Medical Billing Services Pittsburgh: Boost Revenue 2026
Monday starts with a familiar problem in Pittsburgh. Your schedule is full, charges are getting entered, but cash is still arriving too slowly because claims with UPMC and Highmark need rework, follow-up, or corrected documentation before they pay cleanly.
That is why choosing medical billing services in Pittsburgh is a revenue decision, not a staffing decision. In this market, billing performance depends on how well the team handles local payer rules, specialty-specific documentation, and disciplined follow-up that keeps A/R from aging out and protects net collections.
I see the same pattern across independent primary care groups in the South Hills, orthopedic practices near Cranberry, behavioral health clinics serving Allegheny County, and hospital-adjacent specialists trying to keep overhead under control. The pressure looks different by specialty, but the financial outcome is the same. Denials rise, old balances sit longer, and your front office ends up doing work that should have been resolved before the claim ever left the practice.
If your receivables are drifting past a healthy range, the issue is rarely one bad employee or one difficult payer. It is usually a billing model that does not match your Pittsburgh payer mix or your specialty's documentation demands. For a broader view of how these pressures affect practices statewide, see our guide to medical billing services in Pennsylvania.
Local knowledge changes the math. A billing team that understands how Pittsburgh claims move from charge entry to payment puts more money in the bank faster, with fewer preventable denials and less staff time lost to payer follow-up.
Why Pittsburgh Medical Billing Demands Local Expertise
Monday starts with a full schedule in Oakland or the South Hills, but the billing friction usually shows up before lunch. A UPMC claim stalls over documentation detail. A Highmark follow-up sits in queue longer than your staff expected. By the end of the day, charges are posted, work was done, and cash still feels one cycle behind.
That pattern is common in Pittsburgh because the local payer mix creates problems that generic billing teams do not catch early enough. UPMC and Highmark are not interchangeable from an RCM standpoint. Their edits, authorization expectations, portal workflows, and appeal habits shape how fast claims move, which denials repeat, and how much staff time gets pulled into rework. For a practice owner, that shows up in three places fast. A/R stretches, denial rate creeps up, and net collections soften even when patient volume stays stable.
Generic billing breaks down when local payer rules drive the outcome
A vendor can be competent on paper and still perform poorly in this market.
I see it with independent primary care, ortho, cardiology, behavioral health, and hospital-adjacent specialty groups across Allegheny County. The workflow looks fine at a distance. Charges drop, claims scrub, denials get touched. But if the team does not understand which UPMC edits hit your specialty most often, or how Highmark tends to respond to certain documentation gaps, they spend their time reacting after the claim is already delayed.
That is expensive.
An orthopedic group near Cranberry has different failure points than a behavioral health clinic in the city. Ortho may struggle with authorization linkage, modifier use, and surgical documentation that supports the billed level of service. Behavioral health often feels the pain in eligibility, session documentation, and follow-up discipline on smaller balances that age unaddressed. The specialties differ, but the financial result is the same. Slow payments, preventable denials, and more dollars pushed into older buckets where recovery rates drop.
Local expertise shows up in the work, not in the sales pitch
A strong Pittsburgh billing partner should be able to explain payer behavior by specialty and tie that behavior to your revenue results. If they cannot tell you why UPMC denials differ from Highmark denials for your practice, they are processing claims, not managing receivables.
The practical questions are straightforward:
- Which payer is causing the most avoidable rework?
- Which denial categories are rising by specialty?
- How quickly are underpaid or pended claims being touched?
- Which front-end mistakes are creating back-end A/R drag?
Those answers matter more than generic promises about service quality because Pittsburgh reimbursement pressure is local and operational. A cardiology practice dealing with referrals, testing, and procedure coding needs a different billing approach than a pediatric office fighting eligibility issues and vaccine administration complexity. The right team sees those differences early and fixes the workflow before cash slows down.
For a broader state-level view, this guide to medical billing services in Pennsylvania provides useful context, but Pittsburgh requires a closer read on payer behavior than most markets.
Documentation also plays a bigger role than many owners expect. If your providers are trying to speed charting with speech tools, the upside is real only when the billing process catches documentation issues before submission. This 2026 medical voice recognition guide is a useful reference for practices reviewing how documentation workflows affect downstream claim quality.
The core point is simple. In Pittsburgh, billing performance depends on whether the team understands how local claims get paid, delayed, denied, and appealed. That knowledge protects A/R days, keeps denial rates from becoming a staffing problem, and helps net collections reflect the work your clinicians already did.
The True Cost of Your In-House Billing Department
A Pittsburgh practice can feel fully staffed and still bleed cash. I see it when a two-physician orthopedic group has one biller covering charge entry, payment posting, patient balance calls, and UPMC follow-up, while the front desk is also trying to sort authorizations and referral issues. Payroll looks controlled on paper. A/R slows down, denial rework piles up, and net collections slip for reasons that never show up on the salary line.
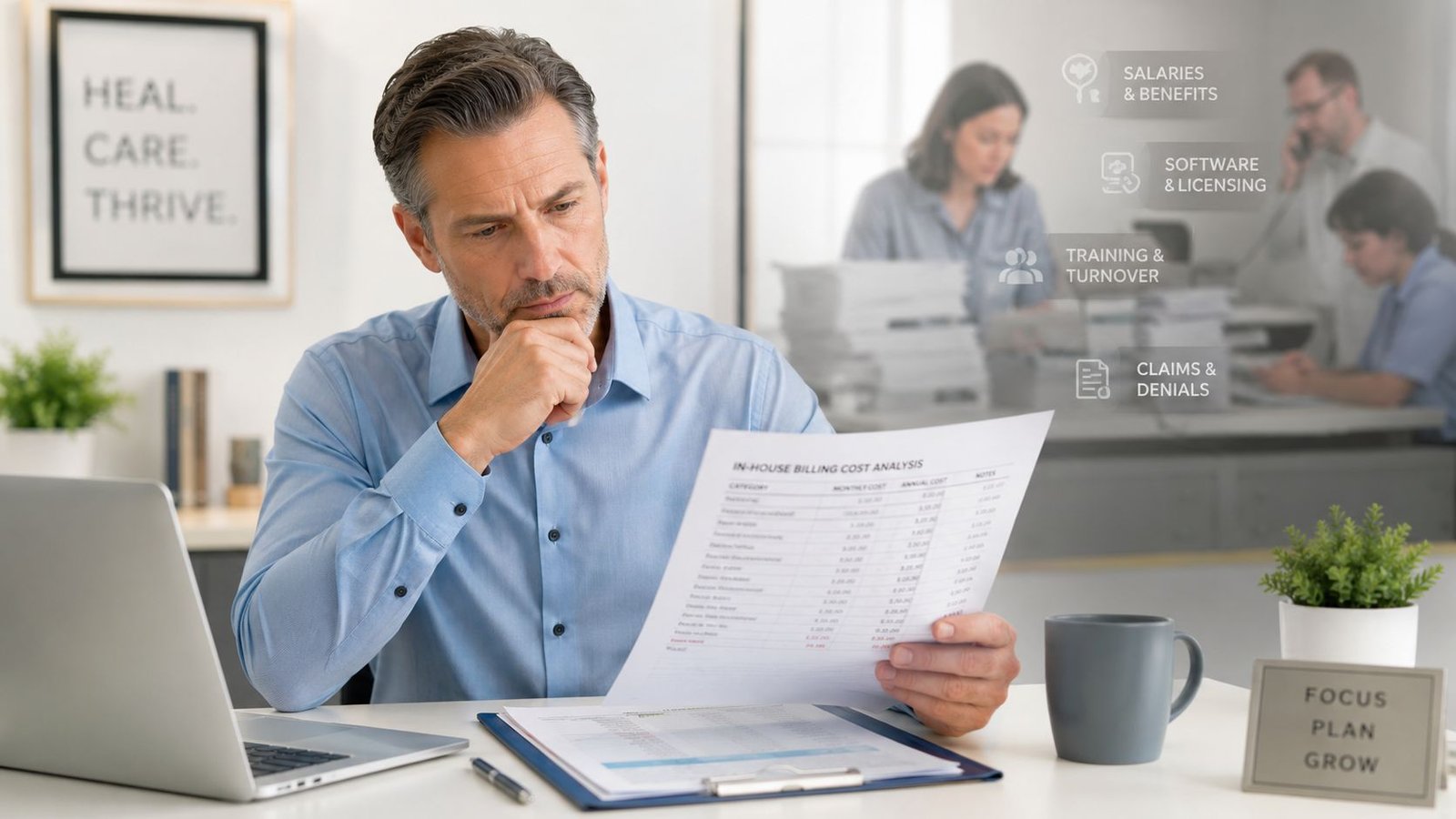
That is the actual cost of in-house billing. It includes wages, but it also includes delayed claims, underworked denials, inconsistent follow-up, and the lost production that comes from billing staff being spread across too many jobs. In Pittsburgh, that pressure shows up fast because payer rules are not generic. UPMC and Highmark each create their own follow-up burden, and specialty groups feel it differently.
Your cost of collections includes hidden operating drag
Owners usually start with salary and benefits. That is only the first layer.
A more accurate review includes manager oversight, PTO coverage, recruiting, onboarding, clearinghouse fees, coding resources, claim edits, software training, and the time it takes to fix preventable errors. If one experienced biller leaves, the replacement cost is not just recruiting. It is the 60 to 90 days of weaker claim submission, slower appeals, and less disciplined A/R work while the new person learns your physicians, your EHR, and your payer mix.
Specialty complexity raises that cost. A behavioral health practice in Pittsburgh may struggle with authorization tracking and coordination of benefits. A cardiology group may lose money on testing, procedures, and modifier-related denials if the billing team is too generalist. A surgical office can post charges on time and still miss revenue if no one is checking whether documentation supports the code set that was submitted.
Documentation technology can help, but only if the billing handoff is tight. If your providers are testing ambient charting or faster dictation, the 2026 medical voice recognition guide is useful background. Faster notes do not help net collections if charge capture gets looser or if missing details create avoidable denials.
Slow A/R creates financing pressure inside the practice
Once claims age past your normal payment window, the practice starts carrying the receivable instead of collecting it. That affects payroll timing, physician draws, hiring plans, and supply purchasing. It also creates more manual work because older accounts take more touches to resolve.
In-house teams feel this first in their daily queue. Staff spend the morning answering patient calls, the afternoon fixing registration mistakes, and the rest of the day reacting to payer correspondence. Very little time remains for root-cause work. Denials tied to authorization gaps, referral errors, modifier usage, or local payer edits keep coming back because nobody owns the pattern.
That cycle is common in Pittsburgh offices with heavy UPMC or Highmark volume. A claim issue that should have been prevented at scheduling turns into rework at charge entry, then another delay at payment posting, then more aging in follow-up. The practice pays for the same mistake several times.
Busy billing staff and strong billing performance are not the same thing. What matters is whether the process lowers denial rates, keeps A/R from aging out, and converts charges into cash predictably.
What owners should compare before deciding
A fair comparison between in-house billing and an outside partner should focus on financial control, not preference or habit.
| Question | In-house weakness to watch | Better operating model |
|---|---|---|
| Who owns denial prevention by payer? | Staff fix denials after they hit | Edits, training, and front-end checks reduce repeat denials |
| Who works A/R by payer and aging bucket? | Follow-up happens when time allows | Clear accountability by payer, claim age, and dollar value |
| Can the team handle specialty-specific coding pressure? | One generalist covers every claim type | Specialty-focused billing and coding review |
| How fast can reporting identify a problem? | Month-end summaries arrive after cash already slowed | Weekly visibility into denial trends, lag points, and net collections |
For a more detailed comparison, review this guide to in-house vs outsourced medical billing. The right answer depends on whether your current team can protect cash flow under Pittsburgh payer conditions, keep denial rates under control, and maintain net collections without constant staffing strain.
What a High-Performance RCM Partner Delivers
A real RCM partner doesn't start at claim submission. It starts before the visit, when eligibility, authorization, and documentation decisions still have time to prevent loss.
Effective medical billing in Pittsburgh requires a workflow that spans insurance verification, pre-certification, charge entry, medical coding, claims submission, payment posting, denial management, and A/R follow-up, integrated with the practice's existing EHR, according to this Pittsburgh billing workflow overview. That matters because revenue leakage rarely comes from one dramatic mistake. It usually comes from small breaks between departments.
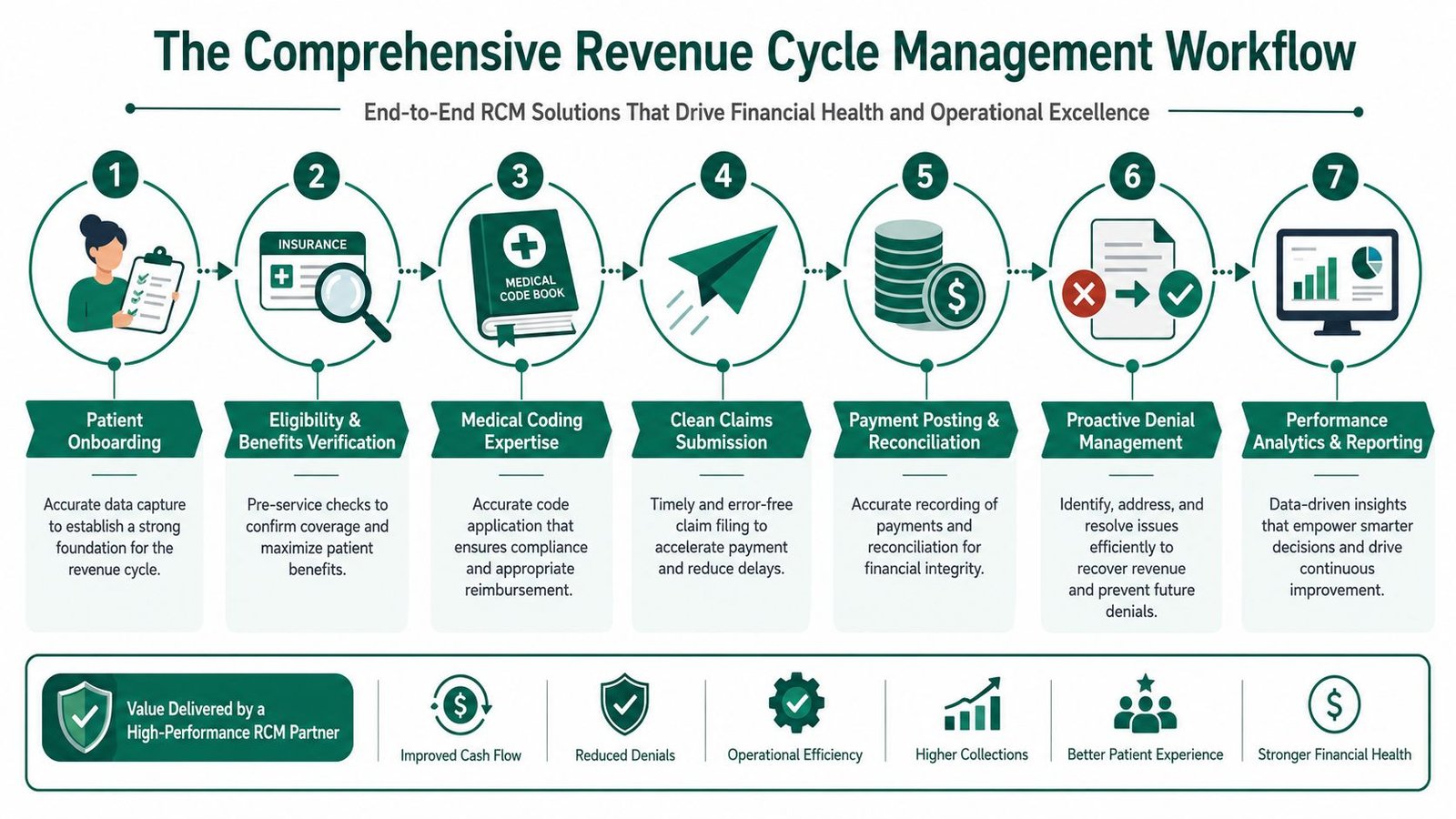
Front-end control determines back-end cash
The strongest billing operations treat intake as a financial control point.
Eligibility and benefits verification
If the plan, product, or coordination of benefits is wrong, the claim is weak before the patient is roomed.Pre-certification and authorization tracking
This is especially important for imaging, procedures, recurring therapy, and behavioral health. Missing or mismatched authorization details create avoidable denials that age badly.Charge capture linked to documentation
The goal isn't just getting a claim out. It's making sure the record supports the CPT, diagnosis linkage, and modifier logic under CMS guidance and payer policy.
Mid-cycle accuracy protects first-pass performance
Most owners hear “coding support” and think code entry. That's too narrow. The operational value is in validating whether the submitted claim will survive payer edits.
A high-performance team checks ICD-10 to CPT linkage, modifier appropriateness, NCCI edit risk, place-of-service accuracy, and whether documentation supports medical necessity. In cardiology, orthopedic procedures, anesthesiology, and mental health, this work directly affects how much rework lands in aging.
Operational insight: Fast claim submission helps, but clean claim submission matters more. Speed without accuracy just moves denials earlier.
Back-end discipline is where revenue is recovered or lost
Once the payer responds, the billing partner should be doing more than posting ERA files and waiting.
- Payment posting and reconciliation: Variances need review, not just posting.
- Denial management: Appeals should follow a repeatable workflow with documentation support.
- A/R follow-up: Aging should be segmented by payer, balance class, and denial reason.
- Reporting: Owners need visibility into trends that change financial decisions, not generic dashboards.
For practices evaluating what modern oversight should look like, this guide to revenue cycle management benefits is a useful benchmark. The takeaway is simple: filing claims is clerical work. Managing the full financial lifecycle is what improves A/R days and collections.
Navigating Pittsburgh Payer and Specialty Challenges
Pittsburgh isn't hard because billing is hard everywhere. It's hard because local payer rules and specialty complexity stack on top of each other. A generic billing team may know CPT and ICD-10 at a broad level. That still won't protect revenue when UPMC, Highmark, and regional plan behavior intersect with advanced procedures, prior authorization requirements, and documentation-sensitive claims.
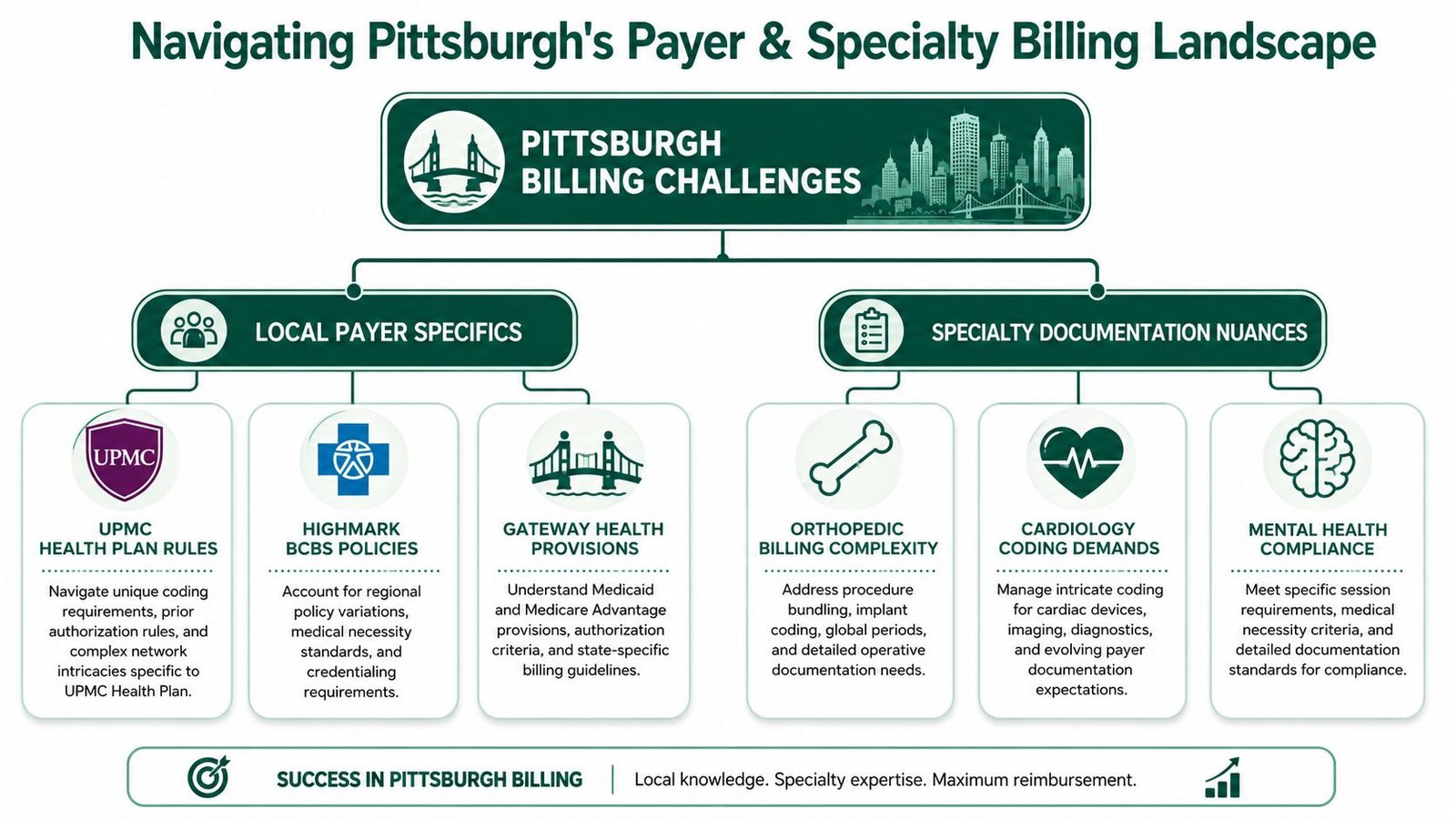
Cardiology is where generic billing breaks fast
Cardiology is one of the clearest examples. Pittsburgh cardiology billing requires precise CPT and ICD-10 pairings, especially for services such as echocardiograms and electrophysiology studies, and successful local cardiology billing firms commonly charge 4% to 10% of collections depending on complexity and volume, according to this Pittsburgh cardiology billing analysis.
For an owner, the coding detail matters because it ties directly to cash:
- Echocardiogram claims: If the diagnosis doesn't support medical necessity for the CPT billed, payment stalls and staff must rework what should have been a clean submission.
- Electrophysiology services: Documentation gaps around the procedure, device work, or modifier use can trigger denials that are expensive to appeal.
- Interventional cardiology: Bundling review and modifier logic matter. If a team applies modifier 59 casually, the payer may reject or downcode based on edit logic rather than your clinical intent.
That's why a cardiology group should expect more than “we know cardiology.” A competent partner should be comfortable discussing CPT family logic, diagnosis linkage, modifier use, and how those choices affect denial risk. If you want a specialty-specific benchmark, review these cardiology billing services standards and compare them against your current reporting.
Orthopedics, anesthesia, and mental health have different failure points
Orthopedic claims often fail on bundling, global period confusion, implant-related support, and modifier misuse. In practical terms, owners lose revenue when the billing team can't defend separate services with the documentation the payer expects.
Anesthesiology creates a different problem set. Base units are only part of the story. Time reporting, medical direction or supervision documentation, and anesthesia modifier handling affect whether the claim pays correctly. A generalist team may submit these claims, but submission alone doesn't mean the reimbursement is right.
Mental health has its own revenue trap. Authorization management, recurring visit rules, and documentation consistency can create aging if the team doesn't track limits and payer-specific utilization requirements before the claim goes out.
The strongest specialty billing teams don't memorize codes. They understand where each specialty actually loses money.
Local payer operations require compliance discipline too
Pittsburgh practice owners also need to think beyond coding. Security, workflow controls, audit trails, and payer-facing documentation processes matter when PHI moves across systems and outside vendors. For groups reviewing their broader operational safeguards, this resource on managing IT compliance for Western PA businesses is worth reading alongside your billing evaluation.
One more practical point: timely filing discipline still matters even when the denial itself gets most of the attention. A claim can be clinically valid and still become unrecoverable if the office misses filing or appeal windows. This reference on UnitedHealthcare timely filing limits is a reminder of how fast administrative misses turn into write-offs.
Critical Questions to Ask Any Billing Service
A Pittsburgh practice usually learns the truth about a billing vendor after the first hard month. UPMC starts dragging on a documentation request, Highmark pushes a medical necessity denial into appeal, your front desk is asking who owns the auth gap, and A/R over 90 days starts climbing. That is the moment to find out whether the billing company knows this market or only knows how to send claims.
A good interview process should get past sales language fast. Ask questions that tie directly to three outcomes: lower denial rates, fewer days in A/R, and stronger net collections. If a vendor cannot answer with examples from practices like yours, you are still hearing a pitch.
Ask for proof tied to your specialty and your payer mix
Generic reporting is not enough in this city. A behavioral health group dealing with recurring authorizations needs different controls than an orthopedic practice fighting modifier edits and post-op visit confusion. A cardiology group with heavy UPMC volume has different follow-up pressure than an ASC trying to keep Highmark payments from aging.
Use direct questions:
Show me reporting for a practice in my specialty.
Ask to see payer aging, denial categories, first-pass claim trends, and follow-up activity. The report should help your practice manager spot where cash is slowing down.How do you handle claims that are technically billable but risky to submit?
Ask what happens when documentation is incomplete, a modifier decision is unclear, or an authorization is missing. You need to know whether they hold the claim, escalate to the practice, or send it and risk a denial.What does your denial workflow look like after the first rejection?
Ask who touches the account, how root cause is documented, and when the issue gets pushed back to scheduling, registration, or the provider.
Ask how they handle Pittsburgh payer friction
Local knowledge's impact becomes evident in the numbers. A vendor that works nationally but does not understand UPMC and Highmark behavior can look organized while your A/R gets older.
Ask them:
| Question | Why it matters |
|---|---|
| How do you separate UPMC issues from Highmark issues in reporting? | Payer-specific aging tells you where cash is stalling and where appeals need attention |
| What is your process for tracking payer follow-up by bucket and by representative action? | A/R improves when follow-up is disciplined, documented, and timed correctly |
| How do you manage authorization and referral failures before claim submission? | Front-end misses become denials, rework, and lower net collections |
| What do you change in the first 30 days if registration errors are driving denials? | You want operational fixes, not just claim resubmission |
A billing company should also be able to explain one difficult local denial from intake through payment. For example, if you run anesthesia, ask about modifier handling and documentation review. If you own a mental health practice, ask how they track visit limits and authorization renewals before balances age out.
If the vendor cannot explain how they reduce rework for your specialty and payer mix, they are unlikely to improve cash flow in a measurable way.
Ask for operating discipline, not reassurance
The right questions expose whether the company manages revenue cycle work in a controlled way or reacts after claims fail.
Ask these four:
- What performance thresholds trigger internal escalation on A/R or denials?
- How do you tell the difference between a payer pattern and a practice workflow problem?
- How do you report root causes to our office manager and physicians?
- What front-desk or documentation changes would you recommend in month one?
These answers matter because the trade-off is real. Some vendors are strong at posting and follow-up but weak at fixing front-end breakdowns. Others know coding but do not communicate clearly enough for your team to correct the source of denials. The best partner does both.
If you want a sharper interview guide, review this checklist of questions to ask a medical billing company before hiring.
How Our RCM Model Solves These Core Problems
The right RCM model should solve the exact problems that push a Pittsburgh practice into slow cash and high rework. That means fewer preventable denials, tighter control of front-end errors, and faster movement from charge entry to payment without forcing the practice into a new system.
The benchmark matters here. The industry standard for claim denial rate is 2% to 3% of net patient revenue, and anything above 5% signals a malfunctioning revenue cycle that creates lost revenue, manual rework, and slower cash flow, according to this RCM KPI benchmark. That's the threshold we use when we assess whether a billing operation is merely busy or effectively performing.
Built for prevention, not cleanup
We've seen that practices don't need another vendor who waits for denials and then starts chasing. They need a model that catches problems upstream.
That's why our approach combines agentic AI with expert human auditors. The AI layer helps identify recurring denial patterns, charge issues, and workflow bottlenecks quickly. Our U.S.-based audit oversight provides the judgment call where payer nuance, specialty documentation, and claim context matter most.
The goal isn't automation for its own sake. It's protecting net collections by reducing the amount of preventable rework entering A/R.
Designed for specialty complexity and local payer friction
In our experience, specialty claims fail for predictable reasons. Cardiology loses money on diagnosis linkage and procedure edits. Anesthesia struggles when unit logic and modifier handling aren't audited carefully. Behavioral health gets hit by authorization drift. Orthopedics runs into bundling and global period confusion.
We've built our workflows around those realities. Claims move inside the existing EHR, so the practice doesn't have to absorb a migration, retrain everyone, or create parallel systems. That matters because disruption at implementation often creates the very billing lag owners are trying to escape.
What works: in-EHR workflows, payer-specific edits, and active denial prevention.
What doesn't: batch processing, weak specialty review, and waiting until month-end to discover a pattern.
Focused on speed that improves cash
We've seen the biggest operational gains come from velocity. Claims can't sit untouched. Follow-up can't depend on whoever has time. Reporting can't be a static month-end summary.
Our model is built around continuous claim movement, around-the-clock operational coverage, and proactive review of issues before they become aged receivables. The result is simple for the practice owner: less time chasing claims, clearer visibility into why cash is slowing, and an RCM process aimed at keeping denial performance well below the threshold that signals trouble.
FAQs From Pittsburgh Practice Owners
Should I outsource billing if my internal team is loyal and experienced
Keep the team if they are protecting cash. Change the model if they are not.
In Pittsburgh, I see this with established internal billers who know the practice well but still get buried by UPMC follow-up delays, Highmark policy quirks, specialty-specific edits, and patient balance pressure. Loyalty matters. So do results. If A/R is aging past your target, denial rates stay stubborn, or net collections are sliding, the problem is not effort. It is capacity, process, or payer expertise.
How do I know whether my billing problem is front-end or back-end
Start with where claims fail.
If rejections and denials center on eligibility, authorization, registration errors, or diagnosis mismatches, the front end is creating rework before the claim has a fair chance to pay. If claims leave clean but sit too long with UPMC, get underpaid by Highmark, or stall in secondary follow-up, the back end is the drain on cash. The pattern will show up in payer aging, denial categories, and how long claims sit untouched after first submission.
Will switching billing services disrupt my practice operations
It can. The risk is highest when the billing company forces a platform change, weakens communication with the front desk, or treats implementation like an IT project instead of a cash preservation project.
The smoother transitions usually happen when the partner works inside the current EHR, maps payer workflows before go-live, and sets clear rules for charge entry, coding review, denial ownership, and patient balance handling. For a Pittsburgh practice dealing with dominant local payers, that matters because even a short billing slowdown can push A/R days up fast.
What should I expect from reporting each month
You should be able to spot what is hurting cash without waiting for a quarterly review.
That means reports tied to action. Payer-specific A/R aging. Denial trends by root cause. Claims sitting in work queues too long. Underpayments that are not being appealed. Net collections viewed alongside scheduling, authorization, and charge lag, so you can tell whether the leak starts at the front desk, in coding, or in payer follow-up.
If a report cannot help you reduce A/R days or denial volume, it is an accounting summary, not revenue cycle management.
If your practice is deciding whether to keep patching an uneven billing process or move to a model with tighter accountability, Happy Billing is built for that decision. We focus on the payer behavior Pittsburgh practices deal with every day, especially UPMC and Highmark, and we do the work inside your current systems so operations stay stable while collections improve. The goal is straightforward. Lower denial rates, faster claim resolution, and stronger net collections without adding more administrative weight to your office.