RCM Denial Management: A Physician’s Guide to Recovery
RCM denial management is the process of systematically preventing, analyzing, and appealing denied claims to recover revenue that your practice already earned. It matters because the average practice sees roughly 1 in 5 claims denied on the first pass, with one industry source reporting an average initial denial rate of 16 to 20% across all payers.
If you're a physician owner or practice administrator, that number should change how you look at billing. Denials aren't a back-office nuisance. They are a direct threat to cash flow, staffing efficiency, and days in A/R. We've seen strong practices lose momentum not because demand was weak, but because preventable denials kept turning clean clinical work into delayed or forfeited collections.
The practices that handle RCM denial management well don't treat denials as isolated events. They run denial prevention on the front end, denial analysis in the middle, and disciplined recovery on the back end. That is what protects margin in specialties where a single authorization miss, modifier error, or documentation gap can tie up revenue for weeks.
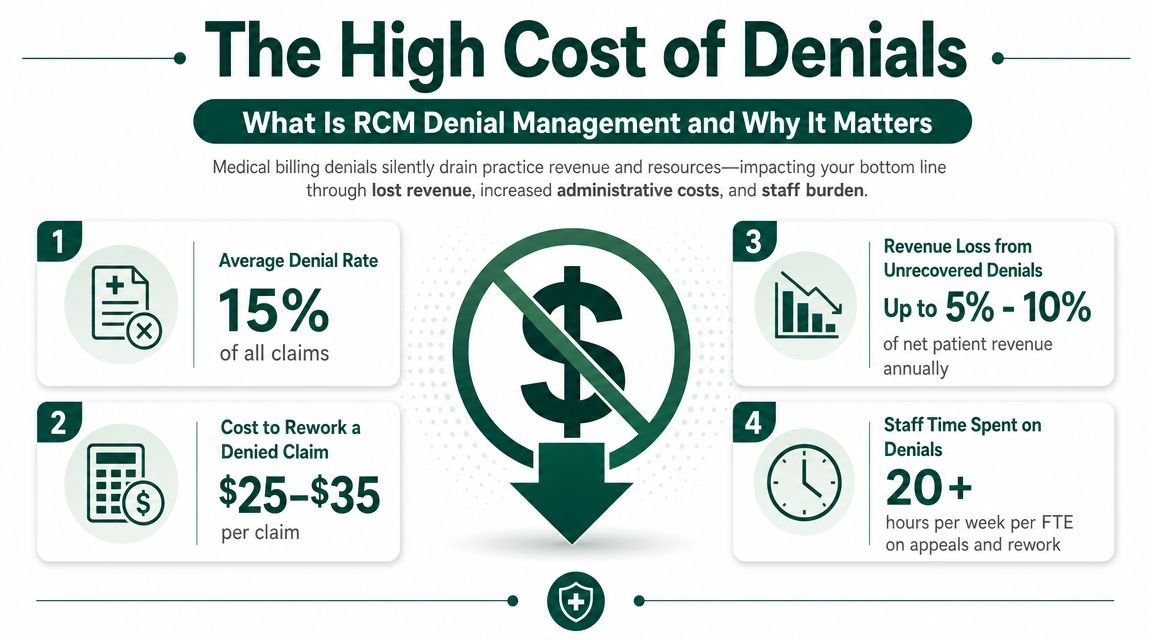
What Is RCM Denial Management and Why It Matters
About 1 in 5 claims gets denied on first pass, with one industry benchmark putting the average initial denial rate at 16 to 20% across payers (industry benchmark on first-pass denials). KFF also reported that insurers on HealthCare.gov denied about 17% of in-network claims in 2021 (KFF analysis of claim denial rates). For practice owners, that is not a billing-side annoyance. It is a margin problem.
RCM denial management is the work of finding out why claims were denied, correcting claims that can be fixed, appealing underpaid or wrongly denied claims, and changing front-end and mid-cycle processes so the same revenue does not get trapped again. The best teams treat it as a financial control system across the revenue cycle, not a stack of follow-up tasks.
Why owners should care first about cash
Denials hit cash flow before they show up on a dashboard.
A cardiology group can perform a medically appropriate echo or stress test and still wait weeks for payment because authorization rules were missed or documentation did not support medical necessity tightly enough. An anesthesia group can lose yield on high case volume if modifiers, time units, or concurrency details are off by just enough to trigger rework. An orthopedic practice can have a profitable surgical schedule on paper while implants, global package edits, and post-op coding disputes slow collections and push dollars into aging buckets.
The operational pattern is predictable:
- Cash collection slows: claims that should have paid in the first cycle move into correction, rebilling, or appeal.
- Labor cost rises: experienced billing staff spend time recovering old revenue instead of protecting current claims.
- A/R quality drops: reported production looks healthy while collectible cash lags behind actual clinical output.
Practical rule: If volume is steady, physicians are busy, and cash still swings month to month, denial performance deserves an immediate audit.
Many revenue cycle teams use under 5% as a strong target for denial rate performance (HFMA guidance on denial rate benchmarks). If a practice is sitting far above that mark, the answer is rarely to hire one more collector. The answer is to find which failure points are producing the most preventable write-offs and rework.
Denial management affects the whole revenue cycle
Denied claims usually start upstream. Registration errors, missed prior auth, coding edits, missing op notes, weak medical necessity support, and payer filing issues all show up later as denied dollars. Owners who want cleaner cash need visibility across scheduling, eligibility, authorizations, documentation, coding, charge entry, and claim submission.
Documentation is often where specialty economics get real. In cardiology, vague indications can weaken support for diagnostic testing. In anesthesia, incomplete records can create payment disputes tied to time and medical direction. In orthopedics, implant-heavy and surgery-heavy cases carry enough reimbursement that one documentation gap can wipe out the margin on a case after staff rework is counted. Teams that want to tighten this area can review expert methods for improvement.
For owners who need a quick refresher before changing process, this overview of how RCM works in medical billing gives the right baseline.
Decoding Denials Common Root Causes and Categories
The fastest way to lose control of denial work is to treat all denials as one pile. The practices that recover cash consistently separate denials by root cause, then fix the upstream failure. A useful operational model is to review EOB and ERA remittance codes, categorize denials by cause such as eligibility, coding, authorization, and documentation, then trend the recurring problems so the team can focus on high-dollar and repeat issues (data-driven denial categorization workflow).
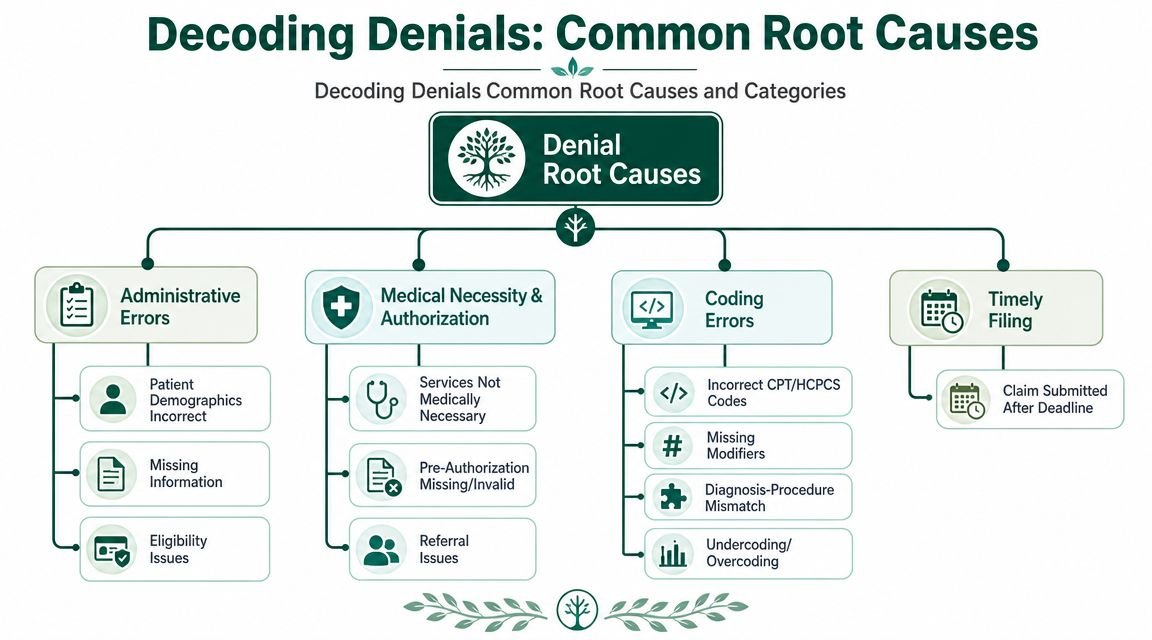
Front-end failures
A surprising share of denials begins before the patient is seen.
- Eligibility issues: Coverage wasn't active, the plan changed, or the wrong payer order was used.
- Registration mistakes: Name, DOB, subscriber ID, or group details don't match what the payer has on file.
- Referral gaps: The service may be appropriate, but the administrative prerequisite wasn't met.
In cardiology, this can surface on something as routine as CPT 93306. If the payer record, referral requirement, or plan rules weren't verified before the echocardiogram, the practice doesn't just get a denial. It gets a delay on a service that already consumed physician time, room time, and equipment capacity.
Clinical and authorization denials
These are expensive because they often involve services with higher reimbursement and more documentation.
A common example is a procedure that required prior authorization but was performed without valid approval on file. In physician-owned groups, this is usually not a billing error alone. It's a handoff failure between scheduling, clinical staff, and whoever owns payer requirements.
A denial for missing authorization is rarely a one-claim problem. It usually means your process is producing more of the same claim right now.
For practice leadership, the point isn't just compliance. It's financial sequencing. If the scheduler doesn't know payer rules and the physician assumes approval was handled, revenue gets put at risk before the encounter even happens.
Back-end coding and billing denials
These are the denials owners tend to recognize because they look technical. They still have a business consequence.
In orthopedics, modifier misuse on a procedure in a global period can trigger a denial even when the service was legitimate. In anesthesia, the wrong anesthesia modifier can change how the payer interprets the claim entirely. A coding error isn't just a coding error when it delays or reduces payment on high-value work.
Here is a practical breakdown:
| Category | Common example | What the owner loses |
|---|---|---|
| Eligibility | Coverage not verified before visit | Delayed payment and avoidable follow-up |
| Authorization | Pre-cert missing for scheduled procedure | Higher-value claim held or denied |
| Coding | Missing modifier or diagnosis mismatch | Rework, rebills, and payer scrutiny |
| Timely filing | Claim submitted after payer window | Revenue may become unrecoverable |
If you want a clearer operating view of recurring payer patterns, this guide on the top denial categories in medical billing pairs well with dashboard work. For leaders building better oversight, using operational analytics well means unlocking real-time ROI with data, not just generating more reports.
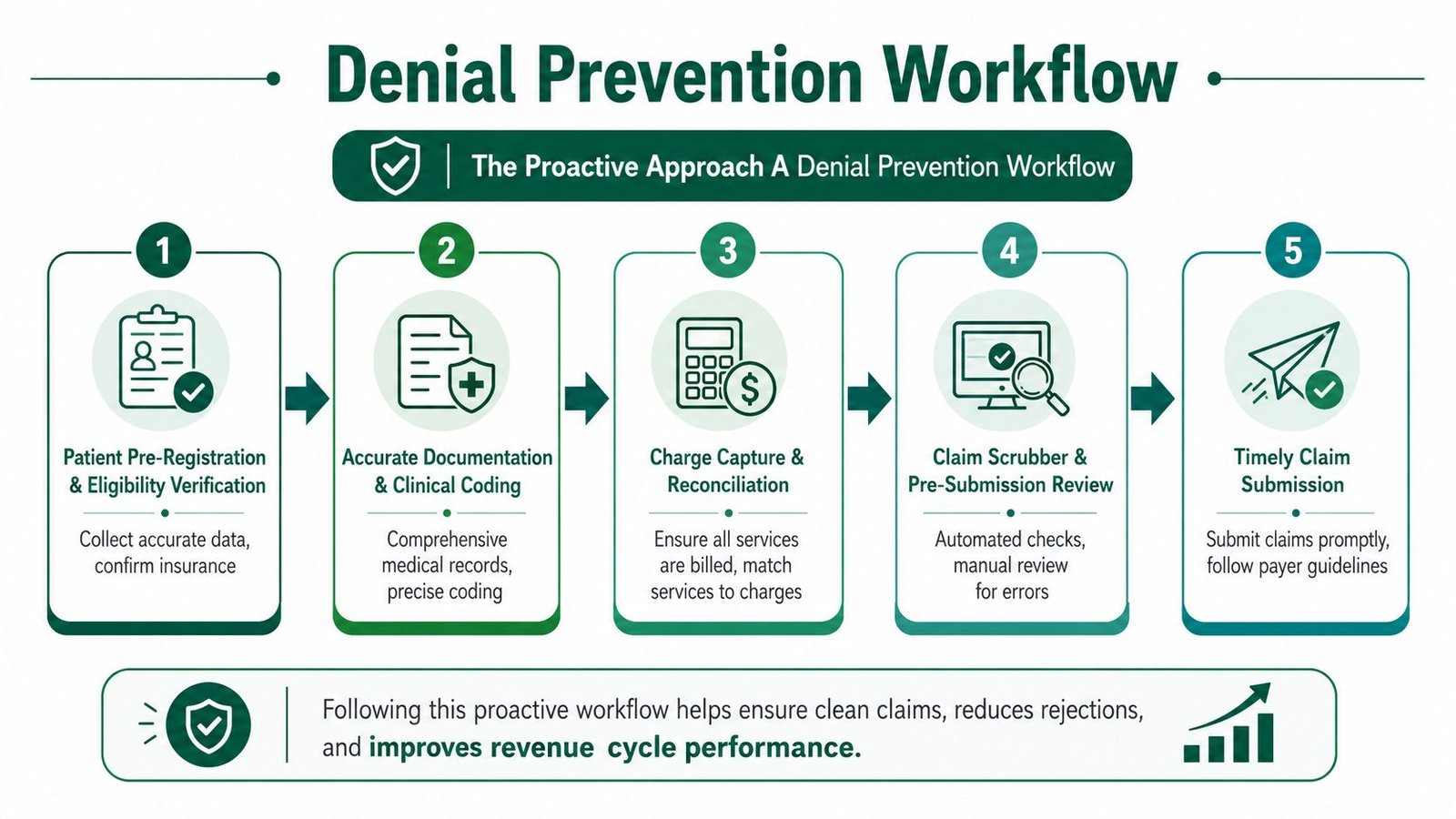
The Proactive Approach A Denial Prevention Workflow
Practices that keep denials under control usually prevent them long before a payer ever touches the claim. High-performing revenue cycle teams generally treat a low single-digit denial rate as the operating target, because every avoidable denial adds labor cost, slows cash, and increases write-off risk.
For owners, the financial question is simple. Which controls stop preventable denials on your highest-value services before staff time gets burned on rework?
Required checkpoint one
Before the visit, the practice needs a clean demographic record, active coverage, correct payer order, and a verified answer on referral or authorization requirements. Small front-end errors create expensive downstream denials.
The impact varies by specialty. In cardiology, a missed authorization on advanced imaging or diagnostic testing can delay payment on a meaningful ticket. In orthopedics, a surgery posted to the wrong plan can tie up a large claim balance for weeks. In anesthesia, a registration error can affect multiple linked charges from the same case and turn one mistake into several denials.
Required checkpoint two
Documentation and coding must support the service exactly as billed. Notes need to show medical necessity and the work performed. Coding has to align CPT, ICD-10-CM, HCPCS, units, and modifiers with both the record and the payer's edits.
Specialty economics hold particular significance.
- Cardiology: Testing and procedure claims often stand or fall on diagnosis support and payer coverage rules. If the note does not clearly support why the study was ordered, payment can stall on a service line that materially affects monthly collections.
- Orthopedics: Modifier 25, 57, 59, and global-period logic can change whether the practice gets paid correctly or invites a denial that takes repeated follow-up to unwind.
- Anesthesia: Time, concurrency, provider role, and modifiers such as QK, QX, AA, or QZ are payment drivers. A wrong modifier is not a minor error. It changes how the payer prices the claim.
Required checkpoint three
Claims need a pre-submission review that combines edits software with experienced human review. Scrubbers catch missing fields and common payer edits. They do not catch every documentation gap, specialty-specific modifier issue, or local payer habit.
A flagged claim before submission is still cheap to fix. A denied claim after submission is already costing money.
A practical prevention workflow usually includes:
- Pre-registration review: Confirm patient identity, insurance details, financial class, and payer order.
- Eligibility verification: Recheck active coverage close to the date of service, especially for procedures and hospital-based work.
- Authorization tracking: Record what is required, approved, pending, or expired, and tie it to the scheduled service.
- Coding reconciliation: Match charges to the note, operative report, imaging order, or anesthesia record before release.
- Claim scrub and hold logic: Stop claims with modifier conflicts, diagnosis mismatches, missing units, or payer-specific edit failures.
- Daily denial feedback: Send denial trends back to registration, clinicians, surgery scheduling, and coding so the same error does not repeat next week.
In audits, the biggest gap is usually not effort. It is ownership. If nobody owns auth accuracy for ortho procedures, diagnosis support for cardiology testing, or anesthesia modifier review before release, denials keep recurring because the process has no control point.
A focused process review can usually show where that leakage starts. This guide on how to reduce claim denials is a useful reference if you need to tighten front-end controls and set clearer accountability.
The Reactive Strategy An Efficient Denial Recovery Process
Even well-run practices still get denials. The difference is what they do next. Weak teams work denials in the order they appear. Strong teams work them in the order that protects cash.
HFMA recommends segmenting denial data by insurer, denial reason, and service location, which points to a broader truth. Effective denial recovery needs a portfolio mindset that ranks denials by likely recoverability, payer behavior, filing deadlines, and net margin impact (HFMA guidance on denial prioritization).
First-in first-out is the wrong model
A FIFO queue feels fair. It is usually financially inefficient.
If one denial is easy to correct but low value, and another is harder but approaching a filing deadline with stronger recovery potential, the second claim should often go first. Practice owners don't need more activity. They need better sequencing of activity.
A useful triage framework looks like this:
- Work now: High-value claims, short filing windows, favorable payer history
- Batch and correct: Routine registration or coding edits with clear fixes
- Escalate clinically: Medical necessity denials that need physician input or records support
- Write off quickly when appropriate: Claims with no practical recovery path, so staff time stays focused on collectible revenue
Correction versus appeal
Not every denial should go through a full appeal.
Some denials only need a corrected claim. Examples include a missing modifier, a typo in subscriber information, or a claim frequency code issue. These should move fast because they tie up revenue without adding strategic value.
Other denials require a formal appeal packet. Those usually involve medical necessity, authorization disputes, or payer interpretation of documentation. In those cases, the practice needs exact payer logic, complete records, and a response that addresses the denial reason directly.
The biggest recovery mistake we see is using appeal labor on claims that only need correction, while true appeal claims sit too long.
Build a denial worklist around money, not emotion
Owners often ask how to tell whether their billing team is doing denial follow-up well. Start with the worklist itself. If the team can't show which denials are being prioritized by payer, denial category, deadline pressure, and financial impact, then the process is still operationally busy but strategically weak.
For independent groups, this matters even more in specialty care:
- Cardiology: A medically necessary study may deserve escalation because the documentation case is strong.
- Anesthesia: A modifier-based denial may be recoverable quickly if the claim role and medical direction details are corrected.
- Orthopedics: Post-op and global-period disputes may need deeper review before deciding whether to appeal or rebill.
If your team needs a cleaner framework for response sequencing, this guide on how to appeal a denied insurance claim is useful as an operational reference. But the bigger owner-level point is simple. Denial recovery should be managed like an investment portfolio, not an inbox.
Technology and Staffing The Right Mix for Your Practice
Most physician groups don't fail at denial management because they don't care. They fail because the staffing model and toolset don't match the complexity of the work. The right answer depends on denial volume, specialty mix, physician documentation quality, and whether your current team can prevent denials before they happen.
A practical benchmark is to keep the denial rate under 5%, and guidance also emphasizes that automation and AI are most valuable when they identify likely-denied claims before submission, because delay can push claims beyond payer resubmission or appeal windows (automation and pre-submission flagging guidance).
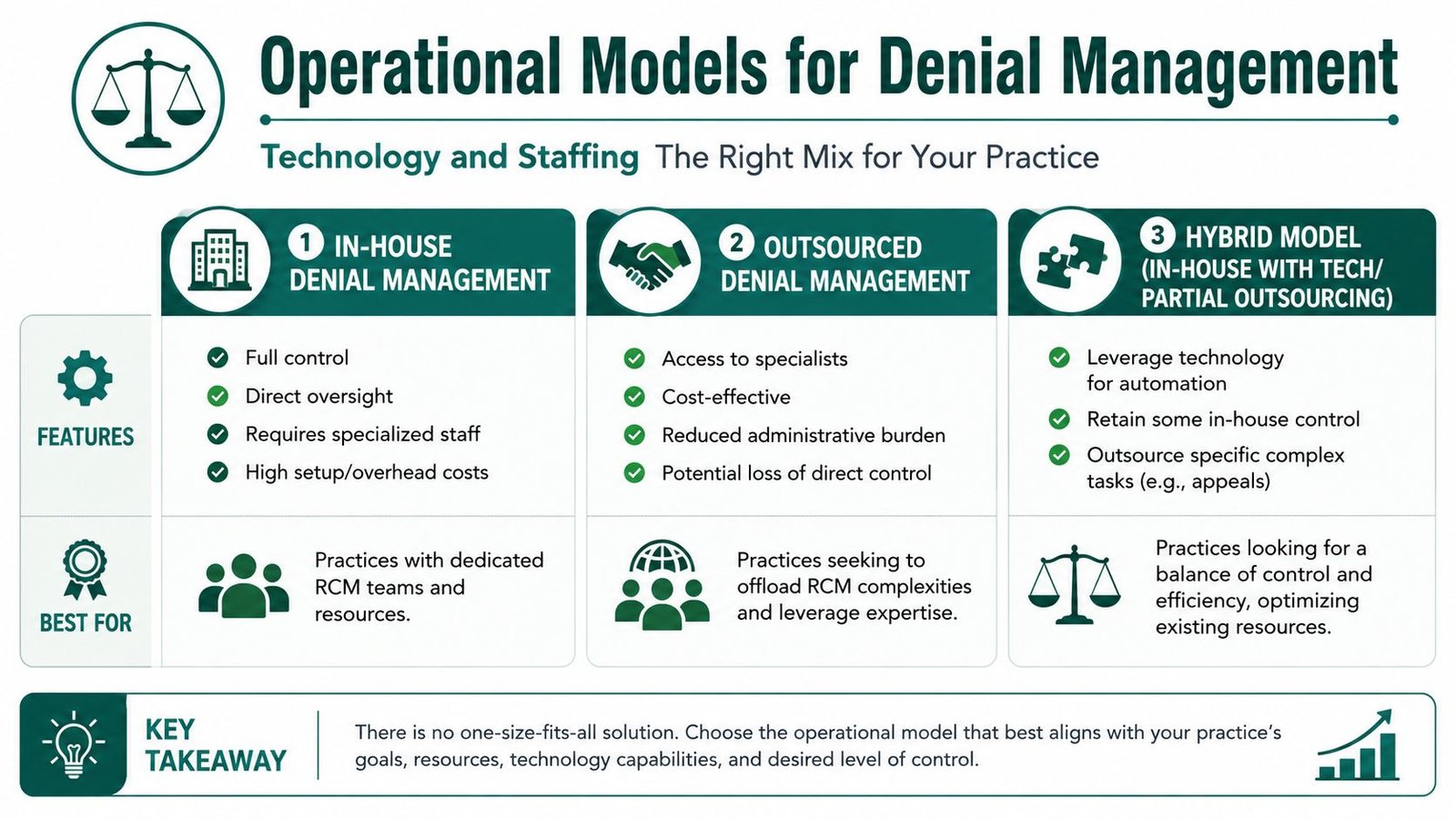
In-house, outsourced, or hybrid
Here is the trade-off:
| Model | What works | Where it breaks |
|---|---|---|
| In-house | Strong visibility, immediate physician access, direct control | Hard to maintain payer expertise, training depth, and coverage |
| Outsourced | Specialized denial teams, broader payer pattern recognition, less admin burden on staff | Can lose nuance if the vendor isn't specialty-specific |
| Hybrid | Internal oversight plus external expertise for prevention, analytics, or appeals | Requires clean role definition and accountability |
For many independent groups, a hybrid model makes the most sense. Keep local ownership of scheduling, front-end intake, and physician documentation habits. Use external expertise and automation for claim scrub rules, denial analytics, appeal workflows, and payer pattern management.
What technology should actually do
Too many practices buy software that produces dashboards but doesn't change outcomes. Good denial technology should do three things well:
- Flag risk before submission: Missing authorization, payer mismatch, modifier logic, or documentation gaps
- Sort denials intelligently after remittance: By payer, root cause, deadline pressure, and work type
- Support specialty nuance: Anesthesia concurrency, cardiology medical necessity patterns, orthopedic global-period edits
Speech and documentation tools can also help if physician notes are contributing to denials. For groups evaluating workflow tools, this guide for healthcare professionals is a useful reference on how voice documentation fits into clinical operations.
Human expertise still matters
Automation is best at speed, consistency, and screening. Humans are still better at argument, escalation, and specialty judgment.
That matters when:
- a payer disputes medical necessity,
- a documentation gap needs physician clarification,
- or a modifier issue depends on operative detail and payer interpretation.
We've seen practices over-automate low-value tasks and underinvest in high-judgment review. The result is usually more throughput, not better collections. For owners, the right question isn't whether to use AI. It's where AI should stop and an experienced denial specialist should take over.
Denial Management in Your Specialty
Generic denial advice falls apart when specialty economics are different. Cardiology, anesthesia, and orthopedics each lose money in different ways, and the denial strategy has to reflect that.
Cardiology
Cardiology denials often revolve around medical necessity, diagnosis support, and payer scrutiny of diagnostic testing. A claim for CPT 93306 may be clinically appropriate, but if the diagnosis linkage or note doesn't support the payer's coverage logic, payment gets delayed or denied.
For the owner of a cardiology group, this creates two costs. The immediate cost is cash delay on a diagnostic service already performed. The larger cost is repeat behavior. If one physician documents loosely and the template doesn't support payer review, the same denial pattern keeps spreading across the schedule.
A practical specialty resource on this point is cardiology billing denials and how to reduce them.
Anesthesia
Anesthesia denials are usually less about generic claim edits and more about precision. Modifier QK is a good example. If medical direction is billed but the record, timing, or concurrency support doesn't align with payer expectations, the claim can be denied or downcoded.
In anesthesia, small consistency problems become major financial leakage because the same issue can affect a large volume of cases. Owners should ask whether the team is auditing modifiers such as AA, QK, QX, and QZ against the anesthesia record and payer rules, not just posting charges.
For practices evaluating specialty support, the broader specialty billing solutions page gives a useful view of where different service lines need different controls.
Orthopedics
Orthopedic denials often cluster around global periods, post-op visits, multiple procedure logic, and modifier use. If the practice bills a service during a global period without the right supporting modifier or documentation, the payer may deny it even when the work was separate and legitimate.
Modifier decisions such as 24, 25, 57, 58, 59, 76, 78, and 79 aren't abstract coding details in this setting. They determine whether post-op and procedural work is recognized as billable revenue or absorbed as unreimbursed effort. In orthopedics, that's where owners often discover that denial management isn't only about getting paid. It's about defending the economic boundaries of work the practice performed.
Specialty denial management works best when the team knows not only the code set, but the business model behind the specialty.
Frequently Asked Questions by Practice Owners
What is a good denial rate for a medical practice
A practical benchmark is to keep your denial rate under 5%. If you're materially above that, don't assume the problem is one payer or one biller. It usually means there are breakdowns in eligibility, authorization, documentation, coding, or pre-submission review that need to be fixed systematically.
When should we appeal a denial versus write it off
Appeal when the claim is recoverable, financially meaningful, and still within the payer's filing window. Write off faster when the claim has no realistic recovery path and the labor required would pull your team away from collectible revenue. The mistake is treating every denial as equally worth chasing.
Do we need a new EHR to improve denial management
Usually not. Most practices can improve denial performance by tightening front-end intake, creating better authorization control, cleaning up charge capture, and adding stronger pre-submission edits inside the current workflow. The bigger issue is usually process discipline, not software replacement.
Should a physician owner outsource denial management or keep it in-house
That depends on your current denial rate, internal staff bandwidth, and specialty complexity. If your team can prevent denials, analyze payer patterns, and manage appeals on time, in-house can work. If denials are dragging cash flow, A/R days are climbing, or specialty-specific errors keep repeating, outside expertise or a hybrid model is often the better financial decision.
If your practice is seeing recurring denials, slow cash flow, or aging A/R that doesn't match clinical volume, Happy Billing can help you diagnose where revenue is leaking and what to fix first. You can request a free RCM audit to review denial patterns, payer behavior, and specialty-specific workflow gaps without changing your EHR or disrupting operations.