What Is RCM in Medical Billing & Why It Matters
Revenue Cycle Management, or RCM, in medical billing is the full financial process that tracks a patient account from registration through coding, claim submission, denial management, and final reimbursement. It goes far beyond billing alone, and a healthy practice typically targets a first pass payment ratio of 80% or higher, while low first-pass performance creates rework, delays cash flow, and ties up staff time.
That’s the counterintuitive part. Many practices think their revenue problem starts after the claim is sent. In reality, the money is usually lost much earlier, at registration, eligibility, authorization, documentation, or coding. By the time a payer rejects a claim with a front-end mistake attached, the practice is already paying twice for the same work.
When people ask what is rcm in medical billing, the useful answer isn’t “it’s the billing process.” It’s that RCM is the operating system for getting paid correctly, quickly, and consistently. Billing is one task inside that system. If you treat the two as interchangeable, you usually outsource claim submission and keep the hardest financial work in-house by accident.
RCM Is Not Medical Billing
A practice can have a competent biller and still have weak RCM. That happens when claims go out on time, but eligibility isn’t verified properly, prior authorizations aren’t tracked, denials sit untouched, and old A/R ages because nobody owns recovery.
Medical billing is the narrower function. It converts documentation into codes, prepares claims, submits them, posts payments, and issues patient balances. RCM is broader. It includes the front-end controls that prevent denials, the back-end processes that recover revenue, and the management discipline that keeps the whole cycle moving.
That distinction matters because many vendors sell “billing” when a practice needs full-cycle financial management. The operational gap is straightforward. If your vendor only submits claims, your staff still owns denial management, aged A/R recovery, and revenue integrity work that directly affects cash flow. This overview of what medical billers do is useful because it shows how narrow the billing role can be compared with the larger RCM function.
Where practices usually get misled
The most common mistake is assuming that a clean claim starts in the billing office. It doesn’t. It starts at intake.
A wrong member ID, a missed authorization requirement, or a bad modifier can kill a claim before payment posting is even relevant. In anesthesiology, that may be a concurrency-related modifier issue such as QK or QX. In behavioral health, it may be a service that should never have been scheduled without benefit verification. In orthopedics, it may be a post-op encounter incorrectly billed during a global period.
Practical rule: If a vendor can’t explain who owns denials, old A/R, and payer follow-up, you’re not looking at full RCM.
The stronger question for an owner or practice manager isn’t whether you need billing help. It’s whether the team handling your revenue cycle covers the entire cycle, including prevention, recovery, and collections. That distinction is the difference between transaction processing and financial control, as discussed in Aspirion’s comparison of revenue cycle management versus medical billing.
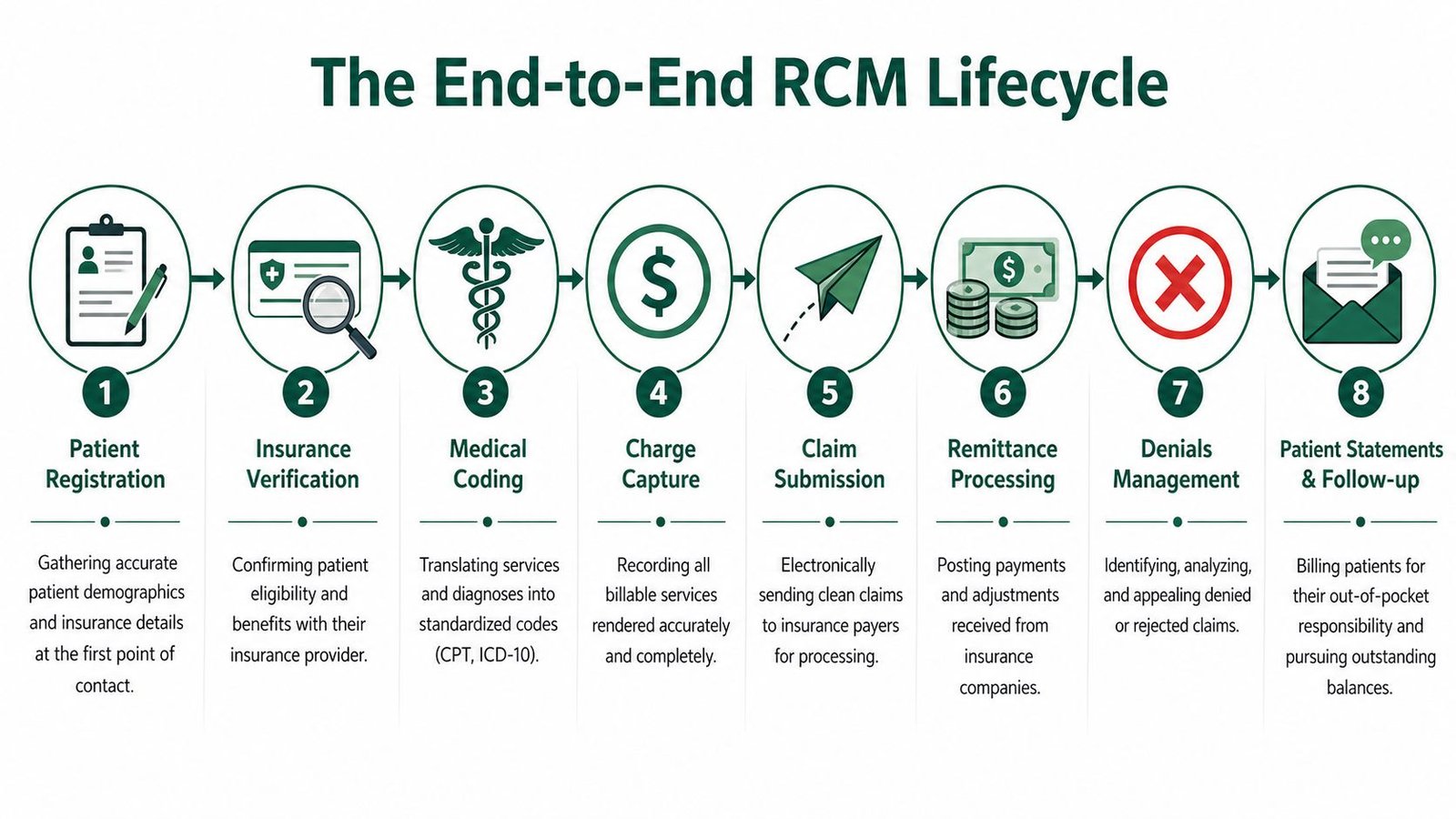
The End-to-End RCM Lifecycle Explained
The easiest way to understand what is rcm in medical billing is to follow one patient account from first contact to zero balance. Every handoff matters. A small error in one step often creates extra work in three later steps.
Front-end controls that determine claim quality
The first phase is pre-service. Some RCM models call this Order to Intake. During this phase, staff collect demographics, confirm insurance, verify eligibility, check benefits, and secure prior authorization when required.
If your front desk enters the wrong subscriber data, the claim may never become a true receivable. It becomes rework. The same applies when a payer requires authorization for a mental health service and the visit proceeds without one. The coder may assign the right CPT code, but the account still starts life broken.
A practical example is an office visit billed with 99214 and linked to proper diagnosis coding, but attached to an inactive plan because eligibility wasn’t verified on the date of service. The coding can be perfect. The claim still stalls.
Mid-cycle work where documentation becomes revenue
The second phase is often called Care to Claim. This includes charge capture and coding. It’s where services, supplies, procedures, and diagnoses are translated into ICD-10, CPT, and HCPCS language and checked for compliance. Medusind’s end-to-end RCM overview notes that this phase carries direct risk from incorrect coding, upcoding, and downcoding, and that integrated workflows can eliminate manual rework cycles that delay collections by 2–8 weeks.
At this point, specialty knowledge stops being optional.
In anesthesiology, the coder has to get the base units, time units, and modifiers right. A claim using 01967 for labor epidural anesthesia with the wrong direction modifier can trigger rejection or underpayment. Modifier choice such as QK, QY, QX, or AA isn’t cosmetic. It changes how the claim is processed.
In cardiology, a diagnostic or interventional service may need careful modifier logic to show whether services are distinct or bundled under payer edits. In orthopedics, coding around surgical follow-up is inseparable from global period rules. In mental health, authorization status often matters before coding even begins.
Clean claims are built in the chart, confirmed at registration, and validated before submission. They aren’t rescued at the payment-posting stage.
A second mid-cycle risk is missed charge capture. If the provider performs billable work that never gets into the charge queue, there is no denial to appeal because no claim exists. That’s silent leakage, and it’s one reason integrated EHR charge capture matters.
For a practical audit framework, this revenue cycle management checklist is a good way to review whether your intake, coding, scrubbing, and posting steps are connected or operating as isolated tasks.
Back-end follow-through that actually gets the money in
The final phase is Claim to Payment. This includes claim submission, remittance processing, denial management, payment posting, patient statements, and A/R follow-up.
Here’s where many practices confuse activity with performance. Sending claims electronically isn’t the win. The win is getting them accepted and paid without avoidable touches. If a payer rejects a claim because modifier logic doesn’t match the procedure, or because the demographics fail a scrubber edit, your team now has to correct, rework, resubmit, and track the account again.
A disciplined back-end process usually includes:
- Claim scrubbing before transmission to catch payer-specific edits.
- Remittance review to confirm expected payment and adjustments.
- Denial classification so staff know whether the root cause was eligibility, coding, authorization, documentation, or filing logic.
- Patient balance follow-up after insurance adjudication and posting.
The most effective teams treat denials as operational feedback, not just billing tasks. If the same payer keeps rejecting claims for missing authorization, the fix belongs upstream. If the same CPT code keeps denying with modifier issues, the coding workflow needs correction.
Key RCM Metrics Your Practice Must Track
Revenue problems rarely start at month-end. They start in the daily metrics that show where claims stall, where staff rework piles up, and where payer behavior is draining cash.
A practice that tracks only collections will miss critical failure points. Full-cycle RCM requires measures that expose preventable denials, slow insurance follow-up, and weak A/R recovery. That is the difference between billing activity and revenue control.
First pass payment ratio
First pass payment ratio, or FPPR, shows how many claims get paid on the initial submission without correction or appeal. A low FPPR usually means the practice is losing money before the claim ever reaches payment posting.
In real operations, weak FPPR tends to trace back to a short list of recurring failures:
- incorrect patient or subscriber data entered at registration
- CPT, ICD-10, HCPCS, or modifier errors
- documentation that does not support medical necessity or code selection
- claims released before payer edits or specialty rules are fully checked
I watch FPPR closely because it exposes upstream discipline. If orthopedic claims keep failing for modifier logic, or anesthesia claims keep bouncing because direction documentation does not match the billed modifier set, the issue is not just billing. The workflow is broken.
Initial denial rate
Initial denial rate measures how often claims are denied on first submission. This metric deserves its own line on the dashboard because denial volume drives labor cost, slows collections, and creates avoidable A/R.
The useful question is not whether denials exist. Every practice has denials. The useful question is what kind of denials keep repeating.
Track denials by root cause and by payer. Separate eligibility failures from authorization denials, coding edits, filing deadline misses, and documentation problems. Then go one level deeper. A denial tied to modifier 59, 25, QK, or QX points to a different operational failure than a denial tied to COB errors or inactive coverage.
That level of classification is where full-cycle RCM earns its keep. Simple billing teams resubmit. Strong RCM teams find the pattern, assign ownership, and stop the leak at the source.
Days in A/R
Days in A/R measures how long it takes to convert charges into cash. If this number starts climbing, the practice is either carrying unresolved payer balances too long, struggling to collect patient responsibility, or both.
I do not treat Days in A/R as a standalone score. It matters most when you read it with aging buckets and payer mix. A practice sitting at an acceptable overall A/R number can still have a serious back-end problem if too much of its balance is sitting in over-90-day buckets or tied up with one high-volume payer. That is usually where underworked follow-up and weak denial recovery show up first.
Strong A/R performance depends on fast correction cycles, disciplined account follow-up, and staff who know which balances are worth pursuing aggressively. A $40 patient balance and a $4,000 underpaid surgical claim do not belong in the same work queue.
For a broader operating dashboard, these medical billing KPIs to track are useful if you want each metric tied to a specific owner, review cadence, and corrective action plan.
Why Generic RCM Fails Specialty Practices
Generic RCM sounds efficient until it touches specialty billing. Then it becomes expensive.
A generalist may know claim flow. That’s not enough when revenue depends on specialty-specific coding rules, modifier logic, authorizations, and payer edits. CareCloud’s discussion of how RCM improves medical billing points out the core problem well: anesthesiology, cardiology, orthopedics, and mental health don’t share the same billing workflow. Treating coding as monolithic is the mistake.
Anesthesiology isn’t just CPT plus time
Anesthesia billing depends on base units, time units, and concurrency rules. A generic team may know the anesthesia CPT family such as 00840, 01402, or 01967, but still miss what makes the claim payable. Modifier selection such as AA, QK, QY, or QX changes the claim profile.
If a team doesn’t understand medical direction rules and concurrency, they can submit a technically complete claim that still doesn’t match payer expectations. In this specialty, RCM has to include charge review, modifier validation, and documentation checks tied to the anesthesia record itself. Practices in that space should expect partner-level knowledge, not just coding familiarity. Happy Billing’s specialty pages show the kind of specialty-specific workflow questions you should be asking any vendor.
Cardiology and orthopedics break generic workflows fast
Cardiology groups deal with diagnostic imaging, interventional coding, and frequent payer edit scrutiny. A modifier issue on a cardiovascular procedure can trigger bundling problems, reduced payment, or rejection.
Orthopedics creates a different hazard. Consider CPT 27447 for total knee arthroplasty. The coding itself may be simple. The RCM challenge is the follow-up billing around the global surgical package. If the billing team doesn’t understand global period logic, post-op encounters that should be included may be billed separately, and separately billable services may be missed because staff assume everything after surgery is bundled.
Mental health rises or falls on authorization discipline
Behavioral health practices often have clean documentation and still struggle financially because the front-end authorization process is weak. A therapist can document the service correctly and the coder can submit the correct CPT code, but if the payer required authorization and the visit occurred without it, the claim starts in trouble.
That’s why generic “we handle all specialties” messaging usually fails under pressure. Real RCM specialization means the workflow itself changes by specialty. The scrubber rules change. The denial patterns change. The reporting priorities change. The training priorities change.
A family practice billing playbook won’t protect an anesthesia group, and an anesthesia workflow won’t fix behavioral health authorization failures.
Outsourcing RCM When to Partner and What to Avoid
Outsourcing RCM fixes cash flow only when the partner takes ownership of the parts of the cycle that leak revenue. A vendor that only pushes claims out the door gives you activity, not control. The result is predictable. Denials stay high, old A/R ages, underpayments sit untouched, and your staff keeps doing cleanup work you thought you outsourced.
The right partner shortens the time from date of service to payment because they manage the full cycle. That means front-end accuracy, coding discipline, denial follow-up, appeal strategy, and recovery of aging accounts. Medical billing covers claim submission and payment posting. Full-cycle RCM goes further. It finds why claims fail, who owns the fix, and how to stop the same loss from repeating next week.
Green flags in an RCM partner
Ask direct questions. A capable partner should answer them without vague promises or generic dashboards.
- They own front-end accuracy: They can show how staff validate demographics, eligibility, coordination of benefits, and prior authorization before the visit or procedure.
- They manage coding quality: They use certified coders, audit regularly, and explain how they handle ICD-10, CPT, HCPCS, modifiers, and payer edits by specialty.
- They work denials as a core function: They do not leave CARC and RARC follow-up sitting in your office. They have denial queues, appeal workflows, and root-cause reporting.
- They pursue old A/R and underpayments: They can explain how they segment aging buckets, escalate timely filing risk, and identify payer underpayments against contracted rates.
- They fit your systems and workflow: Charge capture, documentation flow, and payment posting need to match how your practice operates, not how a generic vendor wants you to operate.
- They report operational causes: They can tell you whether the leak starts in registration, authorization, coding, documentation, claim edits, or payer adjudication.
If you are comparing service models, this in-house vs outsourced medical billing guide is a useful reference point.
Red flags that usually lead to leakage
Some outsourcing failures are obvious before go-live.
| Red flag | Why it matters |
|---|---|
| “We mainly focus on claim submission” | Claim submission alone does not fix denials, aged A/R, or underpaid claims |
| Vague specialty experience | Specialty-specific rules drive payment. Generic workflows miss authorization, modifier, and documentation issues |
| No denial taxonomy | If they cannot categorize denials by cause and payer, they cannot reduce them |
| Reporting only on collections | Collections tell you what came in, not what stalled, wrote off, or was never appealed |
| No process for old A/R recovery | Money older than 60 or 90 days needs a different work strategy than fresh claims |
| No explanation of payer-rule configuration | A scrubber without payer-specific logic still lets preventable edits through |
I look for one thing first. Can the vendor explain how they reduce avoidable denials in your specialty, then recover the claims that still fail? If they cannot answer that clearly, they are not offering real RCM. They are offering outsourced billing labor.
The strongest outsourcing relationships bring discipline to the entire revenue cycle and give the practice owner visibility into where cash gets stuck. The weak ones hide behind claim volume while financial leakage continues in denials, rework, and aging A/R.
The Modern RCM Solution AI Agents Plus Human Expertise
The strongest RCM model now is hybrid. Software handles speed, repeatability, and edit detection. Human experts handle nuance, payer behavior, documentation ambiguity, and specialty judgment.
AI-driven workflows are well suited for repetitive front-end and pre-submission work. They can check demographics, flag eligibility mismatches, run payer-rule edits, and surface likely coding conflicts before a claim goes out. That’s how practices protect first-pass performance at scale. In a well-run operation, those tools support the kind of 98%+ first-pass clean claim performance referenced in the verified data.
Human expertise still decides the hard cases. A denial tied to anesthesia concurrency, an orthopedic post-op billing dispute, or a mental health authorization breakdown usually needs someone who can read the chart, interpret the payer issue, and choose the right correction or appeal path. Machines can flag the account. They can’t own the accountability.
Where the hybrid model works best
The practical split looks like this:
- AI agents handle volume: eligibility checks, claim scrubs, work queues, and error flagging
- Human coders and RCM specialists handle complexity: modifier logic, denial appeals, underpayment review, and specialty-specific corrections
- Leaders use the output to manage the business: not just close tickets, but identify where leakage starts
For practices trying to modernize without replacing their entire stack, technology for revenue cycle is where the conversation should start. The right question isn’t whether software can do RCM alone. It can’t. The right question is whether your technology and your people are assigned to the work they each do best.
Frequently Asked Questions About RCM
Is RCM the same thing as medical coding
No. Medical coding is one function inside RCM. Coding converts documentation into ICD-10, CPT, and HCPCS codes. RCM includes coding, but also registration, eligibility, authorization, charge capture, claim submission, payment posting, denial management, A/R recovery, and patient balance follow-up.
Can a small practice benefit from full-cycle RCM
Yes. Smaller groups often feel denial and cash-flow delays more sharply because fewer people are carrying more operational responsibility. Full-cycle RCM matters even more when the same front-desk team is scheduling, verifying insurance, collecting copays, and answering phones. The smaller the margin for error, the more valuable a disciplined process becomes.
What should I ask an outsourced RCM vendor first
Ask who owns denials, aged A/R, and payer follow-up. Then ask how they handle specialty-specific coding issues such as anesthesia modifiers, orthopedic global periods, cardiology procedural edits, or behavioral health authorizations. If the answers stay general, expect general results.
What’s the clearest sign my current RCM process is weak
Look at first-pass performance and A/R speed. If claims are paid only after repeated corrections, or if accounts sit unresolved well beyond the pace of a healthy cycle, the process is leaking. The fix usually starts upstream with eligibility, documentation, coding accuracy, and payer-rule validation rather than with more aggressive follow-up alone.
If your practice needs a revenue cycle partner that handles the full process instead of just pushing claims out the door, Happy Billing is built for that job. The team supports specialty-specific RCM workflows, works inside your existing EHR, and combines AI-driven claim preparation with human experts who manage denials, A/R recovery, and complex coding issues that generic billing services often miss.