Knee Arthroscopy CPT Code: The Definitive Billing Guide
Monday morning, an arthroscopy claim that looked clean on Friday is now in denial. The op note supports a meniscectomy and work in a separate compartment, but the payer processed the claim under NCCI logic, bundled the secondary service, and cut payment.
That scenario is common in orthopedic RCM, especially with knee scopes. 29881 and 29877 are familiar codes, but reimbursement usually turns on something else. The claim has to match the payer’s rule set on compartment reporting, laterality, modifier use, and whether a CPT code is payable at all under Medicare edits.
A frequent example is chondroplasty. Commercial plans may consider 29877 based on CPT reporting rules. Medicare often expects G0289 instead when the additional work is in a separate compartment and meets NCCI criteria. Bilateral and multi-procedure cases add another layer. One payer may want -50. Another may require RT/LT on separate lines. A third may reject a distinct procedural service modifier unless the op note clearly separates the compartments and pathology addressed.
In our experience, denied arthroscopy claims usually trace back to one of three points. The code set was technically correct but failed the payer edit. The modifier was right in concept but wrong for that payer’s claim format. Or the operative note described good surgery but not a separately payable service.
The revenue impact is straightforward. A knee scope claim can lose payment on the secondary procedure, trigger multiple procedure reduction, or move into appeal status over an edit the team could have caught before submission. For a busy orthopedic group, those small misses add up fast in both physician and ASC reimbursement.
The working rule is simple. The CPT code identifies the procedure. The rest of the claim has to prove why that work is separately payable, which knee it applies to, which compartment was treated, and which billing logic the payer will enforce.
Practical rule: In knee arthroscopy, payment problems usually come from mismatches between CPT coding, NCCI edits, payer-specific bundling rules, and incomplete operative detail.
Introduction
A denied knee scope claim usually looks minor at first. One modifier is missing, one compartment isn’t documented clearly enough, or the coder followed CPT guidance when the payer was adjudicating under Medicare NCCI logic instead.
That’s why the phrase knee arthroscopy cpt code is misleading if you treat it like a simple code lookup exercise. In orthopedic billing, the code is only the starting point. Real reimbursement depends on laterality, compartment specificity, global period awareness, and whether the payer follows CPT conventions or imposes stricter edit logic.
What practice managers are dealing with right now
The common pain points aren’t theoretical. They show up in daily work:
- Bundled denials: A meniscectomy and chondroplasty are both documented, but the payer treats one as included.
- Modifier confusion: The same bilateral or contralateral case pays differently depending on whether the claim carries -50, -59, X{S}, -RT, or -LT.
- Weak op notes: The surgeon documents tissue removal but doesn’t establish a separately reportable pathology.
- Cash flow drag: Appeals consume staff time while the surgical center and physician payment sit unresolved.
For orthopedic groups, the right response isn’t more generic billing advice. It’s tighter code-level discipline. That means coders who know the difference between 29875, 29876, and 29877. It means scrubbed claims that anticipate NCCI edits before submission. It means operative notes written as both clinical and financial documents.
A strong arthroscopy workflow starts before the claim leaves the practice. It starts in the op note and ends only when the claim logic matches the payer’s logic.
The sections below focus on the denial-heavy situations that matter most: core code selection, modifier use, the CPT versus Medicare bundling conflict, documentation that supports separate payment, and claim scenarios your team is likely seeing every week.
Core Knee Arthroscopy CPT Codes and Descriptions
A common denial starts the same way. The surgeon performs a medial meniscectomy, cleans up cartilage in another compartment, and the claim goes out with every documented service listed as separately payable. The payer applies edit logic, bundles part of the case, and payment drops or the claim pends for review.
That is why base code selection matters. In knee arthroscopy, the first error is often not modifier use. It is choosing the wrong primary CPT code, or adding secondary lines that CPT may describe but the payer will not pay separately.
Common knee arthroscopy CPT codes quick reference
| CPT Code | Description | Critical Billing Tip |
|---|---|---|
| 29870 | Diagnostic arthroscopy, knee | Watch for payer scrutiny when a therapeutic procedure is also performed. |
| 29875 | Surgical synovectomy, limited, single compartment | Use only for a true limited synovectomy. Do not treat it as routine cleanup done during another arthroscopic service. |
| 29876 | Major synovectomy, two or more compartments | Confirm the op note supports work in multiple compartments and describes synovectomy, not general debridement. |
| 29877 | Debridement or shaving of articular cartilage, chondroplasty | Separate-compartment logic may work under CPT, but Medicare often expects G0289 instead. |
| 29880 | Meniscectomy, medial and lateral compartments | Use when both compartments in the same knee undergo meniscectomy. |
| 29881 | Meniscectomy, medial or lateral compartment | Do not bill it twice for the same knee. Bilateral or contralateral cases need claim lines built carefully. |
| 29882 | Meniscus repair, medial or lateral | Distinguish repair from meniscectomy clearly in the operative report. |
| 29883 | Meniscus repair, medial and lateral | Use only when both compartments are repaired, not when one side is repaired and the other side is excised. |
The codes that drive most payment and most edits
For many orthopedic groups, 29880 and 29881 drive the largest share of knee arthroscopy revenue. AAPC explains that 29880 applies when meniscectomy is performed in both the medial and lateral compartments of the same knee, while 29881 applies when the work is limited to one compartment. The same AAPC discussion also notes that chondroplasty is included with these meniscectomy codes in the same or separate compartments, and warns that improper double-billing of 29881 is a common source of orthopedic denials under NCCI edits. See AAPC’s discussion of coding knee arthroscopy with precision.
That inclusion rule has real cash impact. If staff bill 29881 and add 29877 without checking whether the payer treats the cartilage work as bundled, the claim often returns with a denial, reduced payment, or an appeal burden that costs more than the extra line was worth.
High-risk code pairs to review before claim submission
Some code combinations deserve a second look every time:
- 29880 or 29881 + 29877. Review compartment rules and payer bundling policy before reporting both.
- 29881 billed twice on one knee. That usually fails unless the team is dealing with separate knees and the claim clearly shows laterality.
- 29882 or 29883 with meniscectomy codes. Mixed repair and excision cases require close reading of the op note to confirm what happened in each compartment.
- 29875 or 29876 added to another arthroscopy code. Verify that the documented work is a reportable synovectomy and not tissue removal inherent to the primary procedure.
For modifier logic tied to distinct procedural services, use a consistent policy and payer-specific edit review. A practical reference for teams that need to tighten that process is this guide to Modifier 59 and distinct procedural service reporting.
How experienced coders choose the right base code
Start with the service that best represents the main therapeutic work.
If the surgeon performs meniscectomy in one compartment of one knee, 29881 is the starting point. If both the medial and lateral compartments in that same knee undergo meniscectomy, 29880 is the better code. If the case is a repair rather than an excision, move to 29882 or 29883 based on whether one or both compartments were repaired.
Then test every additional arthroscopy line against two questions. Is it separately reportable under CPT and NCCI? Will this payer pay it as billed, or does the plan apply stricter bundling logic than CPT describes?
That second question is where practices lose money. A coder can be technically correct under CPT and still send out a claim that a Medicare contractor or commercial payer will bundle on first pass.
The clean claim is usually the one that matches the operative note, the edit file, and the payer’s reimbursement rule on the first submission.
Practice managers should audit this section of the workflow closely. Knee arthroscopy revenue does not usually leak because teams lack a code list. It leaks because multi-procedure cases, same-knee compartment logic, and payer edit rules are not reconciled before the claim drops.
Applying Key Modifiers to Knee Arthroscopy Claims
Modifiers are where orthopedic arthroscopy claims are won or lost. The CPT code states the service. The modifier explains the circumstances that affect payment.
Laterality comes first
In knee arthroscopy, -RT and -LT aren’t optional details. They are core claim identifiers. If a claim involves one knee, laterality should align across the CPT line, diagnosis coding, and operative documentation.
This matters even more when the same code appears more than once in a session. A payer may reject a claim that looks like duplicate billing if the line items don’t clearly show separate knees.
Use laterality to answer the simplest payer question first: which knee was treated?
Distinct service logic matters more than most teams think
The harder modifier decision is usually -59 versus one of the X{EPSU} modifiers. In arthroscopy, coders often reach for -59 because it’s familiar. That can work, but many payers scrutinize it heavily because it is broad.
When the situation is about a separate anatomical structure, X{S} often tells the story more precisely than -59. If your team needs a refresher on how payers evaluate distinct procedural service logic, this guide to modifier 59 in medical billing is worth keeping in your coding library.
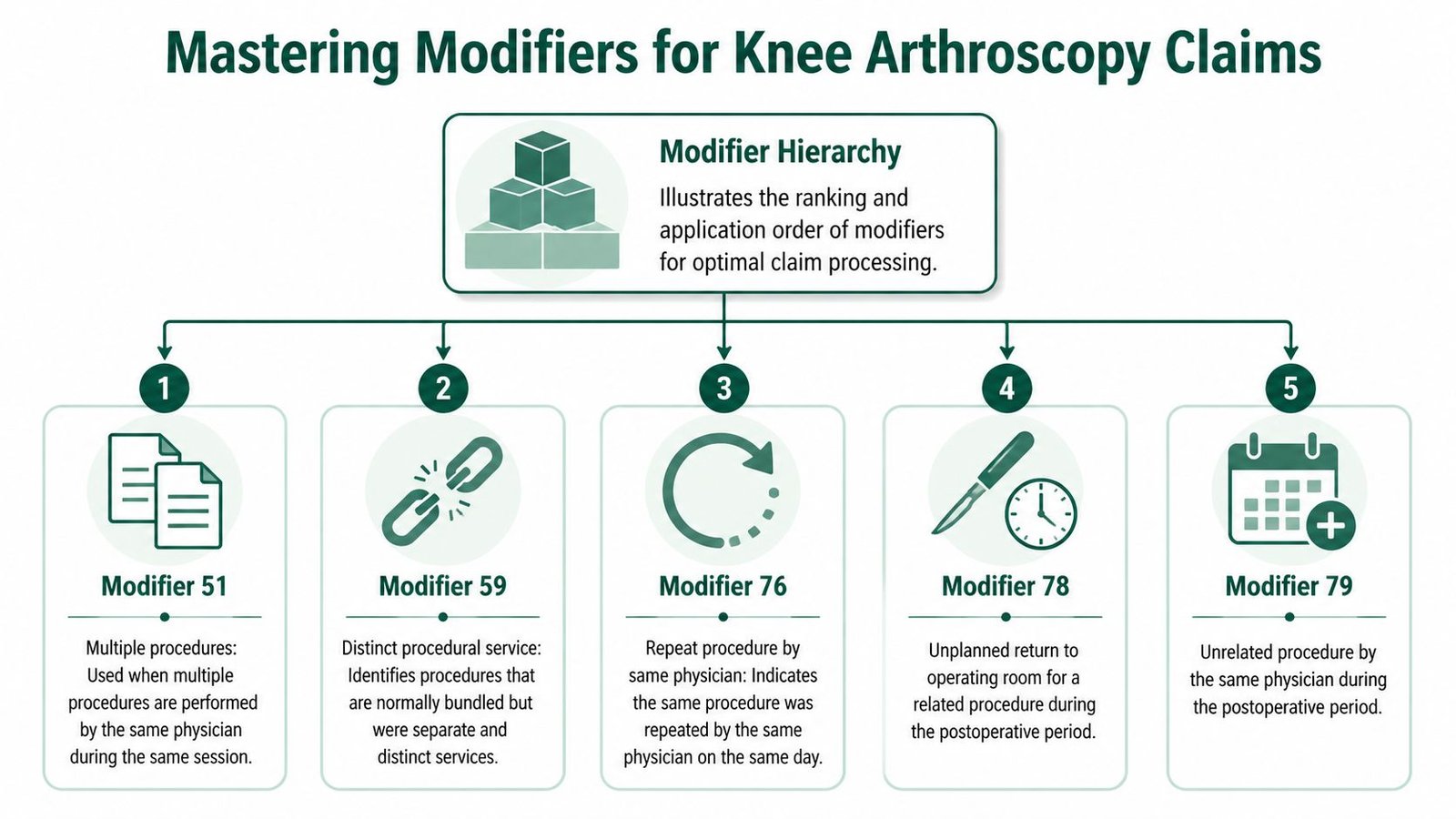
A practical hierarchy helps:
- Use -RT/-LT to establish side.
- Use -50 when the payer accepts bilateral submission that way.
- Use -59 or X{S} only when you must establish a distinct service that edits would otherwise bundle.
- Use -51 only where payer processing expects multiple procedure logic rather than automatic ranking.
- Use postoperative modifiers like -78 or -79 only when you are inside the global period and the later procedure meets the modifier definition.
Modifier choices by scenario
| Scenario | Modifier issue | Operational note |
|---|---|---|
| One knee, one procedure | Laterality | Use -RT or -LT consistently. |
| Same session, both knees | Bilateral vs contralateral | Check whether payer wants -50, separate lines with RT/LT, or both. |
| Bundled service in a separate structure | Distinct procedural service | Consider -59 or X{S} based on payer preference. |
| Repeat same-day procedure by same physician | Repeat logic | -76 applies only when the same procedure is repeated by the same physician on the same date. |
| Return to OR in postop period | Global modifier | Distinguish -78 for related return from -79 for unrelated surgery. |
What doesn’t work
Three habits create avoidable denials:
- Defaulting to -59 on every edit. That looks like unbundling rather than compliant coding.
- Using -50 without checking payer formatting. Some carriers want one line; others want two lines with side modifiers.
- Ignoring the global period. A technically correct CPT code can still deny if the claim lacks the modifier that explains why it’s payable during postop recovery.
Operational advice: Build payer-specific arthroscopy rules into your scrubber or cheat sheet. The modifier that works for one commercial payer may fail under Medicare or another carrier’s claim logic.
For practice managers, the fix is process, not heroics. Require coders to make a documented modifier choice based on payer rule, not habit. If the team can’t explain why -59, X{S}, -50, or RT/LT was chosen, the claim isn’t ready.
Navigating NCCI Edits and Payer-Specific Bundling Rules
The most expensive mistake in knee arthroscopy billing is assuming that CPT guidance alone controls payment. It doesn’t. Medicare adjudicates against NCCI edits, and those edits can override what a coder expects from the CPT book.

The 29877 versus G0289 conflict
This is the denial pattern orthopedic teams keep seeing. Under CPT guidance, 29877 may be reported with another knee arthroscopy procedure when the chondroplasty occurs in a separate compartment. That sounds straightforward.
Medicare often doesn’t process it that way. According to AAPC’s discussion of arthroscopy coding and the 29877 edit conflict, Medicare’s NCCI edits often require HCPCS G0289 instead when chondroplasty or loose body removal is bundled with another arthroscopic knee procedure. AAPC also notes that this edit has a "0" modifier indicator in NCCI Chapter IV, which blocks override logic, and ties the discrepancy to up to a 30% denial rate on multi-procedure arthroscopies.
That means a coder can follow CPT logic and still submit a claim Medicare will reject.
The dual-strategy approach that actually works
You need two coding pathways, not one universal rule:
- Commercial payer pathway: Review policy and contract behavior. Some payers follow CPT compartment logic more closely.
- Medicare pathway: Assume NCCI edit logic controls. If the scenario fits the Medicare rule set, evaluate whether G0289 is the correct reporting option instead of 29877.
That distinction should sit inside your pre-bill review process. If your team only asks, “Was chondroplasty done in a separate compartment?” it’s missing the more important question: “How will this payer adjudicate it?”
For practices that also struggle with postop packaging and related surgery edits, this resource on orthopedic billing global periods fits the same operational problem. Payment depends on payer edit logic, not just the procedure list.
Where revenue leakage actually happens
The leak usually appears in one of these places:
- The coder reports 29877 to Medicare because the op note says “separate compartment.”
- The claim edits out under NCCI because Medicare expected G0289 logic.
- Staff appeal using CPT language only, which doesn’t solve a Medicare NCCI denial.
- A/R ages while the case gets reworked.
If the payer’s edit system and your coding system are using different rulebooks, the claim will lose every time.
The corrective action is not more aggressive modifier use. It is payer-specific claim design. Arthroscopy claims should be scrubbed against payer type before they’re released, especially when chondroplasty, loose body removal, or another secondary arthroscopic service appears on the same operative report.
Documentation Requirements for Bulletproof Operative Notes
A denied knee arthroscopy claim often starts in the OR, not in billing. The surgeon performs the right work, the coder chooses the right code family, and the payer still rejects the secondary line because the operative note reads like routine cleanup instead of a distinct service.
For orthopedic practices, that is where margin slips. Multi-procedure arthroscopy claims are paid or denied on small documentation details: compartment, pathology, laterality, and whether the surgeon clearly separated billable work from work the payer views as included.
What payers need to see for 29875
This section is the right place to get specific about 29875. If your article’s code summary listed the code earlier, keep that explanation short there and let the documentation standard live here.
For 29875, the operative note has to support a limited synovectomy in a separate compartment with documented synovial pathology. A generic statement such as “debrided synovitis” or “cleaned up inflamed tissue” is usually not enough to defend payment, especially when the case also includes meniscectomy, chondroplasty, or another arthroscopic service subject to bundling review.
The note should identify:
- Which compartment was treated: medial, lateral, or patellofemoral
- What pathology was present: inflamed synovium, hypertrophic synovium, or other abnormal synovial findings
- Why the work was medically necessary rather than incidental to the primary arthroscopic procedure
- What the surgeon did to address that pathology
That last point matters. Payers deny many secondary arthroscopy lines because the op note describes tissue removal as access work, visualization work, or routine debridement performed during the main procedure. Once the note sounds incidental, appeals get much harder.
Weak note versus defensible note
Weak documentation usually reads like an afterthought: synovial tissue was removed during arthroscopy. That wording gives the coder almost nothing to work with. It does not identify the compartment, the abnormal finding, or the reason the service should stand on its own.
A defensible note is more precise. It ties the pathology to a location and makes the separate work visible on the page.
Use this standard with surgeons:
- Name the compartment
- Describe the abnormal tissue
- State the treatment performed
- Differentiate separate pathology treatment from routine cleanup
- Keep laterality consistent throughout the report
If the note cannot answer those five points, the claim is exposed.
Documentation points that prevent high-denial arthroscopy edits
The operative report should do more than support the CPT code. It should also survive NCCI and payer edit scrutiny when multiple services appear on the same claim.
That means the note should clearly show:
- Primary procedure first, with the main diagnosis or pathology tied to it
- Secondary arthroscopic work as a distinct service, not a vague extension of the primary procedure
- Separate compartments when applicable, because many edit disputes turn on location
- Bilateral or contralateral details, including which knee and which procedure was done on each side
- Medical necessity for each billed line, especially when one service is commonly bundled into another
Orthopedic groups lose time in A/R. The coding team may know a line is reportable under CPT logic, but if the note does not spell out the separate pathology and location, the payer has an easy denial rationale. Then staff appeal with a better argument than the original note can support.
A practical operative note checklist
Use a surgeon-facing checklist before final signature:
- Laterality is documented in the header, body, and procedure list
- Each arthroscopic procedure is tied to a specific finding
- Each finding is tied to a specific compartment when relevant
- Separate procedures are described in separate sentences or paragraphs
- The report distinguishes treatment of pathology from routine shaving, irrigation, or visualization
- Bilateral cases identify what was done on the right knee and left knee independently
- Implants, repairs, and removals match the procedure list and billing ticket
Template design helps here. Free-text notes create avoidable ambiguity. A structured arthroscopy template with required fields for compartment, pathology, laterality, and distinct procedure descriptions usually cuts coder queries and appeal volume.
If your physicians also struggle with separating services in office or perioperative documentation, the same discipline applies to E/M support. This overview of documentation standards for CPT modifier 25 is useful for reinforcing that separate payment requires separate note support.
Documentation habits that reduce rework
Start with denied claims, not abstract education. Review the last ten denied or downcoded knee arthroscopy cases and compare the operative notes against the payer rationale. That gives surgeons a concrete view of what language cost the practice money.
Then hardwire the fixes into workflow. Add required fields in the op note template. Build coder queries for missing compartment detail. Stop claims with conflicting laterality before they leave the office.
Coder retraining helps. Surgeon documentation changes usually produce the faster financial return because they address the root cause of the denial instead of cleaning it up after adjudication.
Real-World Coding Examples and Claim Scenarios
Monday morning. The surgeon finished three knee scopes on Friday, the claims went out, and by Tuesday one is sitting in edits because the coder followed CPT logic while the payer applied NCCI logic. Another is pending because the bilateral format did not match the carrier’s preference. These are the cases that drain margin in an orthopedic practice. The problem is rarely the primary code. The problem is how the claim is built when multiple procedures, both knees, or payer-specific bundling rules collide.
Scenario one meniscectomy with additional cartilage work
The surgeon performs 29881 for a meniscectomy in one compartment of the right knee. The operative note also documents chondroplasty in a different compartment.
This is a common trap. A coder sees separate compartment work and wants to add a second arthroscopy line. That may be right under one payer’s policy and wrong under another. The financial risk is straightforward. Overbill it and the claim denies or gets recouped later. Underbill it and the practice gives up revenue that was supported by the note.
Use a decision sequence that starts with the payer, not the code book:
- Report 29881-RT as the primary service when the documentation supports meniscectomy.
- Confirm the cartilage work was therapeutic and performed in a different compartment, not routine shaving tied to the meniscectomy.
- Check the payer’s arthroscopy bundling policy before adding any secondary code.
- Apply a distinct service modifier only when that payer requires it and the op note clearly supports separate reporting.
The error pattern I see most often is automatic use of -59 on every chondroplasty line. That invites manual review. It also weakens appeals because the claim looks modifier-driven instead of documentation-driven.
Scenario two contralateral diagnostic arthroscopy and meniscectomy
One knee gets a meniscectomy. The opposite knee gets a diagnostic arthroscopy during the same session. Clinically, the case is easy to understand. On the claim, it can fail for formatting, modifier selection, or both.
Guidance summarized in this discussion of diagnostic arthroscopy and meniscectomy billing notes that CPT allows 29881 on one knee and 29870 on the contralateral knee with -59 or X{S} modifiers, but payer rules diverge. The same source links that modifier inconsistency to a 25% first-pass rejection rate on multi-knee cases and notes that CMS multiple-procedure payment reduction can cut the secondary procedure by 50%.
That matters because this denial often has nothing to do with medical necessity. It is a claim construction problem.
| Service | Likely line construction | Key review point |
|---|---|---|
| Meniscectomy on one knee | 29881-RT or 29881-LT | Match the operative side exactly |
| Diagnostic arthroscopy on opposite knee | 29870-LT or 29870-RT, with payer-dependent distinct modifier logic | Confirm whether the payer wants laterality only or laterality plus -59/X{S} |
Appeals on these cases need procedure-specific logic. A generic reconsideration letter usually fails because it does not address the exact code pair, laterality setup, and payer edit that caused the rejection. Teams that see repeated arthroscopy denials should tighten their medical billing denial management workflow around code-pair analysis and payer-specific appeal templates.
In multi-knee arthroscopy, coding accuracy and claim formatting both determine payment.
Scenario three bilateral arthroscopy in the same session
Now take a bilateral case where similar arthroscopic procedures are performed on both knees in one operative encounter. The coding issue is not only what was done. The issue is how that payer wants bilateral work reported.
Some carriers want modifier 50 on a single line. Others want two lines with RT and LT. Some adjudication systems can process either format, but one format pays correctly while the other suspends or underpays. Using one bilateral method across all payers is one of the fastest ways to create avoidable rework.
For bilateral arthroscopy claims, the billing team should verify four points before submission:
- the payer’s required bilateral submission format
- the exact procedure performed on each knee
- whether multiple-procedure reduction will affect one of the lines
- whether the remittance paid both knees correctly after adjudication
Underpayments are easy to miss here. The claim may not deny, but the second side may process at the wrong rate or bundle incorrectly. Practices that monitor only denials miss that leakage.
Strong orthopedic RCM performance comes from handling these cases at the edit level before the claim leaves the office. That is where multi-procedure, bilateral, and CPT-versus-NCCI conflicts get resolved before they turn into aging AR.
Conclusion Building a Proactive Orthopedic Coding Workflow
A reliable knee arthroscopy cpt code workflow has four parts. First, choose the correct base procedure code. Second, apply modifiers based on payer logic rather than coder habit. Third, check every multi-procedure case against NCCI and commercial bundling rules before submission. Fourth, make sure the operative note supports the billing theory line by line.
Most practices don’t need more code lists. They need a tighter operating system around arthroscopy claims. That means auditing denials by code pair, teaching surgeons exactly what compartment-level detail supports payment, and requiring a pre-submission review for cases involving chondroplasty, synovectomy, contralateral scopes, or bilateral work.
A workable implementation plan is straightforward:
- Audit recent denials: Group them by code pair and modifier pattern.
- Standardize surgeon templates: Force laterality, compartment, and pathology into the note.
- Create a payer matrix: Separate Medicare arthroscopy logic from commercial arthroscopy logic.
- Use a pre-bill checklist: Stop claims with unresolved bundling questions before they leave the practice.
For orthopedic practices looking to eliminate denial-related revenue leakage and streamline their billing, learn more about orthopedic revenue cycle management strategies and explore specialized support through Happy Billing’s orthopedic billing services.
Knee Arthroscopy Coding FAQs
Can 29881 and 29877 be billed together
Sometimes, but not automatically. CPT guidance may allow separate reporting when chondroplasty is performed in a separate compartment. Medicare often applies different logic through NCCI edits and may require G0289 instead of 29877. The operative note must clearly support distinct work, and the final code choice should be payer-specific.
What is the main documentation requirement for 29875
The note must identify a specific knee compartment and document a true synovial pathology that justifies limited synovectomy. A statement that the surgeon removed loose or incidental tissue is usually not enough to support 29875.
Should bilateral knee arthroscopy be billed with modifier 50 or with RT and LT
It depends on the payer. Some carriers accept modifier 50, while others want separate line items with -RT and -LT. The safest process is to maintain a payer-specific bilateral arthroscopy matrix rather than using one submission style for every claim.
When should 59 or X{S} be used on knee arthroscopy claims
Use them only when you need to show that a service ordinarily bundled under edits was in fact distinct. In knee claims, that often relates to separate structures or contralateral procedures. If laterality alone explains the claim, don’t add -59 just because an edit exists.
If your orthopedic team is tired of losing time to knee arthroscopy denials, Happy Billing helps practices tighten coding workflows, reduce rework, and improve payment velocity with specialty-specific RCM support built for high-edit procedural claims.