samples for 97110, 97112, 97140, 97530, and 97535 across mixed contracts. Check whether the billed units match the plan's methodology, especially on days with multiple timed codes and mixed timed or untimed visits. For practices tightening this process, a clear framework for outsourced revenue cycle management can help standardize edits and reduce preventable rework before claims go out.
When to Partner with an RCM Expert for Billing Velocity
Some practices can manage 8 minute rule billing internally. Some can't, at least not without constant rework.
The tipping point isn't frustration. It's operational drag. If your team spends too much time rechecking 97110, 97112, 97140, 97530, and 97535 units across mixed payer contracts, the hidden cost isn't just denials. It's slower cash movement, slower charge finalization, and slower follow-up.
Signs your internal process has outgrown itself
- Payer-rule confusion keeps surfacing in charge review.
- Therapist notes arrive incomplete, and billers have to reconstruct minutes.
- Assistant modifier handling isn't consistent.
- Mixed timed and untimed sessions trigger repeated edits.
- Supervisors spend too much time teaching the same rules instead of managing throughput.
An experienced RCM partner becomes valuable when the practice needs discipline, not just labor. The right partner standardizes payer matrices, catches unit-calculation errors before submission, and keeps documentation defects from reaching the claim stage.
For groups evaluating whether that handoff makes financial sense, this resource on outsourced revenue cycle management lays out the business case clearly.
The primary goal isn't outsourcing for its own sake. It's maintaining billing velocity while protecting compliance when payer logic and therapy documentation get too complex for a stretched in-house team.
Frequently Asked Questions
How do I bill if a timed service is interrupted
Pause the timer when direct treatment stops. Only direct, one-on-one treatment time should count toward timed unit calculation. If the service changes after the interruption, document the new service separately instead of blending everything into one block.
Can I use the 8-minute rule for group therapy CPT 97150
No. 97150 is service-based, not a timed code for 8-minute unit conversion. Bill the service according to the code rules and document the session appropriately, but don't run 97150 through the timed-minute threshold chart.
What happens if two therapists treat in the same session
Treat co-treatment carefully. Each discipline must document its own distinct medically necessary work, and the total billed time can't exceed the actual session structure supported by the note. If a PT and OT both work the case, their documentation needs to show separate services and separate rationale.
Does the 8-minute rule apply to telehealth therapy services
If the payer allows the timed therapy service through telehealth, the time logic still depends on direct treatment time. Document start and stop times for the synchronous session and apply the payer's rule set consistently. If telehealth also requires a modifier such as 95, that modifier doesn't change the underlying timed-unit calculation.
If your practice is losing time to unit disputes, payer-rule confusion, or preventable therapy denials, Happy Billing can help tighten the process without forcing an EHR migration. Their team combines specialty-aware RCM workflows with human audit review to reduce leakage, accelerate claim turnaround, and keep complex billing rules from turning into avoidable A/R.