Mastering United Healthcare Timely Filing Limits in 2026

For most in-network providers, UnitedHealthcare’s standard timely filing limit is 90 days from the date of service, a deadline that requires strict adherence to avoid automatic denials. The actual deadline, however, is not a single rule but a complex matrix dependent on the patient’s plan, your network status, and state-specific mandates. Misinterpreting these variables is a primary source of lost revenue for medical practices.
Understanding United Healthcare Timely Filing Limits
The 90-day timely filing deadline is the baseline for most in-network, commercial claims with UnitedHealthcare. According to UHC's own administrative guide, failure to submit a claim within this window typically results in a denial for which the member cannot be billed. Overturning this denial requires irrefutable proof of timely submission.
Key Variations to the Standard Rule
A billing team's effectiveness hinges on its ability to navigate the exceptions to the standard 90-day rule. These variations directly impact cash flow and are governed by specific payer policies.
- Out-of-Network Providers: Non-contracted providers are generally granted a 180-day window from the date of service.
- Secondary Payer Claims: When UHC is the secondary insurer, the 90-day clock begins on the processing date printed on the primary payer's Explanation of Benefits (EOB), not the date of service.
- State-Specific Mandates: State laws can override UHC’s corporate policy. For instance, if a state mandates a 180-day filing window for all commercial plans, UHC must comply for plans governed by that state's legislation.
For example, a routine office visit billed with CPT code 99214 for a patient with a standard UHC Choice Plus PPO plan is subject to the 90-day rule. However, if Medicare was the primary payer for that same visit, the 90-day filing period for UHC begins on the date of Medicare's EOB. Submitting based on the original date of service would be a critical error.
Critical Insight: The most frequent timely filing errors occur from misidentifying the "start date." For secondary claims, the primary payer's EOB date is Day 1. According to AAPC standards, failure to track this date is a leading cause of preventable denials.
Here is a quick reference table for UHC’s standard deadlines. Always verify these against your specific provider agreement and prevailing state laws.
UHC Timely Filing Deadlines at a Glance
| Claim Type / Provider Status | Standard Timely Filing Limit (from Date of Service) |
|---|---|
| In-Network Provider | 90 days |
| Out-of-Network Provider | 180 days |
| Secondary Payer (In-Network) | 90 days from the primary payer's EOB date |
| Secondary Payer (Out-of-Network) | 180 days from the primary payer's EOB date |
Mastering these deadlines is the first line of defense against administrative denials. A solid grasp of these rules is step one, but ensuring every field on the standard medical claim form is accurate is equally critical to protecting cash flow and optimizing RCM team efficiency.
How Filing Deadlines Differ Across UHC Plans
Treating all UnitedHealthcare timely filing limits as a single rule is a direct path to denials. The actual deadline is dictated by the specific insurance product, and failure to differentiate between them guarantees lost revenue.
UHC's commercial plans, such as Choice Plus PPO, generally adhere to the 90-day limit for in-network providers. The complexity arises with government-sponsored plans administered by UHC.
The Impact of Plan Type on Filing Rules
UnitedHealthcare Medicare Advantage (MA) plans, while often mirroring the 90-day commercial rule, are ultimately governed by CMS directives. When CMS issues guidance, such as extending filing windows during a public health emergency, UHC's MA plans must comply.
UHC Community Plans (Medicaid) present the most significant variation. These plans must conform to individual state Medicaid agency regulations. For instance, the timely filing limit for a UHC Community Plan in Texas is 95 days, while in Florida, it might be a full year. Your RCM team must operate based on local state Medicaid rules, which always supersede UHC’s corporate policy for these plans.
The chart below breaks down the most fundamental difference in filing deadlines.
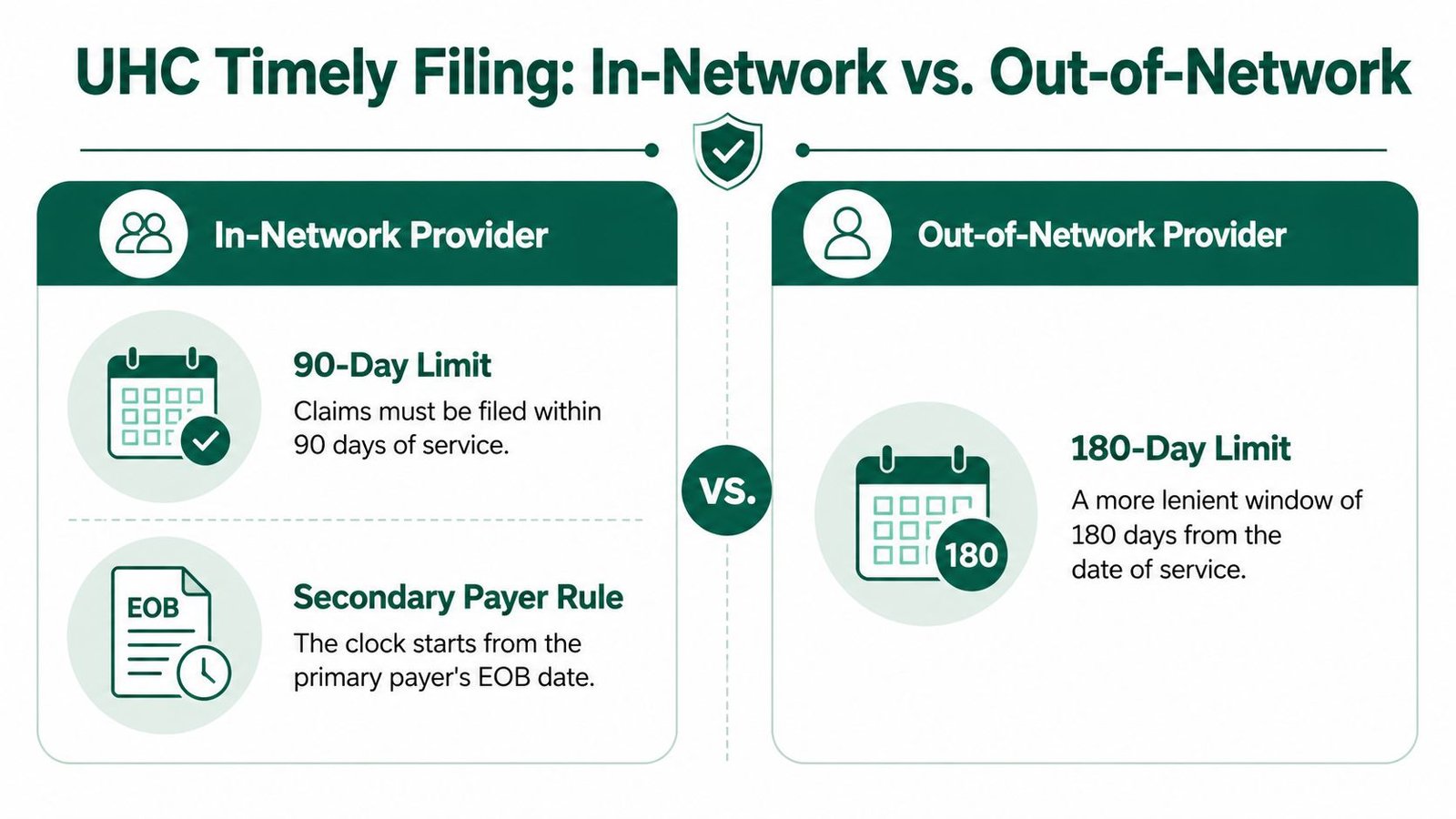
As you can see, simply being out-of-network grants a more lenient 180-day window. Verifying network status before claim submission is non-negotiable.
Navigating Secondary Payer Timelines
When UHC is not the primary insurer, the timely filing clock does not start on the date of service. This critical distinction is a frequent source of error for billing teams.
Instead, the countdown begins on the date the primary payer’s Explanation of Benefits (EOB) is issued.
Imagine your practice performs a polysomnography sleep study (CPT 95810) for a patient. Medicare is primary, and UHC is secondary. If the Medicare EOB is dated June 1st, your team has 90 days from June 1st to submit the claim to UHC—not 90 days from the original study date.
Mismanaging this sequence is a costly mistake. For a deeper analysis of these multi-payer scenarios, our guide on coordination of benefits in medical billing is essential reading for any practice handling dual-coverage patients.
When State Law Overrides UHC Policy
UnitedHealthcare’s corporate timely filing limits are a baseline, not the final word. State-level "prompt pay" laws often supersede these internal payer policies, providing a crucial advantage for practices that understand and leverage them. These statutes are designed to protect provider revenue from arbitrary corporate deadlines.
A clear example is Texas, where state mandates provide providers with more time than UHC’s standard 90-day rule. Our guide on medical billing outsourcing in Texas details these regional requirements.
Citing State Law in Appeals
When a claim is denied for timely filing, the most effective appeal is not a request for an exception but a direct citation of the governing law. If UHC denies a claim submitted on day 92 but state law mandates a 120-day filing window, the denial is invalid.
Your appeal letter must reference the specific statute that overrules UHC’s policy. For example: "This claim was submitted within the 95-day timeframe mandated by Texas Insurance Code Sec. 1301.102 for electronically submitted claims. Therefore, this timely filing denial (denial code CO-29) is incorrect and requires reprocessing."
Expert Takeaway: An appeal grounded in state law is a statement of compliance, not a request. UHC is legally obligated to adhere to state regulations, making this approach far more powerful than pleading for reconsideration.
Maintaining an accessible, updated list of your state's filing mandates is a non-negotiable best practice for any RCM team. This information is the difference between writing off a valid claim and collecting earned revenue. This proactive knowledge transforms a billing department into a strategic unit armed to defend the practice’s financial health against improper denials based on United Healthcare timely filing limits.
How to Fight and Win a Timely Filing Denial
A timely filing denial from UnitedHealthcare is frustrating but often winnable with a formal appeal backed by irrefutable proof. Resubmitting the claim without a formal appeal is futile.
Your first action is to secure evidence of timely submission. For electronic claims, this means retrieving the acceptance report from your clearinghouse, specifically a 277CA (Claim Acknowledgement) or 999 (Implementation Acknowledgement) file. This digital timestamp is the most powerful evidence of when UHC’s system received the claim. For direct submissions via the UHC Provider Portal, a screenshot of the submission confirmation screen is mandatory.
Building Your Appeal Package
With proof in hand, construct an appeal that is impossible to dismiss.
- Draft a Formal Appeal Letter: Be concise and professional. Reference the claim number, patient details, and date of service. State clearly that you are appealing a denial for timely filing (e.g., CO-29) and that the claim was submitted within the required timeframe.
- Attach All Your Evidence: The appeal must include the letter, a copy of the original claim (CMS-1500 or UB-04), your clearinghouse acceptance report or portal screenshot, and the EOB showing the denial.
- Cite the Specific Rule or Circumstance: If a special rule applies, state it directly. For example, if appealing a denial for initial newborn hospital care (CPT 99460), reference UHC's policy allowing 180 days for newborn claims. If UHC was secondary, include the primary payer’s EOB to prove the filing clock was reset.

Submitting and Tracking the Appeal
Submit the complete package through the UHC provider portal according to their guidelines. Always save a digital copy of the submission confirmation. Diligently track the appeal's status through the portal until resolution.
A winning appeal proves either that the claim was filed on time and mishandled by the payer, or that an overriding policy (e.g., state law, secondary payer rule) applies. Without solid documentation, your appeal has virtually no chance of success.
The entire process demands meticulous attention to detail. For practices looking to enhance their appeals process, you can learn more about how to appeal a denied insurance claim in our complete guide. A successful appeal recovers revenue and reinforces the value of disciplined RCM workflows.
Stop Chasing Deadlines: How to Crush Timely Filing Denials
The best-run practices make timely filing deadlines irrelevant by building workflows with so much buffer that a denial is a rare anomaly. Proactive prevention is always more profitable than reactive appeals.
A core principle is the 5-day submission rule: every claim is filed within five business days of service. This discipline creates weeks of cushion before UHC's 90-day clock becomes a factor.
Daily Diligence Is Non-Negotiable
Clearinghouse rejection reports must be monitored daily. A claim rejected by the clearinghouse has not been "filed" with the payer, meaning the timely filing clock continues to tick while the claim awaits a simple fix. These rejections for basic data errors—a misspelled name, a mismatched date of birth—must be corrected and resubmitted within hours, not days.
Front-End Work Prevents Back-End Fires
For specialties reliant on prior authorizations, such as cardiology or orthopedics, the work begins long before the patient encounter. For a knee arthroscopy (CPT 29881) with modifier 59 (Distinct Procedural Service) if performed with another procedure, the authorization must be approved and documented before the service. Failure to do so creates avoidable delays that erode the filing window.
The battle against timely filing denials isn't won on day 89; it's won or lost on the front end. A delay in securing an authorization or a failure to fix a clearinghouse rejection is where most revenue is lost.
Don’t Get Tripped Up by UHC’s Rules
UnitedHealthcare’s deadlines are a complex matrix that varies by network status, claim type, and patient plan.
- In-Network: You have 90 days from the date of service.
- Out-of-Network: The window is a more forgiving 180 days.
- Newborn Claims: These get a special 180-day window.
- Secondary Claims: The 90-day clock starts from the primary EOB date.
- Corrected Claims: You get a full 365 days from the original processing date.
Knowing these rules is one thing; embedding them into your workflow is what matters. You can see just how complex this gets by reviewing the complete breakdown of insurance claim filing limits on cloudrcmsolutions.com.
An expert RCM partner like Happy Billing embeds these rules directly into your workflow, using technology and specialized oversight to ensure claims are submitted cleanly long before united healthcare timely filing limits become a concern.
The image below shows how a dedicated partner organizes services by specialty to address these unique workflow needs.
This level of specialization means that whether it’s managing prior authorizations for mental health or navigating global periods in orthopedics, the billing process is optimized from day one. At Happy Billing, we design workflows tailored to the specific headaches your practice faces—especially from complex payers like UHC. By mastering these nuances, we help you move beyond just avoiding denials to actually accelerating your revenue.
How an RCM Partner Protects Your Revenue
For high-volume practices in demanding specialties like anesthesiology or cardiology, merely meeting the 90-day deadline is a sign of a strained revenue cycle. The objective is not to meet deadlines but to submit clean claims within days of service.
A dedicated RCM partner achieves this by integrating expert oversight and technology into your existing EHR. This system acts as a safety net, automatically flagging unbilled encounters and prioritizing claims by value and urgency, shrinking the claim lifecycle from weeks to days.
Specialized Workflows for Complex Billing
A true expert partner builds workflows designed for your specialty's unique challenges.
For mental health practices, a frequent bottleneck is managing authorizations for ongoing care. A specialized workflow ensures that authorizations for services like psychotherapy sessions (CPT 90837) are secured and verified before submission. This eliminates a chokepoint that risks exceeding United Healthcare timely filing limits.
Similarly, for high-dollar cardiology procedures, a front-end audit of clinical documentation ensures coding is accurate and fully supports medical necessity, preventing time-consuming payer disputes that jeopardize timely filing.
By performing compliance and documentation work on the front end, an RCM partner doesn’t just prevent timely filing denials—they accelerate cash flow. The objective shifts from meeting deadlines to maximizing financial velocity.
This proactive management is the core of a strong RCM strategy. To see how this applies on a broader scale, get a deeper look at the benefits of outsourced revenue cycle management in our guide. By embedding these expert processes, a partner transforms your billing from a reactive chore into a strategic asset that fortifies your bottom line.
H3: What is the timely filing limit for a UHC corrected claim?
UnitedHealthcare allows 365 days from the date of the original EOB or ERA to submit a corrected claim. This window is exclusively for fixing errors on a claim UHC has already processed, such as an incorrect modifier or diagnosis code. To prevent the claim from being denied as a duplicate, you must use the appropriate resubmission code. On a CMS-1500 form, this means placing frequency code '7' (Replacement of Prior Claim) in Box 22.
H3: Does a clearinghouse rejection impact my filing deadline?
Yes, a clearinghouse rejection critically impacts your filing deadline. A rejected claim has not been received by UHC, and the timely filing clock continues to run. These front-end rejections for simple data errors can become fatal if not addressed daily. If a claim is rejected on day 89 and not fixed and resubmitted until day 91, UHC will issue a timely filing denial (CO-29), as they never received the initial submission. Daily monitoring of clearinghouse rejection reports is non-negotiable.
H3: How do I prove my claim was filed on time?
Your definitive proof is the Payer Acknowledgement Report from your clearinghouse, often a 277CA or 999 file. This is your digital receipt directly from UHC, confirming the exact date and time they accepted the claim file. When appealing a timely filing denial, this document is your most critical evidence. Without this electronic proof, it becomes your word against the payer's—a dispute you will almost certainly lose. If you file via a payer portal, a screenshot of the submission confirmation screen is your only defense.
H3: What is the UHC timely filing limit for DME?
For Durable Medical Equipment (DME), the timely filing limit typically follows the standard 90 days for in-network providers and 180 days for out-of-network providers, starting from the date of service. However, this is heavily dependent on the patient's specific plan (Commercial, Medicare Advantage, or Medicaid). For example, a claim for a Continuous Positive Airway Pressure (CPAP) device, coded E0601, must be submitted within 90 days for a commercial plan member but may be subject to different rules under a UHC Medicare Advantage plan, which follows CMS guidelines. For any practice providing DME, a visit to our page on multiple specialties can provide insight into managing these complex, specialty-specific billing rules.