What Is Revenue Cycle Management? Your 2026 Guide
Revenue cycle management is the end-to-end financial process in healthcare, from patient scheduling to final payment, that makes sure a practice gets paid fully and on time for the care it delivers. In practical terms, it covers everything from registration and insurance verification through coding, claim submission, payment posting, denial work, patient collections, and final account resolution.
If you're a new practice manager, this usually becomes real the moment A/R starts stretching out, EOBs don't match what your team expected, and staff spend more time chasing claims than fixing root causes. A healthy schedule can still produce weak cash flow if front-desk data is wrong, modifiers are missing, or follow-up happens too late. That's why what is revenue cycle management isn't a theoretical question. It's the operating system behind your cash flow.
What Is Revenue Cycle Management in Healthcare
Monday morning starts with a full clinic, but cash is already at risk before the first patient is roomed. The referral for a new orthopedic consult is missing. An anesthesiology case was documented correctly, but the claim will still fail if the wrong direction modifier goes out. Revenue cycle management is the system that prevents those misses from turning into slower cash, avoidable denials, and extra staff work.
Revenue Cycle Management (RCM) is the set of financial and operational controls that gets a practice paid for the care it delivers. It starts before the visit, with scheduling, eligibility, authorization, and estimate accuracy. It ends only when every dollar is posted correctly, appealed if needed, and either collected or written off under policy. HFMA describes revenue cycle work as the process that links the clinical side of care to the financial side of payment and account resolution, in its healthcare revenue cycle overview.
For a practice manager, that definition matters because every handoff affects cash timing. Registration errors create eligibility denials. Weak documentation creates coding edits. Slow charge entry delays claim submission. Poor payment posting hides underpayments. Weak follow-up leaves collectible balances aging until they are much harder to recover.
Specialty details are where many guides get too vague. In orthopedics, CPT 27447 carries a global surgical package, so billing a routine post-op visit outside the allowed rules can trigger a denial or later recoupment. In anesthesiology, modifier selection changes payment logic. A medically directed case billed with QK versus QY, or without the supporting documentation for the number of concurrent cases, can move a claim from payable to rejected. Those are not abstract compliance issues. They affect first-pass yield, staff rework, and days cash sits in A/R.
The practical standard is simple. RCM starts at intake, not after claim submission.
If you want a concise operational breakdown built for independent groups and multispecialty clinics, RCM for physician practices gives a useful practice-level reference.
The End-to-End Revenue Cycle Journey
A new practice manager usually notices the problem at 4:30 p.m. The schedule was full, physicians stayed productive, and cash is still behind because claims are stuck in three different places. One patient was never eligible, another procedure note does not support the modifier billed, and a third claim cleared internally but failed payer edits. That is the revenue cycle in real life. It is a chain of operational decisions that either turns visits into cash or turns staff time into rework.
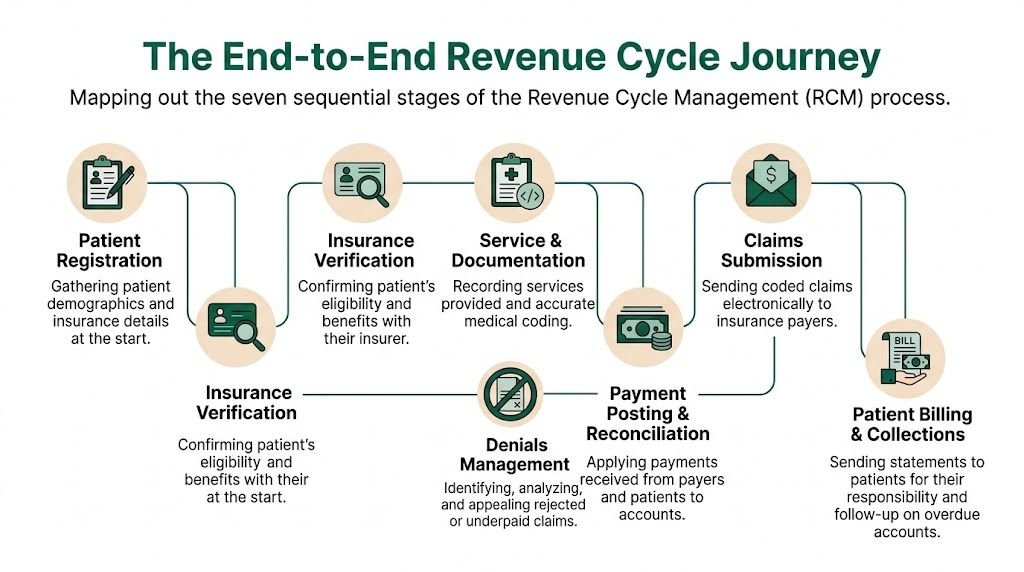
The work runs from scheduling through zero balance, but the highest leakage usually comes from a few predictable points. Front-desk errors create avoidable denials. Incomplete documentation weakens coding. Slow charge entry pushes out submission dates. Weak posting and follow-up hide underpayments. In specialty practices, those misses are rarely generic. They show up in specific code sets, modifiers, authorization rules, and global billing limits.
Pre-visit work decides whether the claim has a chance
The claim effectively starts before the visit.
Scheduling and registration staff need the exact patient identity, current insurance, subscriber details, referral requirements, and authorization status. If any of that is wrong, the rest of the cycle gets more expensive. A rejected claim costs far more to fix after the visit than it does to prevent at intake.
Eligibility checks should happen before the patient is seen, using standard 270/271 transactions where available. The practical goal is simple. Confirm active coverage, benefit category, referral rules, and whether the planned service needs prior authorization. For a pain management case, missing authorization on an injection can stop payment entirely. For behavioral health, the visit may be covered but limited by visit count or plan rules that staff missed at scheduling.
Strong front-end teams focus on three controls:
- exact demographics and member ID entry
- payer-specific referral and authorization requirements
- point-of-service collection for copays, deductibles, and known self-pay balances
A registration error does not stay in registration. It resurfaces in denials, call volume, delayed statements, and extra touches per account.
Documentation and charge capture determine what can be billed
After the encounter, the record has to support the services, diagnoses, timing, and any modifier logic on the claim. At this stage, many practices lose clean claims even though care was delivered correctly.
Orthopedics is a good example. If a provider performs a joint injection and also bills an E/M service, the note has to support a separate, significant evaluation to justify modifier 25. A brief note that only documents the injection decision and performance will not hold up well under payer review. In a post-op setting, teams also have to know whether the service falls inside the global period. Billing routine follow-up outside the global package can create denials or repayment risk later.
Anesthesiology has its own failure points. Modifier selection changes payment logic. A medically directed case billed with QK or QY needs documentation that supports the concurrency and supervision requirements. If the record does not support the modifier, the practice can lose payment even when the case itself was medically necessary.
Good charge capture is operational, not theoretical. Physicians need specialty-specific templates. Coders need fast access to operative reports, time records, implant details, and anesthesia documentation. Edits should fire before the claim goes out, not after the denial comes back.
Coding converts the chart into a payable claim
Coding is where the practice either protects revenue integrity or creates avoidable edits. The job is not just assigning ICD-10-CM, CPT, HCPCS, and modifiers. The job is matching the record to payer rules closely enough that the claim can survive both automated edits and human review.
Specialty billing is where generic RCM advice breaks down:
- Anesthesiology: base units, time units, concurrency, and medical direction modifiers such as AA, QK, and QY
- Orthopedics: global periods, staged versus related procedures, laterality, and multiple-procedure payment reductions
- Cardiology: procedure hierarchies, imaging support, and diagnosis pairing for medical necessity edits
- Behavioral health: authorization tracking, time-based coding thresholds, and payer-specific telehealth requirements
I usually tell new managers to audit denials at the code level, not just by department. "Coding denial" is too vague to fix. "Modifier 25 unsupported on orthopedic injection visits for one payer" is specific enough to retrain providers and stop repeat leakage.
Claim submission is a throughput and edit-management function
Once coding is complete, the claim moves through scrubbing, clearinghouse edits, and payer submission. Speed matters here because every day of charge lag pushes cash out another day or more. Accuracy matters just as much because a fast bad claim still becomes rework.
The highest-value edits usually include:
- NPI, taxonomy, and rendering-versus-billing provider checks
- payer ID and subscriber validation
- authorization number presence and format checks
- diagnosis-to-procedure support edits
- modifier compatibility and bundling edits
Practices get better results when front office, clinical documentation, and billing workflows share the same rules instead of operating as separate teams with separate data. A tighter setup for integrating revenue cycle management across EHR and billing workflows usually reduces handoff errors that never show up until claim submission.
One distinction matters here. A clearinghouse rejection means the payer never received the claim. A payer denial means adjudication happened and the payer found a problem worth refusing or reducing. Those need different work queues, different staff skills, and different turnaround expectations.
Payment posting and follow-up are where practices find the truth
Payment posting looks administrative until you try to manage cash without it. The ERA or EOB shows what the payer did with the claim, including bundling, downcoding, underpayments, contractual adjustments, and denial reason codes. If posting is delayed or inaccurate, managers lose visibility into payer behavior and staff work the wrong accounts.
Denial management should separate issues by root cause. Missing information on a corrected claim is one workflow. Medical necessity appeals are another. Authorization denials belong partly in follow-up and partly in front-end retraining, because the long-term fix sits upstream.
A/R recovery works best when accounts are segmented by age, payer, balance size, denial type, and collectible likelihood. If one payer is slowing anesthesia claims because concurrency documentation is missing, staff should identify that pattern quickly and fix the documentation workflow. If post-op orthopedic visits are being billed during the global period, coders and providers need rule clarification before more claims stack up.
That is the full journey. Every stage affects cash, staff effort, and how often the same account gets touched before it is paid.
Measuring RCM Performance Key KPIs You Cannot Ignore
Monday morning looks busy. The schedule is full, providers are producing, and the bank deposit still misses target. In most practices, that gap shows up in four numbers long before anyone feels it in payroll week.

A useful KPI set does two jobs. It shows whether cash is converting on time, and it points to the exact part of the workflow that is breaking. For a broader operations view, this guide to medical billing KPIs to track is a practical companion.
Days in A R
Formula: Days in A/R = Total A/R ÷ Average Daily Revenue
Days in A/R answers a simple management question. How long does earned revenue sit before it becomes cash? MGMA discusses this metric as a core indicator of billing efficiency and collection speed in physician practices, and their benchmarking resources are widely used for setting practice targets (MGMA on medical practice revenue cycle KPIs).
A high result usually points to one of four operational failures:
- charges are not dropping quickly enough after date of service
- coding review is backing up high-volume encounters
- denied claims are parked instead of appealed or corrected
- payer delay patterns are not separated into dedicated follow-up queues
Specialty detail matters here. If anesthesia claims sit because time units and AA/QK/QX modifier combinations are inconsistent, A/R days rise for a very different reason than an orthopedic practice billing post-op visits inside the global package. The metric is the same. The fix is not.
First-pass clean claim rate
Clean claim rate measures how many claims leave the practice without edits, rejections, or missing data on the first submission. CAQH notes in its index and operating rules work that administrative friction around eligibility, authorization, and claim submission continues to drive avoidable rework across revenue cycle functions (CAQH Index overview).
For a practice manager, this KPI is a process audit disguised as a percentage.
If the rate drops, review claims by payer, CPT family, rendering provider, and modifier pattern. That level of detail usually finds the specific issue faster than broad staff retraining. In anesthesia, one payer may reject claims tied to concurrency documentation and medical direction logic. In orthopedics, the pattern may sit in global surgery edits, assistant surgeon modifiers, or missing implant documentation on high-value cases.
Start with a sample like this:
Payer: Commercial Plan A
CPT range: 01402, 27130, 29881
Modifier review: AA, QK, 24, 25, 57, 80
Edit outcome: front-end rejection vs payer denial
Root cause: auth mismatch, global edit, invalid modifier pairing, missing op note
That is how clean claim rate becomes useful. It stops being a dashboard number and turns into a worklist.
Net collection rate
Net Collection Rate (NCR) is calculated as (payments collected / (charges – contractual adjustments)) x 100 on a date-of-service basis.
HFMA describes net collection rate as one of the clearest measures of how much allowed reimbursement a provider collects after contractual write-offs, making it a direct read on revenue leakage, payer performance, and follow-up discipline (HFMA guidance on key revenue cycle metrics).
This is the KPI I check when leadership says, "Volume is up, so why is cash flat?"
Low NCR often means the practice is doing the hard part. Seeing patients, coding claims, submitting charges, but still losing collectible dollars through underpayments, weak appeals, untimely filing, or bad adjustment posting. It also exposes posting problems. If staff write off balances incorrectly, the practice can make NCR look acceptable on paper while cash trails.
Use date-of-service analysis, not only posted-month reports. Posted-month views can hide whether one payer is consistently underpaying a specific procedure family.
Bad debt rate
Bad Debt Rate is calculated as (Total Bad Debt ÷ Total Service Revenue) × 100.
The Healthcare Financial Management Association has written extensively about rising patient responsibility and the need for earlier financial clearance, accurate estimates, and stronger patient collection workflows because self-pay balances are harder to recover once they age (HFMA on patient financial engagement and collections).
A high bad debt rate usually starts upstream. Eligibility was not verified. Benefits were not explained clearly. The estimate was wrong. No one collected at check-in. Statements went out late. Staff treated patient balances like a back-office issue instead of a front-desk process.
That pattern is expensive in every specialty, but the pressure looks different by service line. Orthopedic cases create larger patient balances tied to surgery, implants, and deductibles. Anesthesia groups often inherit patient dissatisfaction because the anesthesia bill feels separate and unexpected. If managers track bad debt without splitting balances by payer type, service line, and place of service, they miss the operational fix.
These four KPIs matter because each one connects directly to cash, labor, and rework. Track them monthly at minimum. Review them by payer and specialty pattern, not only at the practice total, or the source of leakage stays hidden.
Common RCM Pitfalls and Payer Rules by Specialty
Generic RCM advice breaks down fast when you put it under specialty pressure. Tulane's discussion of revenue cycle variation notes that practices don't all manage the cycle the same way, and that specialty-specific rules such as anesthesiology modifiers, orthopedic global periods, cardiology coding hierarchies, and mental health authorizations significantly alter denial patterns. That's the core issue highlighted in Tulane's overview of specialty-specific RCM complexity.
Here is where practice managers lose money. Not because they don't know billing matters, but because the billing rule is more specific than the workflow they built.
Anesthesiology and the modifier problem
An anesthesiology claim can look complete and still be wrong. The note is signed. Time is documented. The case happened. But the modifier selection controls whether the payer accepts the structure of the claim.
If an anesthesiologist personally performed the case, AA may apply. If the physician medically directed qualifying concurrent cases, modifiers such as QK or QY come into play depending on the scenario and payer rules. If the documentation doesn't support the exact supervision or medical direction standard, the claim can deny or underpay.
The operational fix isn't just coder education. It's building a workflow that checks:
- documented start and stop time
- provider role in the case
- concurrency pattern
- CRNA involvement
- payer-specific anesthesia policy requirements
Orthopedics and the global period trap
Orthopedic RCM gets damaged when teams separate what the payer considers packaged. A common example is CPT 27447 for total knee arthroplasty. Major procedures carry a global period under CMS rules. If the practice bills routine post-op visits separately during that window, the payer may deny them or recoup them later.
Modifier use matters here too. If a later encounter is unrelated and separately billable, the documentation has to clearly support the distinction and the appropriate modifier under the payer's policy. If not, the practice creates avoidable denials and compliance exposure at the same time.
If your orthopedic denials are clustered around postoperative E/M, don't start in collections. Start in surgery scheduling, surgeon documentation, and global-period education.
Cardiology and medical necessity alignment
Cardiology groups often run into denials not because the procedure was inappropriate, but because the claim package doesn't prove why it was appropriate under payer edits. Interventional and imaging services depend heavily on diagnosis selection, documentation support, and code hierarchy logic.
For example, if a diagnostic study is billed without the documentation showing symptoms, findings, or the ordering rationale in a way that aligns with payer policy, the claim may fail medical necessity review. The same is true when multiple cardiovascular procedures occur in one session and the coding hierarchy is handled incorrectly.
Practice managers should audit these claims by payer and CPT family, not just by total denial count. A broad denial bucket hides the underlying issue.
Mental health and authorization-centric leakage
Behavioral health groups often think their biggest risk starts after claim submission. In reality, many denials are born before the patient arrives. Authorization, visit limits, telehealth rules, and payer-specific documentation expectations can all shape collectability.
If the team schedules recurring therapy visits without checking visit counts or auth status, the claim can be dead on arrival even when the clinician's note is strong. For mental health, pre-service and utilization tracking are billing functions just as much as claim submission is.
Specialty-Specific Coding & Payer Pitfalls
| Specialty | Common Pitfall (Incorrect Billing) | The Fix (Correct CPT/Modifier/Rule) | Payer Guideline Source |
|---|---|---|---|
| Anesthesiology | Using the wrong medical direction modifier for the documented staffing pattern | Match the anesthesia claim to documented provider role, time, and concurrency. Review AA, QK, and QY against the operative record and payer rule | CMS anesthesia billing guidance and payer anesthesia policies |
| Orthopedics | Billing routine postoperative E/M outside the surgical package after CPT 27447 | Apply global surgery rules correctly. Bill separate post-op E/M only when documentation supports a truly distinct service under payer policy | CMS global surgery rules |
| Cardiology | Submitting diagnostic or interventional claims without documentation aligned to medical necessity or hierarchy logic | Validate diagnosis support, procedural hierarchy, and modifier use before claim release | CMS coverage guidance and payer cardiology policies |
| Mental health | Failing to secure or track required prior authorization and visit limits | Build pre-service authorization checks into scheduling and intake workflows | Payer behavioral health authorization policies |
If your team is seeing the same denials repeat by specialty, medical billing denial management should focus on rule-specific correction, not generic appeals.
When to Outsource Your Revenue Cycle Management
A practice shouldn't outsource just because billing feels difficult. It should consider outsourcing when internal processes no longer produce predictable cash flow, reliable reporting, or clean accountability.
One reason owners struggle with this decision is that many teams don't measure leakage in a way that separates denials, underbilling, coding gaps, and patient balance fallout. Athenahealth's discussion of healthcare RCM points out that practices can hit a 35-day A/R benchmark and still lose revenue to hidden coding or payer-specific issues, which is exactly why outsourcing decisions often feel unclear until the losses become operationally obvious. That gap is well described in Athenahealth's overview of healthcare revenue cycle management.
Red flags that usually justify a serious review
Some warning signs are easy to spot:
- Staff spend their day firefighting: They chase old claims but can't explain why denials recur.
- Specialty rules outpace internal knowledge: New payer edits, modifier logic, or authorization requirements keep landing after claims fail.
- Turnover keeps resetting the billing team: Every departure takes payer knowledge with it.
- Reports don't separate operational failure types: Leadership sees gross collections, but not whether losses come from coding, underpayments, or front-end registration defects.
Outsourcing also makes sense when providers are growing into more complex service lines. A group that adds pain procedures, advanced imaging, or higher-volume surgery may need deeper coding and denial expertise than a generalist in-house team can provide.
What to look for in a partner
A credible RCM partner should be able to show you how it works the problem, not just promise better collections.
Use this checklist:
- Specialty fluency: Ask how they handle anesthesia modifiers, orthopedic global rules, cardiology hierarchy logic, or behavioral health authorizations.
- Transparent reporting: You need dashboards that isolate claim edits, denials, underpayments, and aging by payer and CPT family.
- Workflow integration: The partner should work inside your current EHR or practice management flow whenever possible.
- Security discipline: PHI handling, role-based access, and HIPAA-first processes aren't optional.
- Defined escalation paths: When a payer stalls, who calls, who appeals, and who updates the root-cause fix?
For practices weighing that shift, outsourced revenue cycle management is worth reviewing with your administrator, physician owner, and billing lead in the same room.
How Technology and Expertise Modernize RCM
At 5:30 p.m., the schedule is closed, charges are in, and the day looks productive. Then the next morning starts with preventable rework. An anesthesia claim held for a missing AA or QK modifier. A postop orthopedic visit billed inside the global period without support for modifier 24. A clean payment posted at face value even though the contract rate was short. None of those failures look dramatic on their own. Together, they slow cash and keep staff stuck in correction mode.
Technology improves RCM when it removes that routine friction before a claim leaves the practice. Expertise improves RCM when payer logic, specialty rules, or documentation judgment decide whether the claim gets paid.
Where automation produces real operational gains
Automation works best on repetitive checks with clear logic. Eligibility verification, demographic validation, NPI mismatches, coverage term dates, duplicate claim detection, and claim-edit scrubbing all belong here. If those checks happen before submission, the billing team spends less time fixing preventable rejects and more time working denials that require analysis.
The strongest systems are configured around specialty-specific rules, not generic billing templates.
For example:
IF specialty = anesthesiology
AND CPT range = 00100-01999
AND modifier NOT IN (AA, QK, QX, QY, AD)
THEN hold claim for review
IF specialty = orthopedics
AND E/M date falls within global period of prior surgery
AND modifier NOT IN (24, 25, 57, 58, 78, 79)
THEN route to coder work queue
Those edits matter because they prevent avoidable touches. Every extra touch adds labor cost, delays submission, and usually pushes payment further out. A fast claim cycle is not just a reporting win. It protects cash flow and reduces the backlog that buries a small billing team by mid-month.
Automation also helps after submission. Good workflow tools sort denials by payer, reason code, CPT family, modifier pattern, and dollar value so staff can work the highest-yield accounts first. That is much better than a flat denial queue where a $45 correction and a $4,500 appeal get the same visibility.
Where human expertise still changes the financial outcome
Software can identify an exception. It usually cannot decide whether the documentation supports payment.
In anesthesiology, a rules engine can catch a missing concurrency modifier. A skilled reviewer still has to reconcile the anesthesia record, confirm time units, and determine whether the documentation supports medical direction rules. If that review is weak, the claim may pay low, deny, or create compliance risk.
In orthopedics, systems can flag visits inside a 10-day or 90-day global period. A coder or auditor still has to read the note and decide whether the service was unrelated, staged, more extensive, or a return to the operating room. Modifier selection is not clerical work in that setting. It directly affects whether the visit is separately payable.
The same pattern shows up in cardiology hierarchy edits, behavioral health authorization failures, and infusion billing where time, drug units, and sequencing all matter. Technology catches what is structured. Experts handle what is clinical, payer-specific, or disputed.
Field advice: Use software to stop repeatable errors at scale. Use experienced coders and denial analysts where judgment protects revenue.
What a modern RCM model looks like in practice
Strong RCM operations use a closed-loop model.
First, the system blocks predictable front-end and coding defects before claim submission. Second, specialized staff handle exceptions, underpayments, appeals, and documentation-based denials. Third, the findings go back to the source of the problem so the same issue does not keep hitting A/R.
That feedback loop is where many practices fall short. If anesthesia claims keep rejecting because the charge ticket does not consistently capture provider direction status, the fix belongs in the anesthesia workflow. If orthopedic postop E/M denials keep rising, the fix may be provider education on global documentation and scheduler prompts tied to recent surgery dates. If payments post below expected reimbursement and nobody compares them to contract terms, the issue is payment variance control, not collections effort.
Modernization is not about buying more software. It is about building a process where automation handles volume, specialists handle judgment, and root-cause fixes reduce repeat work month after month. That is what turns RCM from a billing function into a cash-control system.
Your Next Steps in Mastering Revenue Cycle Management
If you're still asking what is revenue cycle management after reading this, simplify it to one operational truth. RCM is the system that converts clinical work into collectible cash, and every broken handoff inside that system shows up later as delayed payment, write-offs, or staff burnout.
For a practice manager, the next move is usually not a full overhaul on day one. Start with visibility. Pull your aging by payer. Review top denial categories by CPT family and modifier. Spot where front-end errors become backend losses. Then match those findings to specialty-specific rules instead of generic billing advice.
If your group spans several service lines, reviewing the workflows against your exact specialty mix matters more than adopting another generic dashboard. The specialties supported by Happy Billing page is a useful reference for seeing how different specialties require different RCM approaches.
FAQs
| Question | Answer |
|---|---|
| How long does it take to find the main leak in an RCM process? | Usually faster than managers expect if you segment by payer, denial reason, and CPT family instead of reviewing all denials as one bucket. The first goal is not perfection. It's identifying which failure pattern is costing the most cash flow. |
| Should a practice fix front-end or back-end problems first? | Fix whichever issue is creating the highest repeat volume, but most recurring denial problems start upstream. Eligibility, authorization, registration accuracy, and documentation quality often determine whether the backend ever has a realistic chance. |
| Do specialty practices need separate billing workflows? | Yes, in practical terms they do. Anesthesia, orthopedics, cardiology, and mental health all have different coding pressure points, modifier rules, and payer edits. A single generic workflow usually leaves money behind. |
| What should a physician owner ask for in monthly RCM reporting? | Ask for aging by payer, denial trends by category, clean claim performance, net collection view, and a short explanation of root causes. If the report only shows charges and collections, it isn't enough to manage the business. |
How often should you review RCM KPIs
Review core indicators weekly at the operational level and monthly at the leadership level. Weekly review catches fast-moving problems such as rejected claims, authorization misses, or posting delays. Monthly review helps you decide whether the issue is temporary noise or a process flaw.
Which staff roles affect RCM the most
More roles than most owners think. Scheduling, front desk, clinical staff, coders, billers, payment posters, and A/R follow-up all influence collectability. RCM fails when leadership treats it as a billing-office problem only.
What's the first specialty-specific issue to audit
Audit the issue most likely to create repeat denials in your field. In anesthesia, start with modifiers and concurrency documentation. In orthopedics, start with global surgery and postoperative E/M. In mental health, start with authorization tracking. In cardiology, start with medical necessity support and procedural hierarchy review.
Can a practice improve RCM without changing its EHR
Yes. Many improvements come from better workflow discipline, cleaner edits, stronger coding review, and tighter denial feedback loops rather than a full platform change. The key is making sure your current system is being used with specialty-specific rules and clear accountability.
Happy Billing helps physician groups tighten every part of the revenue cycle without forcing an EHR migration. If your practice needs stronger denial control, faster cash flow, or specialty-specific billing support in anesthesiology, mental health, cardiology, orthopedics, or multi-specialty operations, Happy Billing is built for that work.