Master an Example of CMS 1500 Form Completed (2026)

A strong example of cms 1500 form completed does more than show where data goes. It shows how the right diagnosis pointer, modifier, NPI placement, authorization detail, and assignment choice protect payment. In one anesthesiology case study, standardizing CMS-1500 completion with AI-assisted modifier validation pushed first-pass clean claim acceptance to 98% and cut initial denials from 22% to 4% compared with prior manual submissions (CourseHero anesthesiology CMS-1500 case study).
Stop denials by treating the form as a specialty-specific billing tool, not a generic claims worksheet. The examples below give you five practical templates for high-value specialties, with concrete CPT and modifier guidance you can turn into front-end and billing team SOPs.
1. Example 1 Anesthesiology Medically Directed Case Modifier QK
Anesthesia claims break fast when the CMS-1500 and the anesthesia record describe different staffing. In a medically directed case, the form has to show the physician's role with the same precision documented in the note, the time record, and the concurrency log. That is why this example matters. Generic government samples rarely show how modifier selection, units, and rendering NPI placement affect payment in a real anesthesia workflow.
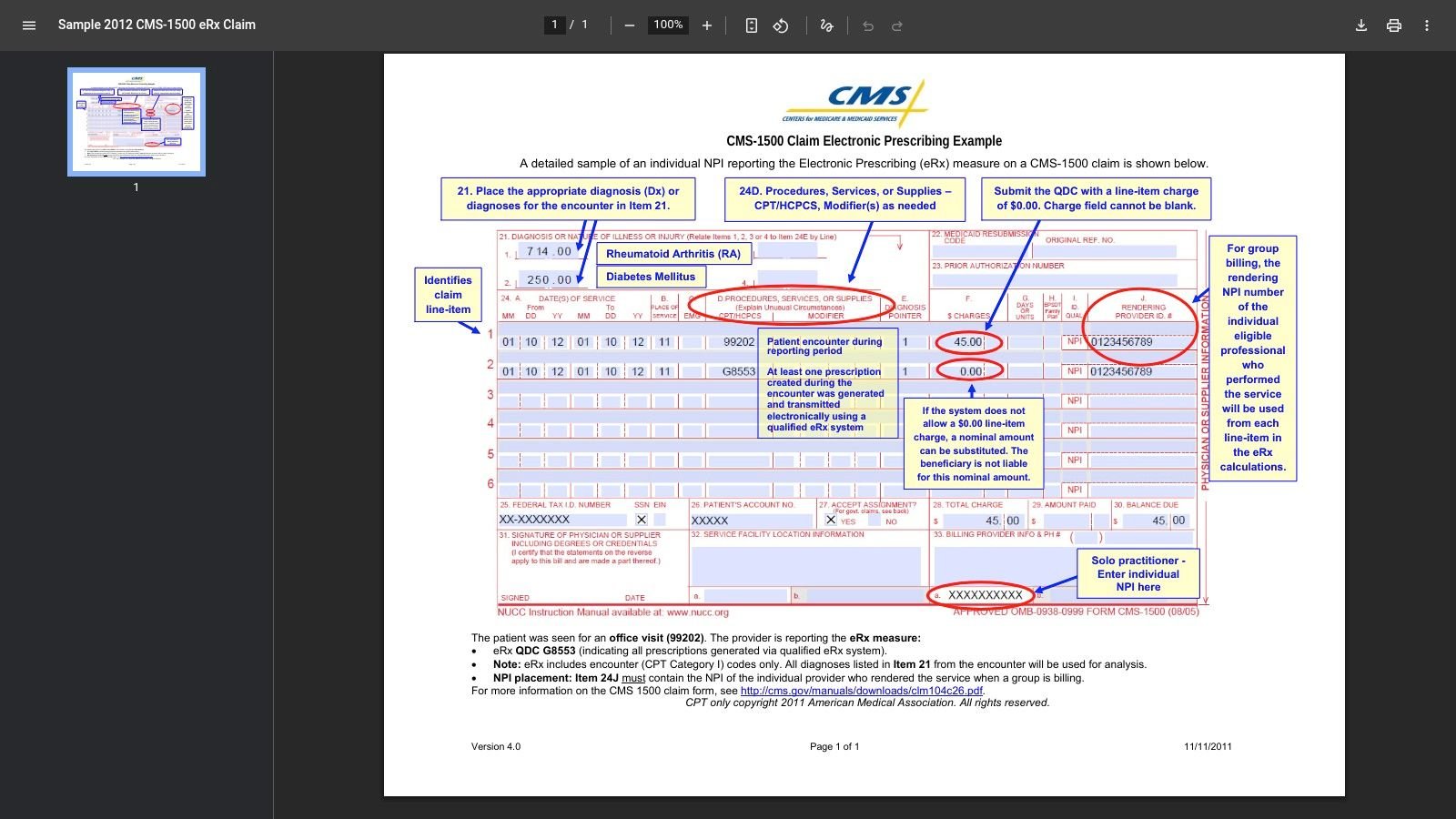
For a QK scenario, focus on the fields that drive denials first: Item 24D for the anesthesia CPT and modifier, Item 24G for units, Item 24J for the rendering NPI, and Item 21 for diagnosis support. If any one of those fields conflicts with the operative record, the payer has a reason to reject, pend, or downcode the claim.
How to populate the critical boxes
Use this structure for the anesthesiologist's line item on a medically directed case:
- Item 21 diagnoses: List the ICD-10 codes that support the surgical encounter and anesthesia service in the correct order.
- Item 24A dates of service: Enter the exact date the anesthesia service occurred.
- Item 24B POS: Use the place of service that matches the operative setting and payer billing rules.
- Item 24D CPT and modifier: Report the anesthesia CPT code from the 00100 to 01999 range, then append QK only when documentation supports medical direction.
- Item 24E diagnosis pointer: Point to the diagnosis letter that supports medical necessity for that anesthesia line.
- Item 24G units: Enter units that match your documented base-plus-time calculation.
- Item 24J rendering NPI: Use the anesthesiologist's NPI on the physician line.
Ensure the CMS-1500 always aligns with the staffing story in the anesthesia record. If the note supports personal performance, bill AA. If the note supports medical direction, bill the medical direction modifier set and make the companion provider line match it.
The common failure point is not the anesthesia CPT itself. It is the modifier logic around who performed the service, who directed it, and whether the unit calculation can survive audit.
What owners should audit every week
Practice owners should review three edits before any anesthesia batch goes out:
- Modifier pairing: QK, QX, QY, QS, and AA must match the documented participation model on every related line.
- Diagnosis linkage: The diagnosis pointer in Item 24E must support the anesthesia code billed in Item 24D, with the correct rendering NPI in 24J.
- Unit integrity: Time units, base units, and any special anesthesia billing rules must reconcile to the anesthesia record before submission.
One more operational point matters. Claims with multiple anesthesia-related service lines can outgrow paper-form logic quickly. If the case structure exceeds what the CMS-1500 can cleanly support, submit electronically through 837P instead of forcing a manual workaround that creates avoidable edits.
If your billers need a tighter reference than a generic form sample, keep a specialty-specific cheat sheet tied to anesthesia CPT code guidance and your top payer rules. For specialty support beyond templates, practices can also review Happy Billing’s anesthesiology billing services.
2. Example 2 Mental Health Telehealth Therapy Session Modifier 95
Teletherapy claims get denied for small setup errors that should never leave the front desk. In mental health, a strong example of cms 1500 form completed has to do more than show a psychotherapy CPT. It needs to show the exact telehealth signal, the right diagnosis linkage, and the authorization data that keeps the claim from stopping in payer edits.
Use a common case: a psychotherapy session billed with 90837 and modifier 95 for a synchronous video visit, with place of service set to the payer’s telehealth rule. That last detail matters. Some payers want POS 10 or 02, and getting that wrong can trigger an avoidable denial even when the note supports the service.
The boxes that drive payment
For mental health telehealth, owners should pay closest attention to Boxes 11, 21, 23, and Item 24.
- Box 11 and 11d: Make subscriber, plan, and coverage data match the active policy on the date of service.
- Box 21: List the diagnosis codes that support medical necessity for the therapy service.
- Box 23: Enter the prior authorization number when the payer requires one.
- Item 24B: Use the correct place of service for the payer’s telehealth policy.
- Item 24D: Report the psychotherapy CPT and append modifier 95 when required.
- Item 24E: Point the service line to the correct diagnosis code in Box 21.
Mental health billing breaks down when staff treat telehealth as a simple modifier add-on. It is a payer-rule workflow. Eligibility, authorization, POS selection, and diagnosis pointer logic all have to match on the same claim.
If Box 23 is blank on an auth-required therapy claim, expect a denial even if the documentation is flawless.
How to build this claim correctly
Train billers to check the claim in this order:
- Eligibility first: Confirm subscriber and plan data before the visit.
- Auth next: Record the authorization number and approved date span in scheduling, then carry it into Box 23.
- Telehealth configuration: Use the payer-required POS and add modifier 95 when the plan requires it for synchronous video.
- Diagnosis linkage: Put the supported diagnosis codes in Box 21 and match the service line pointer in 24E.
- Provider identity: Validate the rendering NPI and billing provider information before release. Specialty-specific examples are important here. Generic government samples do not show the claim decisions that drive denials in behavioral health teletherapy. A practice that bills high-volume therapy visits needs annotated, code-level rules for telehealth, not a blank template and guesswork. Teams working recurring video-visit denials should standardize payer rules with a focused telehealth billing guide for mental health providers.
3. Example 3 Orthopedics Surgical Procedure With Post Op Visit
Orthopedic denials usually start after surgery, not on the surgery date. The problem is global packaging. If your surgeon performs a major procedure and then sees the patient for an unrelated problem during the global period, the CMS-1500 has to show that distinction clearly or the E/M line gets bundled away.
Use a common scenario. The practice bills a surgical CPT for knee arthroscopy, then later bills an office E/M code such as 99213 for a separate complaint during the postoperative period. The second claim only survives if the record and modifier support that the visit is unrelated to the global surgery package.
How to build the unrelated E M claim correctly
Your surgery claim and your later E/M claim should never look like duplicates.
For the postoperative office visit:
- Item 24A: Use the actual date of the later office encounter.
- Item 24B: Use the office POS when the patient returns to clinic.
- Item 24D: Report the appropriate E/M code, such as 99213, with the modifier that identifies the service as unrelated to the original surgery when documentation supports it.
- Item 24E: Link the E/M to the diagnosis for the new or separate complaint, not automatically to the postoperative diagnosis.
- Item 24G: Enter one unit for the office visit unless payer policy requires otherwise. Coding discipline is important here. If the visit is routine postoperative care, don’t bill it. If it’s separately identifiable or unrelated, make the diagnosis and modifier tell that story without ambiguity.
The revenue impact of getting Item 24 right
Orthopedic benchmarks in CMS sample claim guidance showed that accurate Item 24G date handling significantly reduced multiple procedure payment reductions in orthopedic workflows. That’s a practical reminder that service-line precision affects payment logic well beyond simple code entry.
For practice owners, the takeaway is operational. Your orthopedic billers need a global period decision tree, not just a CPT book. Every postoperative visit should be sorted into one of three buckets:
- Included global care: Don’t bill separately.
- Separately identifiable E/M: Bill with the appropriate modifier when documentation supports it.
- Unrelated problem: Use the unrelated diagnosis and modifier combination that matches payer rules.
Operational takeaway: Review the diagnosis pointer before you review the modifier. If the diagnosis still looks postoperative, the payer will likely bundle the visit.
Most orthopedic leakage comes from weak claim construction, not weak surgery coding. A reliable internal reference for this is orthopedic billing global periods. If you’re comparing specialty outsourcing options, Happy Billing also maintains specialty workflows at happybilling.co/specialties.
4. Example 4 Cardiology EKG With Interpretation Split Billing
Cardiology groups lose money on EKG claims for a simple reason: they bill the test as one service when the payer expects two distinct billing rights. If your practice reads the tracing but does not own the equipment, billing the global code invites a denial. If you own the equipment and fail to bill the technical piece correctly, you leave revenue behind.
This specialty is exactly why generic government samples are not enough. A useful CMS-1500 example has to show who performed the test, who interpreted it, and which entity has the right to bill each component.
A practical split-billing claim pattern
Use a common office scenario. The patient receives a 12-lead EKG, and the cardiologist provides the interpretation and report. The claim can be billed as a global service only when the same qualified entity is entitled to both portions. Otherwise, split the service cleanly.
For the interpretation line:
- Item 24D: Report the EKG CPT code with modifier 26.
- Item 24J: Enter the rendering cardiologist’s NPI on that service line.
- Item 24E: Point to the diagnosis that supports the medical need for the interpretation.
- Item 32: List the actual service facility when the tracing was performed at a site different from the billing office.
For the technical line, if your group is allowed to bill it:
- Item 24D: Report the same EKG CPT code with modifier TC.
- Billing provider setup: Confirm that the billing entity owns or is permitted to bill the equipment-related component under payer rules.
- Box 33 and 33a: Make sure the billing provider name and NPI match the entity enrolled to receive payment for the technical portion.
Do not let billers guess. Confirm equipment ownership, supervision requirements, place of service, and whether the interpreting physician is billing under the same tax ID as the technical entity.
Where cardiology claims usually break
The failure point is rarely the CPT code itself. The failure point is claim construction.
A cardiology split-billing claim gets denied when the professional line lacks modifier 26, the technical line is billed by the wrong entity, or the diagnosis pointer in Item 24E does not support both services clearly. Another common error is a mismatch between Item 24J, Box 32, and Box 33a. If those fields describe different operational realities, the payer edit is usually correct.
This is the operational rule I recommend: review the ownership logic before you review the code. The code is easy. The billing right is what gets cardiology groups paid.
Operational takeaway: On every EKG claim, audit three fields together: Item 24D, Item 24J, and Box 33a. If the modifier, rendering NPI, and billing entity do not align, fix the claim before it leaves your system.
Teams that want fewer diagnostic denials should keep a quick reference for modifier 26 vs TC billing rules. In cardiology, that distinction decides whether you collect for the interpretation, the tracing, or neither.
5. Example 5 Primary Care Annual Wellness Visit With G2211
Primary care claim denials are usually caused by bad add-on logic, weak diagnosis linking, or incomplete authorization fields. The visit happened. The claim still fails because the CMS-1500 does not clearly support both the Annual Wellness Visit and G2211.
This matters more in primary care than in many other specialties. G2211 is not a routine extra line item. It is a payment signal that your practice is managing ongoing, longitudinal care complexity, and payers will scrutinize it that way. A generic sample form will not help much here. Your team needs a claim that is built to survive edits at the code and field level.
What the completed claim should show
Build this claim in two parts, then validate the relationship between them.
For the wellness service line:
- Item 24D: Report the correct AWV HCPCS code for the encounter performed.
- Item 24E: Point to the diagnosis that supports the preventive visit and any documented chronic condition context relevant to the encounter.
For the G2211 add-on line:
- Item 24D: Report G2211 on its own line only when the payer allows it and the documentation supports longitudinal care complexity.
- Item 24E: Link G2211 to the diagnosis or diagnoses that show the patient relationship and ongoing care management burden.
- Item 24G: Use the correct unit entry for the add-on line.
Then check the claim-level fields that often slow payment:
- Box 12: Confirm the patient authorization status is correctly captured.
- Box 27: Mark assignment of benefits correctly.
- Box 31: Keep the provider signature on file current.
- Box 33 and 33a: Match the billing provider name and NPI to enrollment records exactly.
Where primary care claims usually break
The denial point is usually not the AWV code. It is the logic connecting the AWV line to G2211.
If your biller adds G2211 without documentation of ongoing care complexity, the payer has a valid reason to deny it. If the diagnosis pointer supports the wellness visit but not the add-on, expect an edit. If Box 12 or Box 27 is wrong, the claim may pend or reject before anyone reviews the clinical merit.
Practice owners should put one rule in writing: never let staff append G2211 by habit. Require a chart-to-claim review standard for this code, especially in Medicare-heavy panels and high-volume preventive care workflows.
That review should also connect to your chronic care revenue strategy. Teams that bill AWVs and manage longitudinal conditions usually perform better when they standardize related workflows such as internal medicine CCM billing for recurring care management services.
Operational takeaway: Audit three elements together before submission: the AWV code in Item 24D, the G2211 diagnosis pointer in Item 24E, and the authorization and assignment fields in Boxes 12 and 27. If those four pieces do not support the same care story, fix the claim before it goes out.
CMS-1500: 5 Completed Case Examples
| Example | Implementation Complexity | Resource Requirements | Expected Outcomes | Ideal Use Cases | Key Advantages |
|---|---|---|---|---|---|
| Anesthesiology – Medically Directed Case (Modifier QK) | High – concurrency modifiers, precise anesthesia-time rules, payer-specific rounding | Anesthesiologist + CRNA, detailed anesthesia record, experienced coders, payer credentialing | Accurate anesthesia reimbursement and fewer denials when compliant; high audit risk if incorrect | Medically directed anesthesia with 2–4 concurrent CRNAs in OR cases | Ensures correct payment for medical direction and compliance with concurrency rules |
| Mental Health – Telehealth Therapy Session (Modifier 95) | Moderate – modifier and POS choices vary by payer; prior auths common | HIPAA-compliant video platform, authorization tracking, clinician documentation, coder knowledge of telehealth rules | Clean telehealth claims if POS/modifier and auth are correct; immediate denials if mismatched | Synchronous video psychotherapy for established patients | Enables remote care billing and preserves reimbursement when payer policies are followed |
| Orthopedics – Surgical Procedure With Post-Op Visit | High – global period rules and modifier -24 require strong justification and documentation | Surgeon documentation tied to distinct diagnosis, coding staff skilled in global period rules, audit-ready records | Payment for unrelated E/M during global period when well-documented; denials if linked to surgical diagnosis | Post-op visits for new, unrelated complaints within a 90-day global period | Recovers E/M revenue otherwise included in the surgical global package |
| Cardiology – EKG With Interpretation (Split Billing) | Low-Moderate – consistent use of -TC and -26 and rendering NPI required | Practice-owned equipment or facility, technician, interpreting physician NPI, billing system supporting split lines | Proper split reimbursement between technical and professional components; fewer modifier errors | Tests where facility/tech performs TC and physician provides interpretation (e.g., clinic EKG) | Maximizes revenue by billing correct components and clarifies billing responsibility |
| Primary Care – Annual Wellness Visit With G2211 | Moderate – correct diagnosis linking and CMS restrictions (no -25) | Detailed chronic-condition documentation, Medicare-specific coding expertise, AWV workflow integration | Additional Medicare payment for cognitive/longitudinal management when properly linked; denials if misused | Medicare AWV for patients with multiple chronic conditions needing longitudinal management | Captures add-on payment for complexity of care and recognizes ongoing management burden |
Key Takeaways for a Denial-Proof CMS-1500 Workflow
A denial-proof example of cms 1500 form completed isn’t a pretty form. It’s a disciplined workflow. The practices that get paid faster don’t rely on memory. They build specialty-specific claim rules around the handful of fields that decide whether the payer accepts, pends, or denies the claim.
Start with the fields that repeatedly control payment. Box 21 for diagnoses. Box 23 for authorization. Item 24D for CPT and modifiers. Item 24E for diagnosis pointers. Item 24J for rendering NPI. Box 27 for assignment. Box 31 for signature on file. Box 33a for billing NPI. Those boxes carry most of the financial risk on professional claims.
The examples above show why generic training fails. An anesthesia claim lives or dies on units, concurrency, and modifiers like AA, QK, or QS. Mental health depends on authorization details, telehealth logic, and diagnosis linkage for codes like 90837 and 90791. Orthopedics requires global-period judgment and correct post-op modifier use on E/M services such as 99213. Cardiology needs clean component billing with 26 and TC. Primary care has to support add-on logic and assignment handling when billing wellness services with G2211.
Build your internal process around these actions:
- Create specialty claim templates: Don’t use one universal CMS-1500 workflow for every department.
- Scrub modifiers before release: Most revenue leakage shows up as a modifier issue before it ever becomes an appeal.
- Match diagnosis pointers to medical necessity: If Item 24E is wrong, the rest of the claim is often irrelevant.
- Validate rendering and billing NPIs: Misalignment between 24J and 33a creates avoidable rejections.
- Control authorizations at scheduling: Claims with missing auth data usually shouldn’t reach billing.
- Keep payer rule cards by specialty: Your team needs quick access to rules for telehealth, global periods, anesthesia concurrency, and split billing.
The difference between a paid claim and a denied claim is often one field, not one visit.
This is why owners should audit denial patterns by box, not just by payer. If denials cluster around Box 23, fix authorization intake. If they cluster around Item 24D, tighten coding review. If they cluster around 24J or 33a, look at provider enrollment and claim build logic.
A high-functioning RCM partner should already operate this way. Happy Billing combines specialty workflows, human auditors, and AI-driven claim review to catch coding, modifier, and authorization problems before submission. If your team is still correcting the same CMS-1500 mistakes after remits come back, the workflow is the problem.
Happy Billing helps specialty practices turn CMS-1500 accuracy into faster payment. If your anesthesiology, mental health, cardiology, orthopedic, or primary care group needs tighter claim construction, denial prevention, A/R recovery, or specialty-specific billing support, visit Happy Billing to see how its RCM team works inside your current EHR and keeps claim velocity high without adding administrative drag.
FAQ What is the best example of cms 1500 form completed for training staff
The best training example is one built from your own specialty and payer mix. A generic sample won’t teach anesthesia concurrency, behavioral health authorization handling, orthopedic global periods, cardiology component billing, or primary care add-on code logic.
FAQ Which CMS-1500 boxes cause the most denials
For most physician practices, the highest-risk fields are Box 21, Box 23, Item 24D, Item 24E, Item 24J, Box 27, Box 31, and Box 33a. Those fields control diagnosis support, prior auth, modifier use, rendering identity, assignment, and billing identity.
FAQ Can I use the same completed CMS-1500 example for every specialty
No. The form is standardized, but denial risk is specialty-specific. A mental health telehealth claim and an anesthesiology claim may use the same form, yet the coding, modifier, authorization, and payer edit logic are completely different.
FAQ When should a CMS-1500 claim be sent electronically instead of on paper
If the claim exceeds six service lines, the CMS-1500 version 02/12 specification requires electronic resubmission through 837P, as noted in the completed anesthesiology CMS-1500 case material. Even when paper submission is technically possible, most practices should standardize electronic workflows for cleaner edits and faster correction cycles.