Choose the Best Medical Billing Company Houston in 2026
If your Houston practice is dealing with slow cash flow, recurring denials, or old A/R that never seems to move, hiring the right medical billing company in Houston is usually the fastest financial fix available. This isn't an admin decision. It's a revenue decision that affects how quickly you get paid, how much you keep, and how much leakage you tolerate every month.
A lot of physicians wait too long. They keep an underpowered billing setup in place because changing vendors feels disruptive. Meanwhile, claims age, denials pile up, and your front office spends time chasing paperwork instead of supporting patient flow. If your A/R is drifting past healthy levels, if payer rework is consuming staff time, or if coding issues around E/M, modifier 25, global periods, or specialty-specific edits keep showing up, the cost is already hitting your bottom line.
When to Outsource Your Houston Practice's Medical Billing
You should outsource when your current setup is costing you more than it saves. For most independent practices, that shows up in three places first. A/R days remain high, denial volume keeps rising, and your staff gets trapped in billing work that doesn't generate new revenue.
Houston practice owners aren't imagining the shift. The U.S. medical billing outsourcing market was valued at USD 5.7 billion in 2023 and is projected to grow at a CAGR of 11.78%, reflecting a major move toward third-party RCM services, and Houston firms are already using agentic AI with human auditors to achieve first-pass clean claim rates exceeding 98% and reduce days in A/R to under 35 days, according to this industry overview of medical billing outsourcing growth.
Three financial triggers you shouldn't ignore
- A/R is staying too old: When receivables sit too long, your practice funds payroll, rent, and supplies before payers fund you. That's backwards.
- Denials have become routine: If your team treats denials as normal volume instead of preventable failures, margin disappears.
- Your staff is doing payer cleanup instead of practice operations: Every hour spent on status checks, corrected claims, and appeals is an hour not spent on scheduling, collections, or patient throughput.
Practical rule: Outsourcing isn't a sign that your team failed. It's what smart owners do when revenue cycle complexity outgrows the people sitting at the front desk.
What usually causes the problem
In Houston, we often see the same pattern. A growing practice adds providers, payer mix gets messier, prior auth rules shift, and coding gets more specialty-specific. The billing process that worked when the practice was smaller stops working once volume increases.
That's especially true when you're billing services that depend on correct pairing of CPT codes, modifiers, and documentation. A basic example is 99213 or 99214 paired with a same-day minor procedure that may require modifier 25. If your current biller doesn't understand when that modifier is supported, you're either losing reimbursement or increasing audit risk.
The right question to ask
Don't ask, "Can we keep billing in-house?" Ask, "What is our current billing setup costing us in delayed cash, write-offs, and staff drag?" That's the question that matters.
Evaluating a Vendor on Key Financial KPIs
Most billing companies sell responsiveness, experience, and software. Ignore the pitch deck until you see the numbers that matter. For a physician-owner, two KPIs tell you almost everything. First-Pass Clean Claim Rate and Days in Accounts Receivable.
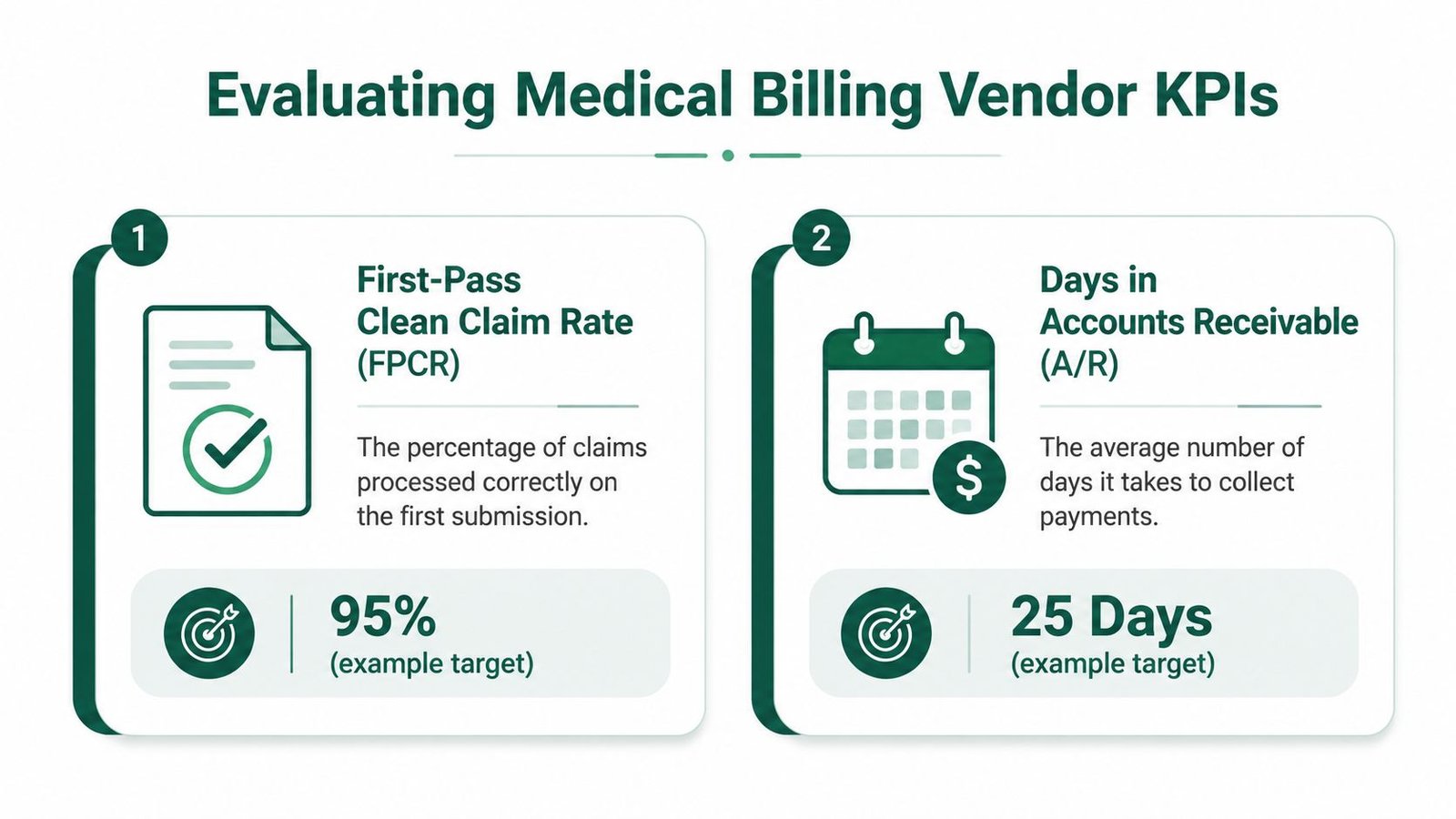
First-pass clean claim rate tells you how much waste you're funding
A claim that doesn't go out clean the first time creates rework. That rework isn't free. The average cost to re-submit a denied claim is approximately $25 to $30 per claim due to administrative labor, and practices with a denial rate above 10% can face $15,000 to $30,000 in annual administrative costs for a practice billing $2M annually, according to Aspirion's discussion of RCM versus medical billing.
That means FPCR isn't a vanity metric. It's a labor cost metric and a leakage metric.
Ask every vendor these questions:
- What is your actual first-pass clean claim rate by specialty?
- How do you define a clean claim?
- Who owns root-cause analysis when rejections cluster around a payer or provider?
- How do you catch edits tied to modifier use, NCCI logic, or payer-specific filing rules before submission?
If the answers are vague, walk away.
Days in A/R tells you how fast your practice turns work into cash
A billing partner can sound great and still collect too slowly. You need speed, not just activity. If a vendor can't explain how it controls charge lag, denial follow-up cadence, unpaid claim work queues, and payer escalation, your cash will stay trapped in receivables.
The best billing partner isn't the one that sends the most reports. It's the one that turns completed visits into deposited cash faster.
Use medical billing KPIs to track as your scorecard when you're comparing vendors, but don't stop at definitions. Make them show you how they manage each number.
Questions that expose real competence
| KPI | What to ask | Why it matters |
|---|---|---|
| FPCR | "What breaks your clean claim rate most often?" | Competent teams know their failure points by payer, code family, and provider habit. |
| A/R days | "How do you handle claims that age without action?" | Old A/R kills cash flow when nobody owns follow-up. |
| Denial handling | "Do you appeal by template or by denial reason?" | Generic appeals waste time and miss recoverable dollars. |
| Coding oversight | "Who audits E/M and modifier usage?" | Errors around codes like 99213, 99214, and modifier 25 can create repeated losses. |
What you should expect
You don't need perfection. You need a vendor that can explain performance in operational terms. If they can't tell you how they reduce payer touches, prevent front-end errors, and keep claims from aging, they probably won't protect your margin once the contract is signed.
Your Houston Medical Billing Company Vetting Checklist
A serious vetting call should feel less like a sales demo and more like a due diligence interview. You're not hiring a receptionist. You're handing over part of your cash flow.
The checklist to use on vendor calls
| Category | Question to Ask | Why It Matters (Red Flag if 'No') |
|---|---|---|
| Security | Do you use HIPAA-first workflows, role-based access, and bank-level encryption for PHI? | Weak security creates compliance exposure and operational risk. |
| EHR workflow | Can you work inside our existing EHR and PM system without forcing a migration? | Forced software changes slow implementation and distract staff. |
| Reporting | Do we get on-demand dashboards and aging visibility without asking for custom exports? | If reporting isn't easy to access, you won't catch problems early. |
| Communication | Will we have one accountable contact who owns escalations? | Shared inbox support usually means slow answers and finger-pointing. |
| Old A/R | Who owns legacy A/R and how will it be worked? | Unassigned old balances usually become write-offs. |
| Credentialing | Will you verify payer enrollment and provider setup before go-live? | Credentialing errors delay claims before billing even starts. |
| Denial process | Do you use payer-specific appeal workflows instead of generic resubmission? | Denial prevention and recovery require payer nuance. |
| Document exchange | How do you handle records and claim support securely? | Loose document handling creates delays and privacy issues. |
What matters more than the sales pitch
A specialized RCM partner can reduce A/R days from an average of 45 to 50 days to under 35 days, which can accelerate cash flow by approximately 20% to 25% for independent practice owners, based on this discussion of outsourced RCM performance. That's why your checklist should focus on operating discipline, not personality.
If a vendor talks endlessly about customer service but can't explain claim edit workflows, payer follow-up cadence, or ownership of unresolved A/R, you're listening to the wrong team.
One operational detail most practices overlook
Document transfer still breaks billing operations more often than it should. If your staff is constantly sending records for appeals, audits, or payer requests, build a secure process before go-live. A practical reference on secure faxing medical records is worth reviewing if your practice still depends on fax-heavy workflows.
Ask one blunt question: "If our cash drops in month one, who on your side fixes it, and how fast do they act?"
For a stronger interview script, use these questions to ask a medical billing company before hiring. It will save you from signing with a vendor that looks polished and performs like a call center.
Why Specialty-Specific Billing Expertise Matters
A generalist billing team can submit claims. That doesn't mean it can protect your revenue. Specialty billing is where practices either preserve margin or bleed it.
Modifier 25 is a small coding detail with a real financial consequence
One of the most common examples is modifier 25. When a provider performs a significant, separately identifiable E/M service on the same day as a minor procedure, the documentation and claim have to support that distinction. If they don't, payers often deny the E/M line.
The financial impact isn't minor. Incorrect CPT coding in high-volume scenarios, including failure to properly apply modifier 25 for minor procedures on the same day as an E/M service, can cause a 10% to 15% loss of reimbursable revenue per claim due to automatic denials by Medicare and commercial payers, according to this review of coding and revenue cycle management that references AAPC standards.
For an owner, the takeaway is simple. If your biller doesn't understand when 99213-25 or 99214-25 is defensible, you're either giving away money or inviting payer scrutiny.
Specialty errors don't look the same across practices
- Orthopedics: Problems often show up around post-op visits, global periods, and multiple procedure reductions. If the team doesn't understand what's bundled and what's separately payable, collection drops.
- Cardiology: The risk is usually in diagnostic testing, interventional coding, and payer edits tied to procedure combinations.
- Mental health: Authorization tracking and visit limits are often the choke point.
- Anesthesiology: Base units, time units, modifiers, and concurrency rules all need close control.
CMS guidance, payer bulletins, and AAPC standards all matter here, but the issue for you is not academic compliance. It's whether the biller can convert those rules into fewer denials and cleaner payment posting.
What real expertise looks like
A capable specialty team doesn't just know code descriptions. It knows what payers deny, what documentation supports appeals, and where providers tend to undercode or misapply modifiers.
Owner's lens: Every specialty-specific billing mistake becomes either a write-off, a delay, or an expensive appeal.
If you're in a procedural or diagnostically complex field, review a partner's actual specialty depth before you sign. A good place to pressure-test fit is their specialty billing experience across cardiology and other specialties, then compare that to your own denial patterns.
Decoding Pricing Models and Finding the True Cost
Pricing is where many practices get distracted. A low quoted rate feels efficient until the hidden work starts showing up as separate fees, slower collections, or internal staff burden.
The three common pricing models
| Pricing model | How it works | Where it fits | What to watch |
|---|---|---|---|
| Percentage of collections | Vendor earns a share of collected revenue | Usually the cleanest alignment for independent practices | Make sure contract language defines what counts as collected revenue |
| Flat fee per claim | Practice pays per claim submitted | Can work for high-volume, predictable environments | This can reward volume over quality if edits and denials aren't tightly managed |
| Fixed monthly fee | Set monthly billing charge | Sometimes useful for stable operations | Risky if claim complexity spikes or service scope becomes vague |
In most physician-owner situations, percentage-based pricing is the easiest model to evaluate because the billing company has a direct incentive to collect. That said, the percentage itself means nothing if the contract excludes old A/R, charges extra for appeals, or leaves credentialing outside scope.
Compare outsourcing against the real cost of in-house labor
In Houston, the mean annual wage for medical records specialists is $49,620, and experienced professionals in hospitals can earn upwards of $60,000, according to this Houston-area salary guide for medical billers and coders. That's your baseline for salary only.
It doesn't include hiring friction, turnover, supervision, training, PTO coverage, coding oversight, or the cost of a weak performer who lets claims age. That's why owners who compare outsourcing only against payroll usually underestimate the true in-house cost.
Hidden costs to ask about before you sign
- Setup fees: Ask whether onboarding, data mapping, or account buildout costs extra.
- Legacy A/R fees: Some vendors bill separately for old balances and denied claim recovery.
- Software charges: Confirm whether you need new clearinghouse tools, PM modules, or licenses.
- Termination terms: Early exit penalties often trap practices in poor-performing relationships.
Cheap billing is expensive if it increases write-offs, slows collections, or ties up your office manager in constant follow-up.
If you want a clean framework for comparing options, review this breakdown of outsource medical billing cost before you negotiate. It will keep you focused on total financial impact, not headline pricing.
Planning a Smooth Transition to Your New Billing Partner
The first 90 days determine whether a switch improves cash flow or creates temporary chaos. Most transitions fail for simple reasons. Nobody defines ownership, credentialing issues surface late, and old A/R gets ignored while everyone focuses on new claims.
What the first 90 days should look like
Days 1 through 30
Start with data access, payer enrollment review, and workflow mapping. Your new partner should understand how charges are entered, where documentation lives, how providers use CPT and modifier combinations, and where current denials originate.
This is also when you assign responsibility for old balances. If nobody owns unresolved A/R from the prior setup, your practice will miss out on recoverable dollars.
Days 31 through 60
Claims should be moving through the new process, but friction usually emerges at this stage. Provider enrollment mismatches, taxonomy issues, clearinghouse edits, and EHR work queue confusion all tend to surface here.
Use this phase to tighten communication. You need one operating rhythm for unresolved claims, payer escalations, coding questions, and posting discrepancies.
Days 61 through 90
By this stage, you should be reviewing trends, not just activity. Which payers are slowing? Which CPT families are denying? Are charge entry delays improving? Are appeals being resolved or submitted without resolution?
The goal is control. A billing partner earns trust when your reporting becomes clearer and your follow-up becomes more deliberate.
Common transition mistakes
- Unclear ownership of old A/R: New claims get attention. Old money gets neglected.
- No dedicated contact: Problems bounce between teams and never get solved.
- Credentialing assumptions: Practices often assume payer enrollment is current when it isn't.
- No baseline report: If you don't document starting performance, you won't know whether the switch helped.
Start the relationship by defining who owns data access, payer communication, old A/R, and denial escalation. If those owners aren't named early, the transition drifts.
If you're planning a vendor change, this guide on how to outsource medical billing is a practical starting point. Before any agreement, get a financial audit. You want a baseline for A/R aging, denial categories, coding risk, and recoverable revenue before the new team touches the process.
Frequently Asked Questions From Houston Practice Owners
How do I know if my practice needs a medical billing company in Houston or just a better biller?
If the issue is one employee, replace the employee. If the issue is old A/R, recurring denials, payer-specific failures, lack of reporting, and no one owning follow-up, you need a system change, not a staffing change. Most practices wait too long because they frame a structural RCM problem as a personnel issue.
Will switching billing companies disrupt our EHR and front office?
It shouldn't if the partner can work inside your existing EHR and practice management workflow. That's one of the first questions to ask during vetting. Forced migrations create avoidable disruption. A competent partner adapts to your operating environment and gives your staff clear handoff rules for charges, documentation, and denial support.
Should I choose a local Houston vendor or a national one?
Choose the team that protects revenue, communicates clearly, and understands your specialty. Local presence can help, especially if your physicians want tighter communication and regional familiarity. National scale can help if the team is operationally mature. Location matters less than accountability, specialty fluency, and financial performance.
How quickly should I expect financial improvement after outsourcing?
You should expect early visibility before you expect full optimization. First, reporting should get sharper. Then unresolved claims should get cleaner ownership. Then cash flow should improve as denials, edits, and old A/R are addressed. The exact timeline depends on credentialing status, claim backlog, payer mix, and how damaged the existing process is, but a good partner should give you a concrete transition plan instead of vague promises.
If your practice is evaluating a medical billing company in Houston, start with numbers, not sales language. Happy Billing helps independent practices reduce leakage, tighten denial management, and improve A/R velocity without forcing an EHR migration. If you want to see where cash is getting stuck before making a change, request a free revenue cycle audit and review the findings against your current billing performance.