Medical Billing Services Los Angeles: Expert Solutions

Monday morning in a Los Angeles practice often looks the same. The schedule was full last week, clinicians documented the work, and the bank balance still does not reflect it. Claims are sitting in payer edits, a Medi-Cal managed care authorization did not match the rendering provider, a secondary never crossed over, and front-desk staff are trying to collect balances without creating patient billing risk under California rules.
That is why medical billing services in Los Angeles need to do more than submit claims. A billing partner has to protect cash flow, keep A/R from aging out, and catch California-specific payer issues before they turn into write-offs. Generic national vendors miss these details all the time. In this market, that gets expensive fast.
The problem I see most often is not low demand. It is weak reimbursement operations. Practices are busy, but revenue trails production because eligibility was checked too late, modifiers were applied inconsistently, authorizations were incomplete, and payer follow-up lacked urgency. If you want a clear breakdown of the operational work involved, this overview of what medical billers do is a useful reference.
Los Angeles has its own billing environment. Medi-Cal rules and delegated IPA processes vary by plan. Commercial payers apply their own edit logic. Patient balances require more caution here because aggressive or sloppy collections can create legal exposure, reputational damage, and complaints that cost more than the balance you were chasing. Good billing in LA is not just about getting claims out the door. It is about getting paid correctly while staying inside payer rules and California consumer protection expectations.
Practice owners usually focus on staffing first. I get that. But billing problems rarely stay in the back office. They affect payroll decisions, provider compensation, expansion plans, and patient experience. Even your growth efforts can stall if operations are leaking revenue. Strong outreach matters, and so does marketing that feels like you, but marketing cannot fix a broken revenue cycle.
What Are Medical Billing Services
Medical billing services are your external finance department for reimbursement. They take what your clinicians document, convert it into claims that pay correctly, and manage the work between date of service and money in the bank.
For a Los Angeles practice, that usually means fixing a familiar pattern. Patient volume is solid, but cash flow is flat. Anthem Blue Cross, Health Net, and other payers kick claims back for avoidable reasons. A/R creeps upward, staff spends more time chasing claims than preventing denials, and the practice owner starts subsidizing revenue leakage with longer hours and tighter payroll decisions.
A real billing partner doesn't just transmit claims. The job includes charge entry, eligibility review, coding review, claim scrubbing, denial management, payment posting, A/R follow-up, and patient-balance workflows that don't create unnecessary friction. If you want a plain-language breakdown of the actual work, this overview of what medical billers do is useful.
Why LA practices outsource this function
The market has moved in that direction for a reason. The U.S. medical billing outsourcing market was valued at USD 5.7 billion in 2023 and is projected to grow at a CAGR of 11.78% from 2024 through 2030, reflecting strong demand in major markets like Los Angeles, according to CPA Medical Billing's market review.
That growth tracks what we see on the ground. Independent groups don't outsource because billing is mysterious. They outsource because payer rules keep changing, software matters, and weak process discipline erodes collections.
Practical rule: If your front desk verifies coverage, your clinicians document properly, and your practice still waits too long to get paid, the problem is probably not volume. It's revenue cycle execution.
What the service should actually improve
A billing service is worth keeping only if it improves financial control in three places:
- Claim quality at submission: Bad claims create rework, delay cash, and increase write-offs.
- Denial response discipline: The first denial is expensive. The second touch is more expensive.
- Visibility for ownership: A practice owner should know where money is getting stuck by payer, provider, and service line.
One more point gets overlooked. A strong billing operation also supports brand trust. If you're working on patient acquisition and retention, sloppy statements and unresolved payer errors undercut that effort. That's why practice owners often pair RCM cleanup with broader operational messaging and marketing that feels like you, rather than treating billing and reputation as separate issues.
Outsourcing vs In-House Billing for LA Practices
A Beverly Hills specialist can stay busy for a full month, see a healthy payer mix on paper, and still end the month short on cash because claims are sitting in portal limbo, authorizations were mishandled, or a staff absence slowed follow-up. That is the real decision here. LA practices are not choosing between two abstract billing models. They are choosing which setup is more likely to protect collections in a market with California-specific rules, aggressive payer edits, and legal exposure around patient balances.
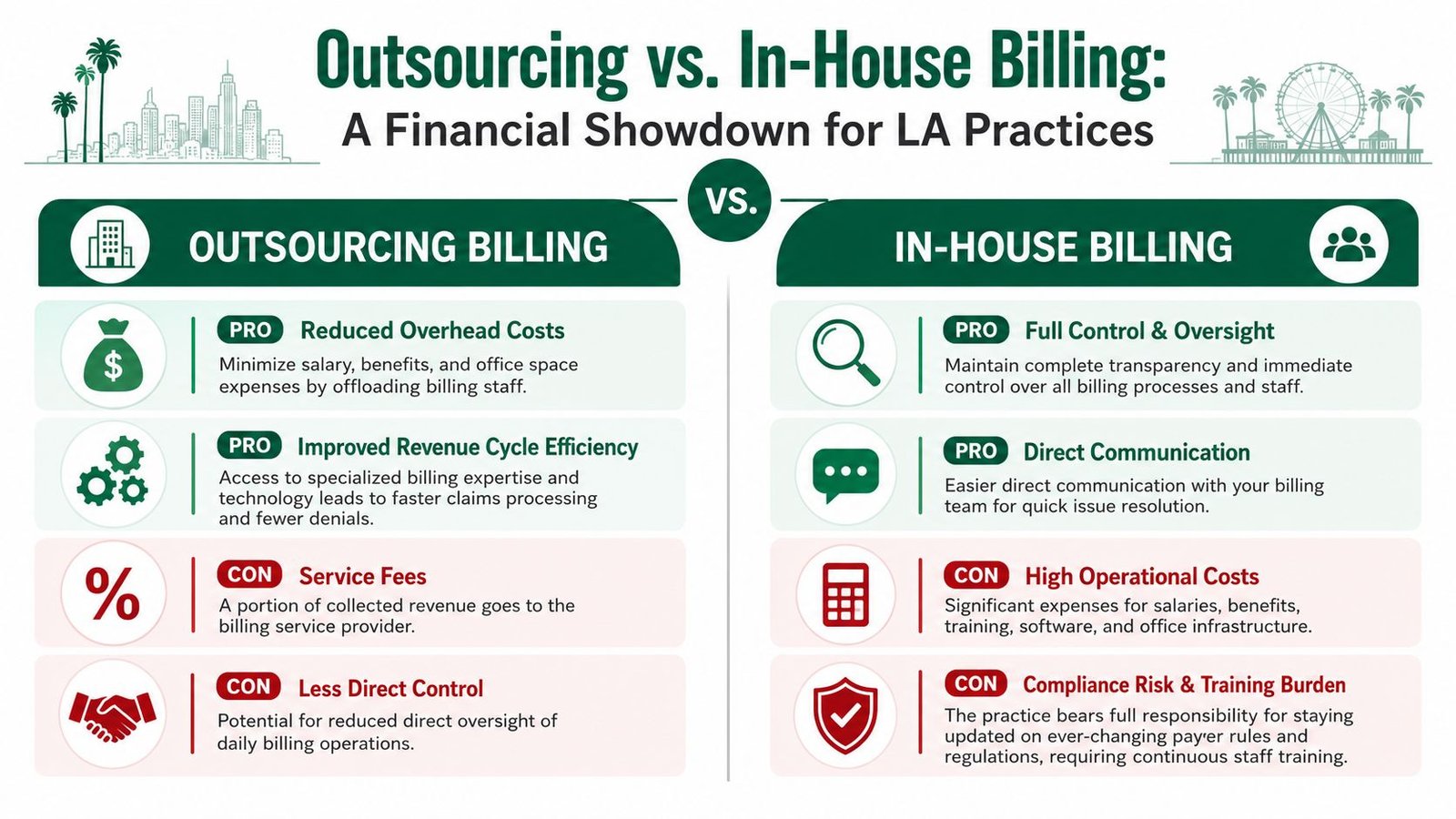
What in-house gets right
In-house billing gives owners direct control. The biller is on site. Front-desk questions get answered quickly. Providers can correct documentation issues faster when the billing team is part of the same daily workflow.
That setup can work well for a smaller practice with low claim complexity, stable staffing, and a physician-owner who reviews reports consistently.
In Los Angeles, that last part matters more than owners expect. An internal team needs active management to keep up with payer portal changes, California billing updates, IPA requirements, timely filing rules, and the operational impact of state scrutiny around patient billing and collections. If leadership is not reviewing denial categories, aging by payer, and auth-related write-offs every month, in-house billing becomes expensive very quickly.
Where in-house usually breaks down
The pressure point is redundancy.
One strong biller may be excellent at charge entry and payment posting but still fall behind on appeals, secondary claims, underpayment review, and portal follow-up. Once that person takes vacation, gets sick, or leaves, cash slows down within weeks. I see this often in independent LA groups that assume a loyal biller and a decent PM system are enough. They are not enough when the practice deals with Medi-Cal managed care, multiple commercial plans, outsourced coding questions, and specialty-specific modifier rules at the same time.
If you are weighing whether your current setup can scale, this guide to in-house vs outsourced medical billing is a useful reference for comparing control, cost, and coverage.
Internal billing works best when the practice has backup staff, close physician documentation oversight, and a payer mix that does not require constant exception handling.
What outsourcing changes
Outsourcing shifts billing from a one-person dependency to a process with assigned functions. Claims submission, denial work, payment posting, authorization follow-up, and reporting are handled by different people with specific responsibilities. That structure usually improves consistency first, then cash.
For LA practices, the bigger advantage is not lower payroll. It is error containment. A billing partner that already works inside California rules is less likely to miss Medi-Cal managed care details, local plan quirks, or documentation gaps that later create collection problems. That matters because revenue is only part of the risk. If statements go out with the wrong balance, or staff push patient collections before payer liability is resolved, the practice can create compliance and reputation problems along with bad debt.
The trade-off that actually matters
Outsourcing does reduce hallway access. Owners lose some day-to-day immediacy. The fix is not vague promises about communication. The fix is a reporting cadence, named contacts, defined turnaround times, and clear rules for when denials, credentialing issues, or high-dollar accounts must be escalated.
The decision framework is similar to other specialized business functions. This article on expert advice on marketing decisions is about a different service, but the owner logic is familiar. If the work depends on specialized knowledge, current systems, and consistent execution, an external partner often outperforms a thin internal team.
For most independent Los Angeles practices, the practical answer is straightforward. Keep scheduling, intake, and patient experience close to the office. Outsource billing when your internal team cannot reliably control denials, keep up with California payer rules, and protect the practice from preventable revenue loss.
Navigating the Unique Los Angeles Payer Landscape
Los Angeles isn't just a big market. It's a fragmented payer environment with local rules, managed care layers, IPA relationships, and California Medicaid complexity that generic billing shops often underestimate.
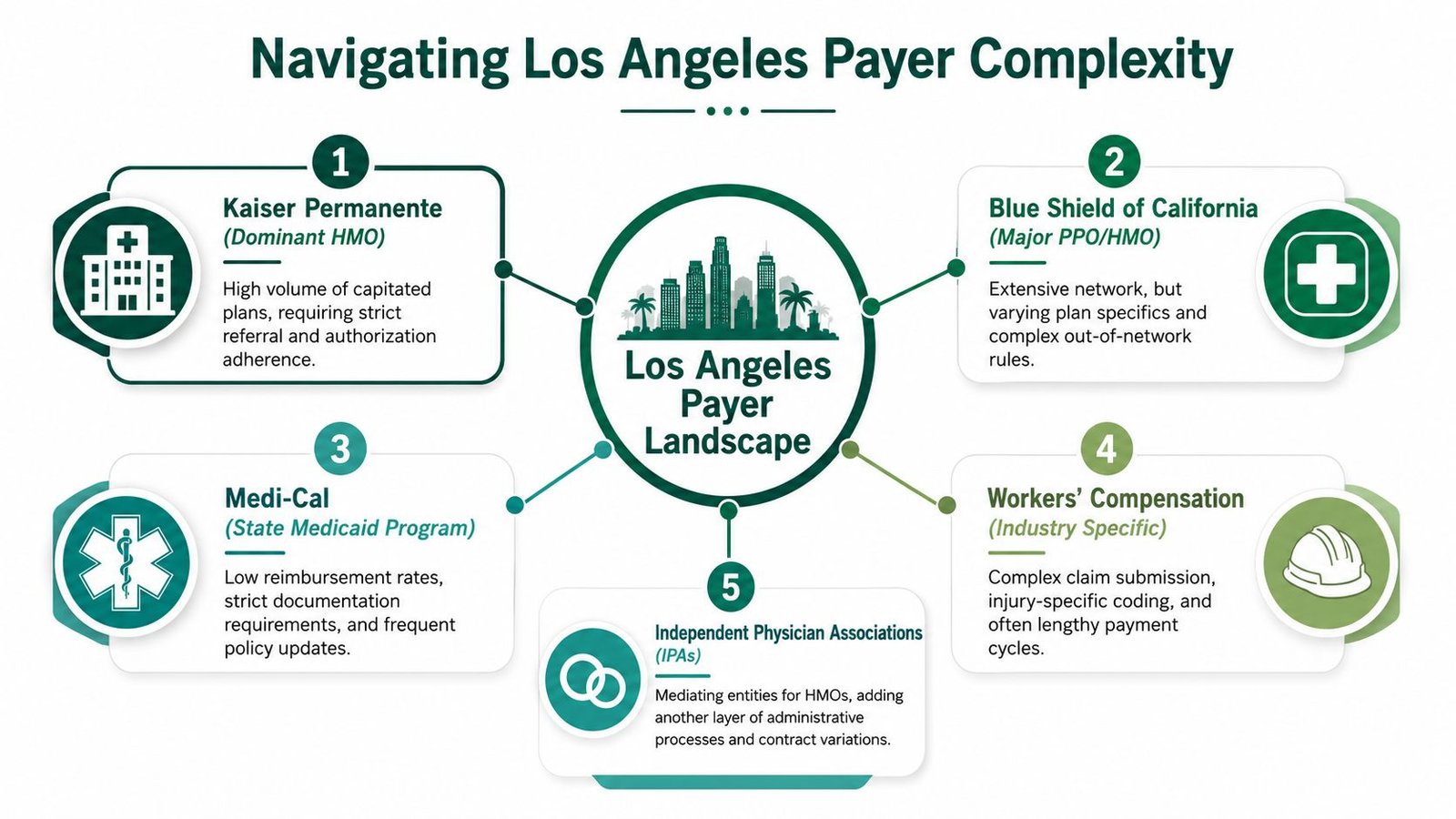
Medi-Cal is where generic billing advice fails
Most content about medical billing services in Los Angeles stays too broad to be useful. A significant issue is that Los Angeles practices contend with unique California Medicaid complexities, including revised telehealth codes and mental health authorization mandates that differ from national standards, as noted by P3Care's California billing analysis.
That matters because state-specific rules aren't side notes. They affect whether the claim pays at all.
An out-of-state billing vendor may understand Medicare well and still mishandle Medi-Cal managed care claims, especially when documentation, authorizations, modifier logic, or telehealth requirements don't mirror national habits. We see this often in behavioral health, urgent care, and multispecialty groups that assume a clean commercial workflow will translate to California Medicaid. It won't.
Specific coding details that hit owner revenue
Practice owners don't need coding lectures. They need to know where money gets lost.
Here are common examples:
- Telehealth coding: If the service setup, place-of-service logic, or payer-specific telehealth requirements don't align with California rules, the claim can deny even when the care was clinically appropriate.
- Urgent care modifiers: Urgent care claims often fail because the service was documented correctly but billed without the payer-specific modifier logic that determines reimbursement pathway.
- Behavioral health authorizations: Recurring therapy services can look routine operationally, but if authorization tracking slips, denials stack quickly and are difficult to reverse after the fact.
- E/M and procedural combinations: Commercial and managed Medi-Cal plans may review these pairings differently, especially when modifier use isn't supported tightly in the note.
A Los Angeles billing partner should also understand how these issues intersect with CMS guidance, AAPC standards, and payer bulletins. That includes modifier use such as 25, 59, and specialty-specific anesthesia modifiers when the note supports them.
Clear documentation isn't enough. The claim has to match the payer's logic, not just the chart.
Billing mistakes can become legal and reputational problems
LA County has another pressure point that billing vendors rarely discuss. Medical debt is a consumer crisis locally, and legal aid groups including Neighborhood Legal Services of Los Angeles County and Bet Tzedek provide free legal services to people facing wage garnishment or lawsuits tied to unpaid hospital bills, according to the Los Angeles County medical debt overview.
For a practice owner, that means poor billing isn't only an internal collections issue. If denials aren't prevented early, statements aren't clear, or patient balances reflect unresolved payer responsibility, the practice can end up fueling disputes that harm reputation and create unnecessary legal friction.
This is also why No Surprises Act workflows belong inside billing operations, not just compliance binders. If you want a practical operational review, this guide on No Surprises Act compliance is worth reading.
How to Evaluate a Medical Billing Partner
Most billing companies sound competent in a sales call. The difference shows up when you ask operational questions they can't answer clearly.
A Los Angeles practice should evaluate a billing partner the way it would evaluate a lead physician hire. Look for depth, pattern recognition, and proof of process. A polished dashboard means very little if the company can't explain how it handles payer-specific denials or specialty nuance.
What to look for first
Start with fit, not price.
- Specialty fluency: If you run anesthesiology, cardiology, orthopedics, mental health, or urgent care, ask how they handle the exact claim types that drive your revenue.
- LA market knowledge: They should be comfortable discussing Medi-Cal managed care, IPA workflows, authorization bottlenecks, and local payer escalation paths.
- Reporting discipline: You need monthly reporting that shows denial categories, A/R aging, payer lag, and unresolved balances in plain English.
- Technology compatibility: The vendor should work inside your existing EHR or practice management setup whenever possible, not create unnecessary migration risk.
- Security posture: Ask direct questions about HIPAA controls, encryption, access management, and oversight if any part of the workforce is distributed globally.
For a sharper checklist, this guide on questions to ask a medical billing company before hiring is a good starting point.
Questions that expose weak vendors
Use questions that force specifics:
| Question | Why it matters |
|---|---|
| How do you appeal a denied claim with LA Care Health Plan? | Tests payer-specific denial skill instead of generic process talk |
| How do you handle CPT 99214 paired with modifier 25 when a procedure is billed the same day? | Reveals whether they understand revenue-impacting documentation and modifier logic |
| What does your monthly report show for A/R aging by payer and provider? | Shows whether ownership will get actionable visibility |
| How do you manage anesthesia concurrency modifiers such as QK and QX? | Critical for high-risk specialties where one modifier mistake changes reimbursement |
| How do you track mental health authorization renewals? | Exposes whether they prevent predictable denials or merely react to them |
Red flags you shouldn't ignore
A few answers should stop the conversation fast.
If the vendor says "we work with all specialties" but can't discuss one claim scenario from yours, they're not a specialist.
Also watch for these signs:
- Vague denial language: "We work denials aggressively" means nothing unless they can explain workflow and ownership.
- No sample reporting: If they won't show a performance report, expect poor transparency later.
- One-size-fits-all onboarding: Los Angeles practices need local payer setup, not a generic implementation template.
- Overfocus on coding alone: Coding matters, but owner outcomes depend on the full cycle from eligibility to appeal.
The best billing partners don't get defensive under scrutiny. They welcome it.
Specialty-Specific Billing Is Non-Negotiable
General billing competence isn't enough for high-stakes specialties. The financial exposure is too large, and the rules are too specific.
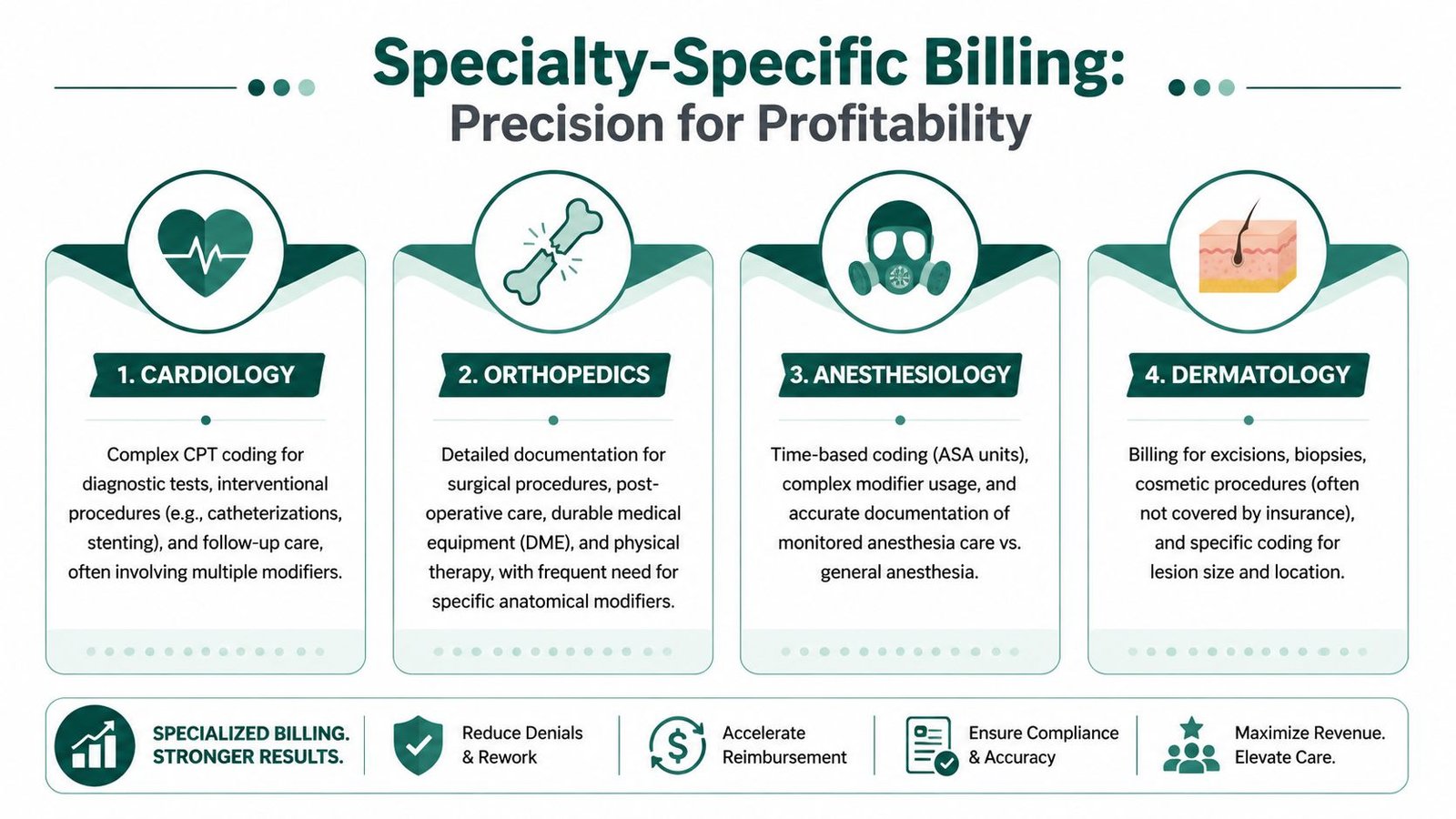
Anesthesiology errors aren't small
Anesthesia billing can look simple to a generalist because every case starts with a CPT anesthesia code and ends with a claim. In practice, reimbursement hinges on base units, time units, physical status, medical direction rules, and concurrency.
If a biller mishandles modifiers like QK, QX, or AA, the payment logic changes. If time isn't captured correctly, the practice loses legitimate reimbursement. If concurrency isn't supported by the record, the claim becomes vulnerable on audit. Our deep expertise in anesthesiology billing exists for exactly this reason. These aren't abstract coding details. They're owner-income details.
Cardiology requires procedural judgment
Cardiology groups often lose revenue in the gray space between documentation and payer interpretation.
Take CPT 93306 for a complete transthoracic echocardiography study. Whether that claim pays smoothly can depend on diagnosis support, modifier use, payer edits, and whether related services create bundling issues. The same is true when E/M services are billed on procedural days and the chart needs to support modifier 25. A general billing team may submit the claim correctly on paper and still miss the combinations that trigger review or delay.
Mental health denial prevention starts before the visit
Behavioral health billing is where weak authorization management subtly erodes collections.
The clinical side may deliver recurring therapy correctly, document consistently, and still run into preventable denials if payer-specific authorization windows aren't tracked tightly. In Los Angeles, those risks increase when Medi-Cal rules and managed care requirements differ from what a national vendor expects. That includes recurring outpatient therapy, telehealth encounters, and plan-specific review rules.
In mental health, the cleanest claim in the world won't pay if the authorization expired last week.
Orthopedics and procedural specialties have their own traps
Orthopedics adds another category of owner risk. Global periods, staged procedures, anatomical modifiers, and post-op visit logic all affect reimbursement. If a billing team doesn't understand when an encounter falls inside a global package, the practice either bills and gets denied or underbills and gives revenue away.
The broader point is simple:
- Different specialties fail in different ways
- Different payers review the same specialty differently
- A billing vendor without specialty depth creates preventable write-offs
That is why "we bill everyone" is usually the wrong answer.
What Measurable RCM Outcomes Should You Expect
A billing partner should be judged on outcomes, not activity. "We submitted claims quickly" isn't a meaningful result if denials stay high and cash still arrives late.
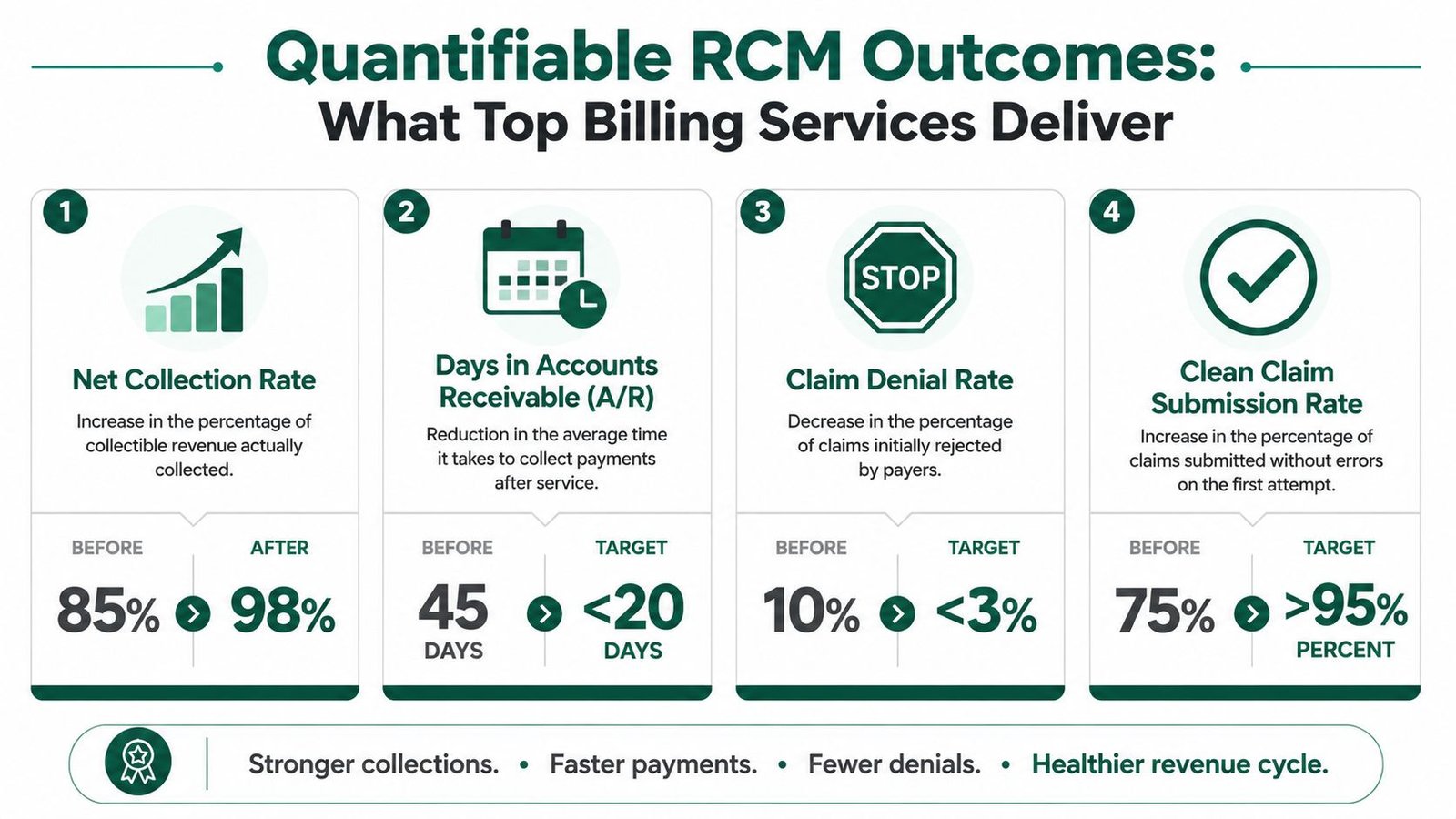
The benchmarks that matter
In Los Angeles, advanced medical billing services use automated claim scrubbing to achieve first-pass acceptance rates exceeding 95%, reduce costly rejections by 30 to 40%, and shorten days in A/R from a regional average of 45 to under 35, according to AnnexMed's California billing benchmarks. That's the level of operational effect an owner should expect from a capable RCM partner.
Those numbers matter because they translate directly into business health:
- Faster first-pass acceptance means less staff rework and fewer stalled payments.
- Lower rejection volume means fewer claims enter the expensive denial cycle.
- A/R under 35 days means stronger cash predictability for payroll, hiring, and growth decisions.
If you want to build an internal scorecard, this list of medical billing KPIs to track gives owners a solid framework.
Results should show up in the monthly report
A strong monthly report should let you answer these questions in minutes:
- Which payer is slowing payment the most?
- Which denial category is growing?
- Which provider has the highest unresolved A/R?
- Which CPT and modifier combinations are producing avoidable edits?
If your current billing company sends aging totals without interpretation, you're not getting management insight. You're getting a spreadsheet.
The right reporting doesn't just tell you what happened. It tells you where revenue is getting stuck and what action fixes it.
At that point, the next move is practical. Discover your practice's potential revenue lift with a complimentary RCM audit.
FAQs From Los Angeles Practice Owners
Practice owners usually ask the same final questions before changing billing partners. The right answers should reduce risk, not create more uncertainty.
Alongside revenue operations, many owners are also thinking about practice growth, referral visibility, and patient communication. If that's on your list too, this comprehensive guide for physician owners is a useful companion read.
How hard is it to switch billing companies without disrupting cash flow
A well-run transition shouldn't require a disruptive rebuild. The key is a controlled handoff of payer enrollments, aging A/R responsibility, open claims, authorization tracking, and posting workflows.
The risk isn't the switch itself. The risk is switching without a transition map. Before signing, ask who owns old A/R, how claim inventory is separated, how payer portals are reassigned, and what happens to denials that arrive during the handoff period.
Will a billing company work inside our current EHR
The best answer is yes, whenever possible.
For most independent practices, forcing a software migration just to change billing vendors creates unnecessary operational drag. A better model is working inside the current EHR and practice management stack, then tightening workflows around eligibility, charge capture, edits, and follow-up. Ask the vendor which systems they already support and how they handle access, audit trails, and user permissions.
How do I know whether my denial problem is a coding issue or a process issue
Usually it's both, but not in equal proportion.
If denials cluster around missing authorizations, eligibility failures, untimely filing, or incomplete follow-up, the problem is process. If they cluster around modifier logic, diagnosis support, bundling edits, or specialty-specific claim construction, the problem leans coding and billing judgment. A competent audit should separate those causes clearly instead of blaming everything on "documentation."
What should I ask for before signing a billing contract
Ask for four things in writing:
- A sample monthly report so you can judge reporting quality
- A transition plan that covers open claims and legacy A/R
- A communication map showing who handles daily issues and escalations
- A specialty workflow explanation using examples from your actual claim types
If a vendor can't provide those cleanly, keep looking.
If your practice is losing time to denials, slow A/R, or California payer complexity, Happy Billing is built for that exact problem. The team specializes in high-stakes specialties, works inside your existing systems, and focuses on the owner metrics that matter most: cleaner claims, faster cash, and fewer preventable write-offs.