What Do Medical Billers Do? Protect Practice Cash Flow
TL;DR: Medical billers manage the full revenue cycle so the practice gets paid correctly and on time. In physician offices alone, 69,840 billing and posting clerks were employed in May 2023 with an annual mean wage of $45,760, and the field is projected to grow 8% from 2022 to 2032 according to medicalbillingandcoding.org’s summary of BLS data.
Medical billers create claims, verify coverage, post payments, resolve denials, reconcile A/R, and handle patient balances. In a well-run group, they are not back-office data entry. They are the people who protect cash flow every day.
If your schedule is full but collections still feel uneven, the billing function is usually where the story becomes clear. The question isn't just what do medical billers do. The better question is whether your billers are routinely moving claims, or actively guarding revenue.
The Core Engine of Your Practice's Revenue
Monday morning, the schedule is full, providers are seeing patients on time, and the front desk feels productive. By Thursday, deposits are light, aging has inched up, and three large claims are stuck for reasons nobody can explain quickly. That gap between clinical work and collected cash is the biller's territory.
A medical biller manages the financial path of care from registration through reimbursement. The work includes insurance verification, charge review, claim preparation, submission using code sets such as ICD-10, payment posting from EOBs and ERAs, denial follow-up, A/R reconciliation, patient balance handling, and compliant communication under HIPAA. On paper, those tasks look administrative. In a functioning practice, they directly shape days in A/R, net collection rate, and how much staff time gets burned fixing preventable rework.
The strongest billers operate like financial detectives. They trace where revenue is likely to leak, then stop the leak before it shows up on the aging report. A missing authorization, weak diagnosis linkage, an invalid modifier, an unbilled secondary, or an underpayment that slips through once can turn into repeated losses across dozens of encounters.
What the role really controls
A strong biller controls three outcomes that matter to ownership and management:
- Cash timing: Claims go out quickly, with fewer front-end edits and fewer preventable holds.
- Cash accuracy: The claim matches the documentation, payer rules, and contract terms closely enough to support full payment.
- Cash recovery: Denials, underpayments, credit balances, and missed patient balances are worked before they age into write-offs.
A clean claim has a better financial profile than one with avoidable errors that requires later intervention. Every touch after first submission adds labor cost, slows cash, and raises the odds that the balance will never be fully recovered.
That is the difference between a biller who processes transactions and a biller who protects margin. In my experience, average billers move what they receive. Strong billers question weak documentation, catch missing pieces before submission, and recognize payer behavior patterns early enough to prevent repeat losses.
Why practice managers should treat billing as a revenue function
The staffing footprint alone shows how common and operationally important this role is. The U.S. Bureau of Labor Statistics lists medical records specialists, a category that includes billing and related revenue cycle work, with projected job growth of 9% from 2023 to 2033, faster than average for all occupations, according to the BLS Occupational Outlook Handbook for medical records specialists.
For a practice manager, the more useful question is not how many people hold billing jobs nationally. It is whether your biller is producing measurable financial results. Good performance usually shows up as low initial rejection volume, disciplined follow-up, tight posting controls, and limited old A/R. Weak performance shows up as claims sent without scrutiny, denials touched too late, secondary balances left open, and patient A/R that drifts because nobody owns the handoff.
If you want a practical framework for evaluating that workflow, review this guide to RCM for physician practices. The biller sits in the center of that operating system, guarding revenue one claim, one payment, and one correction at a time.
A Day in the Life From Charge Entry to Payment Posting
The biller's day starts earlier than many practice owners assume. It doesn't begin when a denial arrives. It begins when the appointment is scheduled and the practice has a chance to shape the claim before the encounter ever happens.
Medical billers can initiate the coding and claims workflow as soon as the patient schedules. That front-end approach supports pre-authorization, payer rule checks, and real-time patient liability estimates so the practice can collect patient responsibility at the time of service rather than chasing it after the visit, as described by Ultimate Medical Academy’s overview of medical coding and billing specialists.
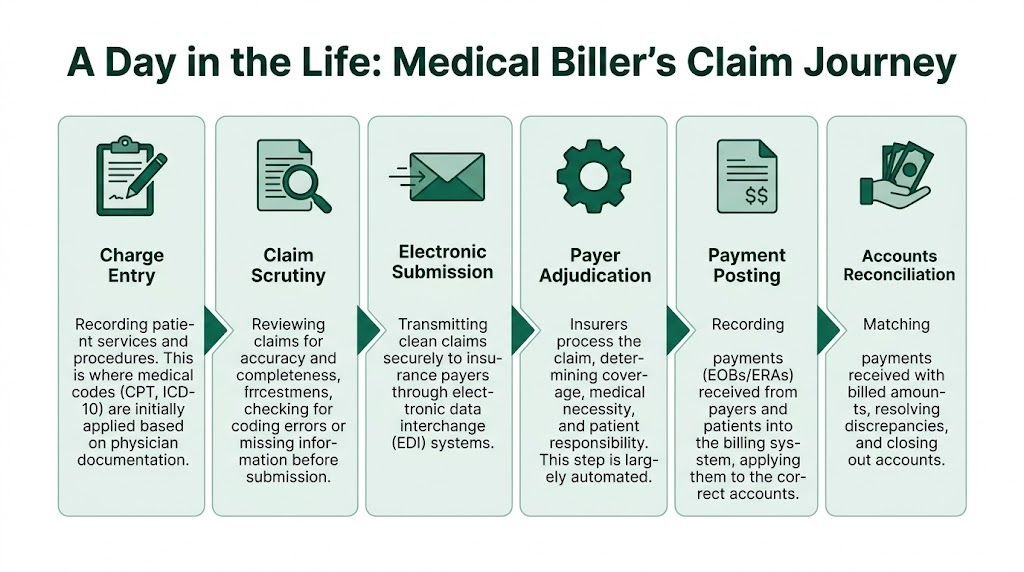
Step one is cleaner than people think
Charge entry isn't just typing in codes from a superbill. The biller has to decide whether the data package is strong enough to survive payer edits.
In anesthesiology, that means more than dropping an ASA code onto a claim. If the service is ASA 01402 for anesthesia related to a total knee arthroplasty, the biller needs supporting diagnosis linkage, anesthesia time documentation, physical status if applicable such as P3, and the right modifiers to reflect the service circumstances and payer expectations. If the documentation is thin or the timing sequence doesn't reconcile, the problem starts before transmission.
In cardiology, a claim built around CPT 93015 has to reflect the full global stress test when all components were performed and billed together. If the components were split across entities, the biller has to avoid accidental unbundling and match the claim to the actual service arrangement. That isn't generic data entry. That's rule application.
Claim scrubbing is where money is protected
Most clean claim performance is won before submission. Billers review demographic accuracy, payer ID selection, diagnosis-to-procedure consistency, modifier usage, authorization status, provider credentialing status, place of service, and whether payer-specific edits apply.
A few examples from day-to-day work:
- Modifier review: If a procedural pair may require modifier 59, the biller has to confirm the documentation supports a distinct procedural service under CMS and payer policy. Using 59 as a shortcut is how claims get denied and audited.
- Behavioral health timing: If a therapist bills CPT 90837, the biller has to verify the session length is documented and that the payer's benefit rules support that code for the member and rendering provider.
- Secondary billing logic: After primary adjudication, the biller has to make sure crossover happened correctly or submit secondary claims with the proper EOB data.
Clean claims aren't the result of luck. They're the result of someone checking what the payer will reject before the payer has to tell you.
Submission, posting, and reconciliation
After scrubbed claims pass internal review, billers submit them electronically through the practice management system or clearinghouse. If you want to see the data structure they are building toward, this example of a completed CMS-1500 form is useful for managers training staff on claim fundamentals.
Once payers adjudicate, the biller posts ERA or EOB payments, adjustments, denials, deductibles, and coinsurance to the correct accounts. Then comes reconciliation. Posted dollars must tie back to billed services, contractual expectations, and patient balances.
Where good billers save the most time
The most effective billers don't just post and move on. They look for patterns such as:
- recurring edits tied to one provider or location
- missing authorizations from one referral source
- underpayments on a specific CPT family
- claims stuck because one payer ID or taxonomy was entered incorrectly
That pattern recognition is what turns a biller into a revenue guardian.
Mastering Denial Management and Payer Communication
The clean claim path is only half the job. The other half is recovering money that is already at risk.
A core duty of medical billers is denial management, including denial investigation, correction, resubmission, and formal appeal with supporting evidence. Insurance complexity can drive initial denial rates up to 20-30% in some sectors, and that complexity is one reason the profession is projected to grow 8% through 2032, according to CareerStep’s medical billing job market overview.
Denial work starts with categorization
An experienced biller doesn't treat all denials the same. They sort them into operational buckets because each bucket points to a different failure point.
| Denial type | What the biller checks first | Typical action |
|---|---|---|
| Eligibility or coverage | Effective dates, plan status, subscriber data | Correct data, rebill, or redirect balance |
| Authorization | Referral, auth number, units, service dates | Obtain retro review if allowed, submit corrected claim, or appeal |
| Coding or modifier | CPT, ICD-10 linkage, NCCI-related issues, modifier support | Review note, correct coding, add records, or appeal |
| Medical necessity | Policy criteria, diagnosis support, documentation depth | Submit records and policy-based appeal |
| Timely filing | Submission history and rejection logs | Prove timely filing or write off if not defensible |
This is why weak A/R follow-up hurts so badly. If the person working denials can't identify the root cause quickly, the account ages while everyone waits on the wrong next step.
Real examples of detective work
Take a behavioral health denial on CPT 90837 for "exceeding plan limits." A weak process resubmits the same claim and waits for the same denial. A strong biller checks the patient's benefit structure, confirms whether authorization was required, verifies whether that plan limits the code by diagnosis, provider type, or frequency, then calls the payer with the exact claim number and benefit question.
If the payer made the error, the biller documents the call reference and pushes reprocessing. If the denial is tied to missing records, the biller sends a targeted packet instead of dumping the whole chart. If the service exceeded benefit limitations, the biller escalates the patient balance correctly and closes the payer path.
Now take orthopedics. A surgeon bills two procedures and one line uses modifier 59. The payer denies one line as bundled. The biller has to go back to the op note, determine whether the services were distinct under CMS guidance and the payer's own edit logic, and support the claim with operative detail. If the note doesn't support distinct work, appealing is wasted effort. If it does, the appeal should say so directly.
The best denials teams don't ask, "Can we appeal this?" They ask, "What evidence would make the payer reverse this?"
Payer communication is a skill, not a courtesy task
Calling a payer isn't the work. Getting to an actionable answer is the work.
Effective billers prepare before contacting the payer:
- They have the exact identifiers ready: claim number, DOS, billed CPT, rendering NPI, and denial code.
- They ask narrow questions: not "Why was this denied?" but "Was this denied for missing authorization, exhausted benefits, or unsupported modifier use?"
- They document every touch: representative name, reference number, next action, and deadline.
That documentation matters because appeals live or die on the paper trail. If the payer gave inconsistent guidance on two separate calls, the biller should preserve both references.
For teams trying to improve this process, this guide to medical billing denial management is a strong operational checklist.
What doesn't work
Three habits sink denial recovery:
- Blind rebilling without fixing the root problem
- Late follow-up after appeal windows have already narrowed
- No denial trend reporting by payer, code family, provider, or site
A biller who only "touches" accounts is not protecting revenue. A biller who identifies denial patterns, coordinates with coding and clinical teams, and builds defensible appeals is doing the job at a high level.
Biller Coder and RCM Manager Demystified
Practice owners often blend these roles together, then wonder why no one has full accountability. The coder, the biller, and the RCM manager all touch the same revenue stream, but they are solving different problems.
The simplest way to separate them is this. The coder translates documentation into billable language. The biller turns that coded encounter into collected cash. The RCM manager monitors the whole machine, finds bottlenecks, and drives corrective action.
Role comparison
| Role | Primary Focus | Key Performance Indicator (KPI) | Core Tools |
|---|---|---|---|
| Biller | Financial outcome after the encounter. Submission accuracy, payment posting, denial follow-up, A/R cleanup | Clean claims, aged claims movement, denial resolution, payment accuracy | Practice management system, clearinghouse work queues, payer portals, ERA/EOB posting screens |
| Coder | Clinical accuracy and code assignment based on documentation | Coding accuracy, documentation support, modifier correctness, audit defensibility | EHR charts, CPT and HCPCS references, ICD-10 resources, AAPC-style coding guidance |
| RCM Manager | Strategic oversight across front end, coding, billing, payer mix, and collections | Trend visibility, workflow adherence, root-cause correction, team accountability | Dashboards, aging reports, denial reason reports, payer matrixes, workflow audits |
Where practices get confused
A coder may know whether 93015 should be billed globally or split by component, but the coder usually isn't the person chasing a payer underpayment weeks later. A biller may know a claim denied for modifier use, but the biller shouldn't independently rewrite coding logic that isn't supported by the chart. The RCM manager decides whether this is a training problem, a template problem, a payer policy issue, or a staffing problem.
That distinction matters most in high-variance specialties. In anesthesiology, coding judgment touches time units, physical status, and modifier logic. Billing judgment touches whether the payer processed the units correctly and whether concurrency-related issues need follow-up. Management judgment decides whether denials are tied to one facility, one payer, or one recurring documentation gap.
The handoff has to be tight
Most revenue leakage happens at role boundaries. The coder thinks the claim is clean because the code set is technically valid. The biller knows the payer rejects that exact setup unless the note includes one additional element. The RCM manager sees a trend but doesn't have a closed-loop process to fix it.
A high-functioning revenue cycle isn't built on job titles. It's built on clean handoffs and clear ownership.
In practical terms, managers should expect:
- coders to defend code selection,
- billers to defend collection action,
- and RCM leadership to defend process performance.
If one person is doing all three jobs, the risk isn't just workload. It's blind spots.
The KPIs That Separate Good Billers from Great Ones
Most practices say billing is "fine" because claims are going out and money is coming in. That's not enough. If you can't measure billing performance, you can't tell whether revenue is being protected or merely delayed.
One of the biggest blind spots in medical billing content is the lack of quantified operating benchmarks for errors and A/R performance. That gap matters because practices can't evaluate the return on better billing operations without a scorecard, as discussed in University of Providence’s medical biller overview.

The metrics that matter most
In high-performance billing operations, four KPIs tell you most of what you need to know:
- Clean claim rate measures how often claims leave the practice ready to process without preventable edits.
- Days in A/R shows how long receivables are sitting before they convert to cash.
- Denial rate reflects how often claims hit payer resistance after submission.
- Net collection rate shows how much of the allowed reimbursement the practice is capturing.
The practical targets many strong RCM teams use are clean claim rate above 98%, Days in A/R under 35, denial rate under 5%, and net collection rate above 95% of allowed amount. These are operational benchmarks used by high-performing billing partners and mature internal teams, and they are best treated as management targets rather than published industry averages.
What each KPI is really telling you
A weak clean claim rate usually means your front end and coding edits are loose. The claim may still get paid eventually, but the practice has already lost time.
High Days in A/R usually points to one or more of these issues:
| KPI problem | Likely operational cause |
|---|---|
| A/R trending older | poor follow-up cadence, unresolved denials, delayed claim release |
| denial rate drifting up | front-end errors, authorization misses, unsupported modifiers |
| net collection softness | underpayments ignored, write-off discipline weak, patient balance process inconsistent |
A denial rate problem doesn't always mean your billers are failing. Sometimes it means they are exposing a bigger weakness elsewhere, such as poor documentation or sloppy authorization intake. Great billers surface that quickly instead of merely reworking the same claims.
What good looks like operationally
You don't need vanity dashboards. You need reporting that a practice manager can act on this week.
Ask your billing lead these questions:
- What are our top denial reasons by payer?
- Which CPT families are generating the most follow-up work?
- Which providers or locations create the most front-end corrections?
- How quickly are denials being touched and resolved?
If the answers are vague, your team isn't managing by KPI. They're managing by inbox.
For a practical framework, this guide to medical billing KPIs to track can help managers structure reporting that drives decisions.
Red Flags in Your Billing Operations and When to Outsource
Monday starts with a full schedule, but last week's money is still missing. Claims were submitted, yet cash has not posted the way it should. By noon, your biller is buried in portal checks, a few denials were reworked without a clear appeal path, and no one can tell you whether the delay came from front-end intake, coding, payer edits, or follow-up failure. That is the point where billing stops being an admin function and becomes a revenue risk.
Weak billing operations rarely break in one dramatic moment. They leak cash through delay, rework, underpayments, and preventable write-offs. A strong biller catches those leaks early. They act like a financial detective on the front end and a revenue guardian once the claim is out the door.
Operational warning signs you shouldn't ignore
Look for patterns that affect cash, not just workload:
- A/R aging keeps rising: Staff activity may be high, but collections are slowing. That usually means claims are leaving late, follow-up is inconsistent, or denials are sitting too long before action.
- Denied claims are being resubmitted without a documented strategy: A good appeal includes payer-specific reasoning, records when needed, and a tracked next step. Blind resubmission burns time and often delays payment another cycle.
- No one can name the top denial reasons by payer: If your team cannot break denials down by payer, service line, or provider, it is operating without control points.
- Authorization-heavy services keep failing medical necessity or referral requirements: In specialties with complex prior auth rules, one missed requirement can wipe out the margin on an otherwise profitable visit or procedure.
- Modifier use is inconsistent: Errors around 59, NCCI edits, bundling logic, and specialty-specific coding rules create avoidable denials and compliance exposure.
- Payment posting is delayed or sloppy: You cannot pursue the right balances, identify underpayments, or keep patient statements accurate if remits are not posted correctly.
- Underpayments are accepted without review: Small payer shortfalls add up fast across high-volume CPTs.
- One or two employees hold all the operational memory: If one person leaves and clean claim performance drops, the process was never stable.
These issues show up fastest in specialties with tighter reimbursement rules. Cardiology is a common example because procedural coding, payer edits, and documentation requirements leave little room for generalist billing. If that sounds familiar, the specialty examples on Happy Billing’s cardiology billing page show why generic support often misses revenue.
The staffing market makes weak processes more expensive
Hiring alone does not fix this. Practices need billers who can read an ERA closely, spot payer behavior patterns, distinguish a coding problem from an eligibility problem, and protect cash without creating compliance trouble. That level of judgment is harder to hire, train, and retain than many managers expect.
As noted earlier, the labor market for experienced billing staff is tight. The practical consequence is straightforward. Open roles stay open longer, specialty knowledge gets concentrated in too few people, and turnover creates backlogs that show up in A/R within weeks.
When outsourcing makes operational sense
Outsourcing is usually worth serious consideration when the financial downside of the current model is already visible:
- Your specialty rules are outpacing your team's expertise. Anesthesiology concurrency, behavioral health authorization workflows, orthopedics global periods, and cardiology procedure logic all require billing judgment, not basic claim handling.
- Leadership cannot get reliable operating visibility. If reports on denials, aging, lag days, and follow-up activity are inconsistent, you cannot manage performance or hold anyone accountable.
- The team spends its time reacting. Preventable denials keep coming back, staff work queues stay full, and the same claims get touched multiple times before resolution.
- Turnover keeps interrupting collections. Every staffing change creates training drag, release delays, and a temporary drop in follow-up quality.
Effective outsourcing solves a capability gap and gives the practice stronger process discipline at the same time.
A good RCM partner should bring specialty fluency, daily work coverage, cleaner reporting, and tighter denial management. It should also show you measurable operating improvement. Cleaner claim acceptance, faster denial touch times, better underpayment recovery, and more consistent posting discipline are the benchmarks that matter. If those do not improve, the vendor is just moving the same problems to a different inbox.
If you're assessing options, use this checklist of medical billing company red flags before you sign anything.
Taking Control of Your Revenue Cycle
Medical billers do far more than submit insurance claims. They protect timing, accuracy, and recoverability across the entire reimbursement process. In a healthy practice, they are financial detectives on the front end and revenue guardians on the back end.
For a practice manager, that means two things. First, you need to know exactly what work your billing team is doing beyond claim submission. Second, you need to know whether that work is producing the right financial outcome. If you can't see that clearly, you're not really managing the revenue cycle.
The most useful next step is simple. Audit one month of billing activity with fresh eyes. Review how charges enter the system, how modifiers are validated, how many claims go out clean, how quickly denials are touched, and whether payment posting leads to actual account resolution. The goal isn't to blame staff. The goal is to find where cash slows down.
Once you do that, the answer to what do medical billers do becomes concrete. They don't just move paperwork. They decide whether the practice gets paid cleanly, slowly, partially, or not at all.
How can I tell if my biller is doing strategic work instead of basic data entry
Ask for evidence of decision-making, not just volume. A strategic biller can explain top denial reasons, show how claims are being corrected before submission, identify recurring payer issues, and document appeal outcomes with clear rationale.
Should one person handle both coding and billing
Sometimes, but only if the practice is small and the specialty is simple. In complex specialties, combining the roles often creates blind spots because the same person is trying to interpret documentation, apply code logic, submit claims, and chase payment without a second layer of review.
What billing tasks have the biggest effect on cash flow
Front-end insurance verification, authorization capture, claim scrubbing, fast claim release, accurate payment posting, and disciplined denial follow-up usually have the biggest effect. Those are the tasks that influence whether the practice collects at time of service, gets paid quickly by the payer, or loses time in rework.
Which specialties need the strongest billing expertise
The specialties with the most payer nuance and modifier sensitivity usually need the strongest expertise. Anesthesiology, behavioral health, cardiology, orthopedics, pain management, and multi-specialty physician groups all tend to benefit from billing teams that understand specialty-specific rules rather than generic claim processing.
If your practice needs a billing partner that treats revenue cycle work as an operational discipline instead of a clerical task, Happy Billing is built for that standard. The team combines specialty-specific billing expertise, denial management, A/R recovery, and AI-assisted claim review to help physician groups accelerate cash flow without changing EHRs or adding internal billing overhead.