How to Reduce Claim Denials: A Practice Owner’s Playbook
Practices that let denials pile up often never recover a meaningful share of that revenue. A denied claim is not just a billing defect. It is a broken operating step that keeps draining cash until someone finds the source and fixes it.
For an owner, a high denial rate hits the income statement from several directions at once. Cash arrives later. Staff spend more time on rework. Write-off risk rises as filing deadlines pass. The underlying cause usually sits upstream in eligibility, authorization, coding, charge capture, or follow-up, so the same mistake can repeat across dozens of encounters before anyone notices.
The practical question is not how to reduce claim denials. The better question is how to build a repeatable denial-control loop: diagnose the pattern, correct the workflow creating it, and monitor the KPIs that show whether the fix is holding. That is why denial management belongs beside collections, A/R days, and other revenue cycle performance metrics on the owner dashboard.
This also ties directly to efforts to reduce waste and boost growth. Strong denial control improves margin without adding visits, and many practices can tighten this process with better workflow discipline, targeted automation, or outside RCM support rather than a painful EHR migration.
Why Your Denial Rate Is a Critical Practice Metric
A denial rate tells you whether your revenue cycle is controlled or drifting. If denials keep climbing, your practice is spending more labor on repair work and waiting longer to turn encounters into cash.
Industry guidance says organizations that treat denials as exceptions often keep denial rates below 5%, and some reach 2% when they maintain proactive front-end controls and monitor KPIs continuously, as noted by Medcare's denial reduction guidance. That's the operational target. Not perfection, but control.
Why owners should care before the month closes
A denied claim is rarely a one-time defect. If the problem is a broken insurance verification step, a missing authorization habit, or a modifier rule your team keeps missing, the same error can repeat across days or weeks of encounters before anyone catches it.
That's why denial rate belongs on the same dashboard as charges, collections, and A/R days. If you already track production but not denial trends, you're measuring work done, not money kept.
For owners trying to reduce waste and boost growth, denial management is one of the clearest operational efficiency projects in the practice. Every avoidable denial creates duplicated labor, delayed collections, and avoidable write-off risk.
Practical rule: If a denial can be predicted before submission, it should never become back-end work.
What a high denial rate usually means operationally
In most independent groups, high denials trace back to a short list of failures:
- Front-desk capture errors that put wrong demographics or inactive coverage onto the claim
- Authorization breakdowns where the service was scheduled before payer requirements were confirmed
- Coding and modifier misses that leave revenue on the table or trigger payer edits
- Weak follow-up discipline that lets denied claims sit until timely filing risk appears
Owners need a small, visible KPI set. A practical starting point is denial rate, top denial categories, dollars denied, and time-to-resolution. If you need a baseline framework, this overview of revenue cycle performance metrics is useful for deciding what belongs on an executive dashboard.
What works and what doesn't
Here's the trade-off most practices eventually face:
| Approach | What happens |
|---|---|
| Treat denials as routine cleanup | Staff stay busy, but root causes survive and cash stays delayed |
| Treat denials as process failures | Fewer repeat errors, cleaner submissions, and less rework |
| Rely mainly on appeals | You recover some money, but the same denials keep coming back |
| Fix defects before submission | You protect cash flow earlier and reduce labor burn |
A practice owner doesn't need more billing activity. A practice owner needs fewer preventable denials.
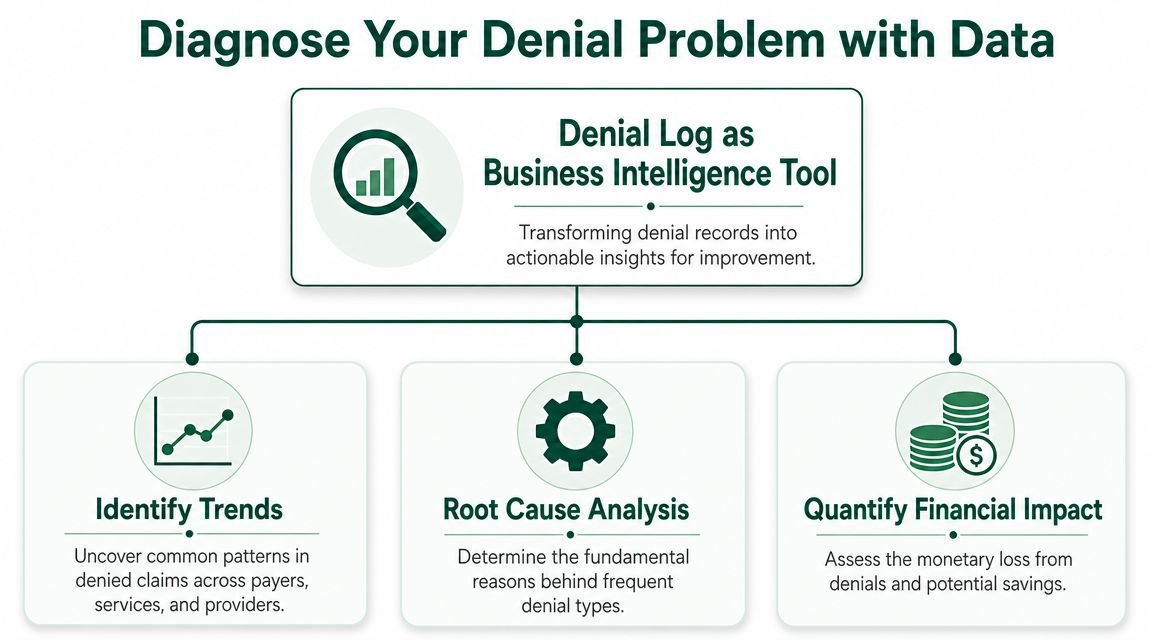
Diagnose Your Denial Problem with Data
Most denial reports are too shallow to be useful. They list payer responses, maybe a denial code, then stop. That isn't enough to manage the business.
The better approach is to turn the denial log into an operating tool. Leapfrog BI recommends a 3-step loop: quantify the problem with KPIs, rank denials by financial impact and frequency, and correct the upstream business process causing the issue, using segmentation by payer, procedure, and reason code to isolate the exact failure point in the workflow, as outlined in Leapfrog BI's denial reduction framework.
Start with segmentation, not anecdotes
The wrong question is, “Why did this claim deny?”
The right question is, “Which combination of payer, CPT, diagnosis, modifier, provider, and work queue is producing the most repeatable revenue loss?”
That shift matters because it changes denial management from reactive billing work into business intelligence. If one payer keeps denying an orthopedic follow-up tied to a global-period issue, that's not an isolated denial. It's a process defect. If behavioral health claims are denying around authorization or coverage checks, the problem likely starts before the encounter, not in accounts receivable.
Teams that struggle with this often need the same discipline used in analytics projects: standardize fields, remove inconsistent labels, and make the data usable before looking for patterns. This primer on preprocessing data for insights is a good example of why raw operational data has to be cleaned before it can guide decisions.
The three numbers owners should review every week
If your billing team sends you a giant denial spreadsheet, simplify it. You need a compact management view.
Denial rate
This shows whether the system is becoming cleaner or noisier.Dollars denied
Count matters, but financial impact matters more. One payer edit on a high-value procedural line can matter more than a pile of smaller denials.Top recurring denial categories
Group by root cause such as eligibility, authorization, coding specificity, modifier mismatch, documentation support, or payer filing rule.
A denial dashboard should tell you where money is getting stuck, who owns the fix, and whether the same defect showed up again this week.
Rank by impact, then assign ownership
Once the data is visible, rank denial categories by two factors: frequency and financial consequence. Then tie each category to a person and a workflow owner.
For example:
- Eligibility denials belong with registration and insurance verification
- Authorization denials belong with scheduling and pre-cert workflows
- Modifier denials usually belong with coding review and specialty education
- Documentation denials often need provider feedback, not just billing edits
Many groups often stall here. They measure denials but never create accountability for the upstream repair.
A practical companion to that process is a KPI framework like this guide to medical billing KPIs to track. The point is not more reports. The point is making denial patterns visible enough that your team can't ignore them.
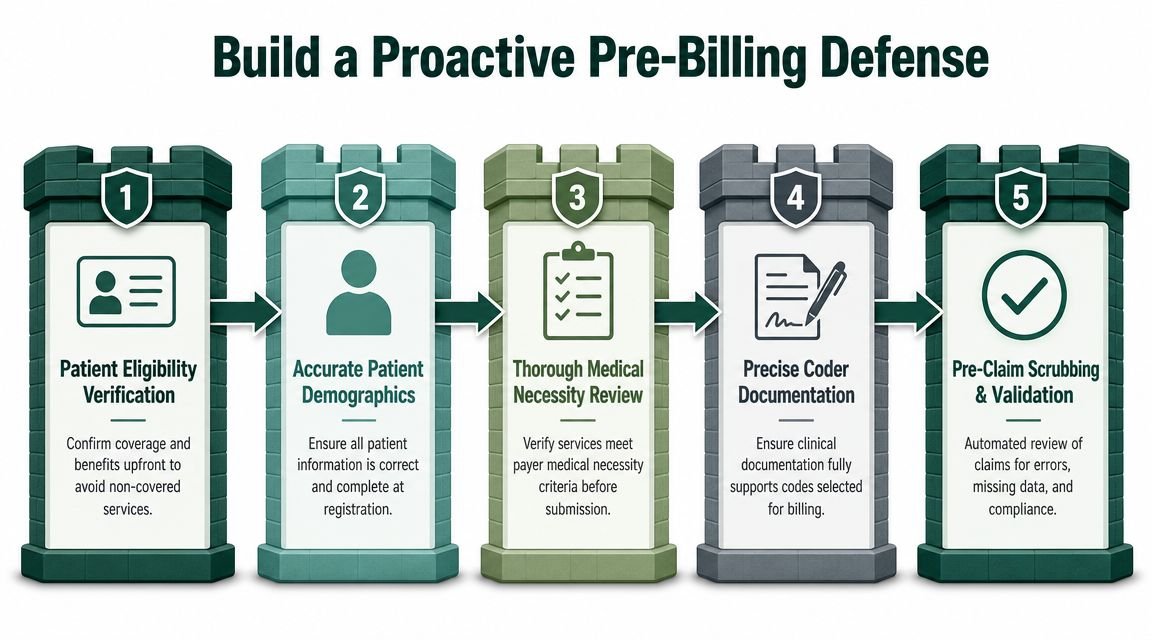
Build a Proactive Pre-Billing Defense
The cheapest denial to manage is the one that never gets submitted. That means your strongest advantage sits before charge entry, not after a payer rejection posts.
FinThrive's 2025 guidance reports that nearly 82% of prior authorization denials are overturned on appeal, which strongly suggests many of those denials are avoidable administrative problems rather than true medical necessity disputes, as discussed in FinThrive's denial prevention guidance. Owners should read that as a process warning. If a denial is frequently overturned, your staff likely had the ingredients to get it right the first time.
Three controls that stop the most expensive mistakes
A pre-billing defense doesn't need to be fancy. It needs to be consistent.
Real-time eligibility verification
Verify active coverage and plan details before the visit or procedure. Don't rely on last visit's insurance card. A front-desk shortcut here creates downstream denials your billers can't cleanly fix.Prior authorization management
Confirm whether the planned service requires authorization, and whether the authorization matches the exact service set expected to bill. For procedural specialties, that means checking code-level alignment, not just confirming “auth on file.”Pre-submission claim scrubbing
Use edits to catch missing demographics, invalid modifiers, diagnosis-to-procedure mismatches, and payer-specific formatting issues before the claim leaves the practice.
Clean claims protect owner economics
A clean claim is not just a billing ideal. It's a margin protection strategy. ACFAS emphasizes filing a clean, error-free claim the first time because even small mistakes such as wrong patient information, missing modifiers, or inaccurate codes can trigger rejection. For an owner, that translates into slower collections, more touches per claim, and staff time diverted from productive work.
This is especially important in specialties with heavy rule complexity:
| Specialty context | Common front-end risk | Financial consequence |
|---|---|---|
| Behavioral health | Coverage and authorization mismatch | Visits get denied after service delivery |
| Cardiology | Procedure-specific payer rules | High-value diagnostics can stall in A/R |
| Orthopedics | Surgical authorization defects | Expensive cases move into appeal cycles |
| Anesthesia | Modifier and documentation gaps upstream | Claims require rework before payment |
If the payer can reject a claim based on information your team knew before the encounter, that denial belongs to operations, not collections.
A useful benchmark for your internal process is whether your team consistently produces a clean claim in medical billing. If that definition isn't operationalized by role, your denial rate will stay stubborn.
Reinforce Your Coding and Documentation Hygiene
Some denials come from front-end mistakes. Others come from revenue that was never defensible because the coding or documentation didn't support the claim.
Owners in specialty practices often experience subtle financial losses. These are incurred not through dramatic compliance failures, but through missing specificity, incorrect modifier use, weak note support, or coding habits that don't match payer rules.
Small coding misses become large revenue leaks
Take anesthesiology. If the record supports a qualifying circumstances add-on code such as +99100 and the claim goes out without it, the practice may collect less than it earned. If the physical status modifier isn't aligned with the documentation, the claim may not reflect the full complexity of the case.
In orthopedics, the opposite problem is common. A post-op visit billed during a global period without the correct modifier can trigger a denial that was entirely predictable. If the visit is unrelated and the documentation supports it, the claim has to communicate that clearly. Otherwise, the payer sees bundled follow-up care and denies it.
For office-based specialties, E/M services often create the same problem. A separate evaluation on the same day as a procedure may require a modifier, but the modifier only works when the note supports a distinct service. That's why owners should make sure clinicians and billing leads both understand when CPT modifier 25 protects legitimate revenue and when it invites payer scrutiny.
Documentation has to defend the code
A useful way to look at specialty billing is this:
- Coding chooses the revenue opportunity
- Documentation defends it
- Payer rules decide whether it survives first pass
If any one of those breaks, you either lose revenue or create rework.
We've seen this most clearly in high-stakes specialties. An anesthesia group may know its base units and time reporting cold, but still lose money if concurrency support or modifier logic isn't consistent. An orthopedic group may perform excellent surgery, then lose post-op related revenue because global-period distinctions aren't communicated cleanly in the chart and on the claim.
For practices with complex procedural billing, regular internal audits around your most common CPT families are more useful than generic coding meetings. That's especially true in fields like anesthesiology billing, where a small modifier error can change reimbursement or trigger denial logic.
Good documentation isn't “more words.” It's the exact detail the payer needs to understand why this billed service should be paid.
What works better than broad retraining
The most effective coding improvement plans are narrow and repetitive. Review the claims that produce the most dollars, identify the modifiers or documentation elements that repeatedly fail, and train only on those patterns.
That is more useful than sending everyone to generic coding refreshers and hoping denial rates improve on their own.
Systematize Your Denial Triage and Appeals
Denied claims do not become revenue just because they sit in a work queue. Practices lose cash when recoverable denials age out, miss filing deadlines, or get written off because nobody decided what was worth pursuing.
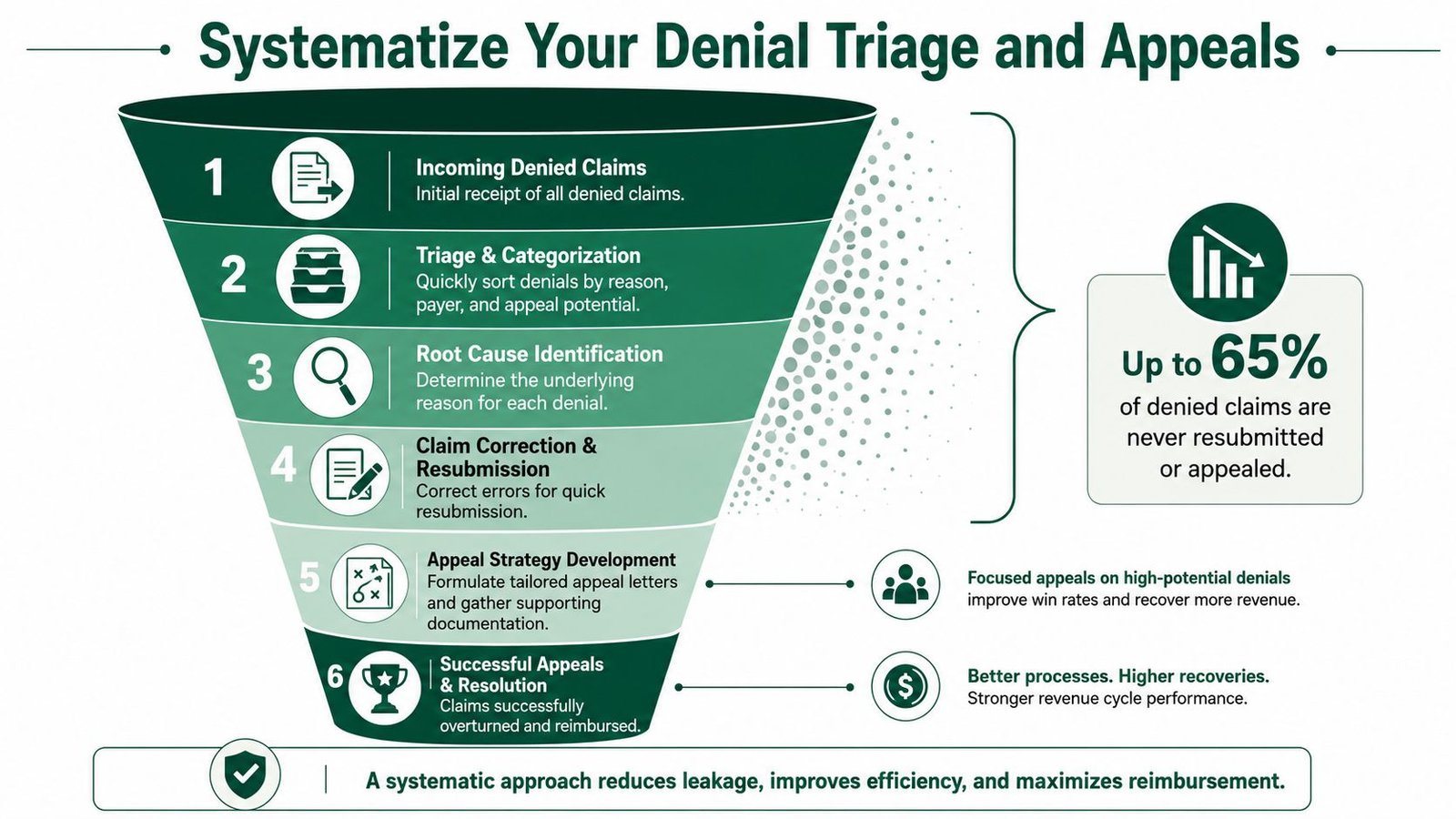
The operational goal is simple. Diagnose the denial, assign the right response, fix the upstream process, and watch whether the same denial comes back next month. That loop matters more than appeal volume. A busy billing team can close a lot of denial tasks and still leave the practice with the same revenue leak.
Triage by recoverability, value, and deadline
Appeals should be prioritized like any other financial work. A $25 coding denial with weak support should not consume the same staff time as a $2,500 surgical claim denied for missing records.
A practical framework looks like this:
| Denial type | Best action |
|---|---|
| High value and likely recoverable | Assign quickly to senior staff and correct fast |
| Lower value but repetitive and recoverable | Batch, template, and automate the response |
| High value but weak appeal odds | Review medical necessity, contract terms, and prevention options before spending more labor |
| Low value and poor odds | Close promptly and redirect staff time to claims with better return |
That is basic denial economics. Every hour spent on low-yield appeals is an hour not spent recovering better dollars or fixing the process that caused the denial in the first place.
Build payer-specific playbooks that reduce rework
Strong teams do not start from zero on every denial. They use payer-specific playbooks that tell staff what the denial usually means, who owns the correction, what documentation is needed, whether to resubmit or formally appeal, and how fast the payer clock runs.
Many practices lose margin when a denial gets touched by billing, then coding, then the provider, then billing again, with no standard path. Turn that into a defined workflow instead. If one payer repeatedly denies behavioral health claims for incomplete authorization fields, the playbook should route the correction, attach the required support, and flag scheduling or intake to fix the source.
For practices trying to tighten this process without replacing their core systems, revenue cycle management automation tools can help standardize queues, assignment rules, and status tracking around the workflows you already have.
Every appeal should produce an operational lesson
A denial unit should recover cash and generate feedback. If the same denial reason appears every week and nothing changes upstream, the practice is paying for rework over and over.
Track denial reasons in a way that helps operations act on them. "CO-16" is not enough. Translate that into plain-language categories such as missing authorization, invalid modifier, medical records not sent, eligibility mismatch, or timely filing miss. Then assign each category to the department that can prevent it.
I advise practices to review three questions every month:
- Which denial categories produced the largest dollar loss?
- Which categories were most recoverable?
- Which categories repeated after an appeal or corrected claim?
Those answers tell you where to train, where to automate, and where to stop wasting labor.
Turn follow-up into a measured profit recovery function
Denial follow-up needs clear KPIs, not vague expectations to "work the aging." Measure appeal win rate, dollars recovered per full-time employee, average days to resolution, timely filing losses, and repeat denials by payer and reason code. If a payer takes too long or overturn rates are consistently poor, that is a contract management issue as much as a billing issue.
Documentation intake matters here too. Missing forms, incomplete questionnaires, and unstructured patient information often create downstream rework before an appeal even starts. Practices that want cleaner intake workflows can review BuildForm's guide to form integration for examples of how to connect front-end data capture with back-office processes.
The best appeal teams do three things well. They recover high-probability dollars quickly, close low-value dead ends without debate, and send denial patterns back to the people who can prevent them. That is how denial management stops being a cleanup task and starts protecting margin.
Integrate Technology and Partners Without an EHR Migration
Most practice owners already know what needs fixing. The primary problem is capacity. Your front desk is busy, your physicians are documenting under pressure, and your billing staff is buried in payer work.
That's why technology matters most when it reduces manual decisions at the exact points where denials start. Experian Health's 2025 State of Claims Report says 14% of organizations reported using AI in their claims process, and among those adopters, 69% said AI boosted claims success rates by reducing denials and/or increasing the success of resubmissions, as reported in Experian Health's State of Claims Report coverage.

Where technology actually helps
The best use of automation is not replacing judgment. It's removing repetitive failure points.
That usually means:
- Eligibility checks run consistently before the encounter
- Authorization requirements are flagged before scheduling mistakes become claim denials
- Claim scrubbers catch common edit failures before submission
- Work queues route denials by payer, reason, and value
- Analytics show whether a fix reduced repeat denials
For many practices, the fear is that any meaningful RCM improvement requires a disruptive platform change. It usually doesn't. A lot of denial prevention can be added around the existing EHR, practice management system, clearinghouse, and intake workflow.
If your intake process itself is part of the problem, it helps to think in workflow terms. This overview of BuildForm's guide to form integration is a good reminder that data capture quality often depends on how well front-end forms connect to the rest of the process.
What to look for in an outside partner
If you're considering help, the key question isn't “Do they submit claims?” It's “Can they run the denial prevention loop inside our current environment?”
A competent RCM partner should be able to work within your existing systems, tighten controls around clean claims, and produce visible reporting on denial categories, root causes, and corrective actions. If they need a full migration before they can improve your process, that's often a warning sign.
You should also expect a clear explanation of how they use automation. This resource on revenue cycle management automation is a solid baseline for evaluating whether a vendor is offering real workflow improvement or just another layer of software.
If your internal team can't tell you where denials start, which ones are financially worth chasing, and which workflow changes would reduce them fastest, it's time for a complimentary billing audit.
Frequently Asked Questions
How much does a high denial rate really cost my practice
More than the posted denial percentage suggests.
The obvious loss is delayed or missed reimbursement. The larger cost usually sits in labor. Staff time shifts from clean claim production to rework, payer calls, corrected claims, appeals, and status checks. That lowers team capacity and raises the cost to collect.
Over time, denial drag also pushes up A/R days and increases the chance that otherwise collectible balances turn into write-offs.
When should we stop trying to fix denials internally
The right point is usually when the practice can no longer connect denials to a specific owner, workflow step, and financial impact.
If the same denials keep showing up by payer, CPT family, modifier, or authorization type, and your team is still treating them as one-off events, the process needs more structure than most internal teams can spare. I usually tell physician-owners to look at one question first. Can your team identify the top denial categories, assign root cause, make the upstream fix, and prove the rate is dropping over the next 30 to 60 days? If not, the issue is no longer just staffing. It is operating discipline.
Can AI reduce denials without becoming an IT project
Yes, if you use it to tighten the denial prevention loop inside your current systems.
The best use cases are narrow and measurable: eligibility checks before the visit, claim edit review before submission, denial categorization after remits post, and work queues that route high-value accounts first. That approach gives a practice faster feedback on where revenue is leaking without forcing a full EHR change. AI should shorten the time between diagnosis, process correction, and KPI review. If it adds another dashboard no one uses, it is overhead, not improvement.
Which specialties usually benefit most from denial reduction work
Any practice with payer complexity can benefit, but the financial gains show up fastest where rules change often and documentation errors are expensive.
Authorization-heavy and modifier-sensitive specialties usually see the quickest return. Behavioral health, cardiology, orthopedics, pain management, and anesthesia are common examples because small front-end or coding fixes can prevent repeated downstream rework. The specialty matters less than the pattern. If denials cluster around prior auth, medical necessity, coding specificity, or registration accuracy, there is usually money to recover and protect.
If your practice is reworking the same denials every month, Happy Billing helps physician owners build a tighter revenue cycle without forcing an EHR migration. We combine specialty billing expertise, denial analytics, and AI-assisted workflows to identify root causes, repair the upstream process, and track whether the fix is improving cash flow. If you want an outside read on where your billing operation is leaking revenue, ask for a revenue cycle audit.