Mastering Coordination of Benefits in Medical Billing
A COB denial usually means your claim hit the wrong payer sequence, not that the service was coded incorrectly. If your team is staring at messages like “payment adjusted because this care may be covered by another payer,” the fix is operational: identify the correct payer order, transmit the right COB data, and resubmit with clean adjudication proof.
Specialty practices feel this faster than most. Anesthesia claims with modifiers like QK, QX, and AA, cardiology claims with procedure-heavy coding, and orthopedic claims tied to global packages such as 27447 can stall quickly when payer order is wrong.
What Is Coordination of Benefits in Medical Billing
An orthopedic practice closes a postop visit tied to 27447. The coding is fine. The note is signed. The claim goes out, then comes back with a payer message that another plan may be primary. An anesthesia group sees the same problem on a case billed with AA or QK/QX, where the payer sequence blocks payment before anyone even reaches the medical necessity or modifier review. In cardiology, the delay often hits higher-dollar procedural claims, where one COB mistake can hold a meaningful chunk of the week’s receivables.
That is coordination of benefits in medical billing. It is the set of rules and workflow steps used to determine which insurer pays first, which pays second, and what documentation has to follow the claim so each payer can adjudicate in the right order.
For a practice, COB is not just an insurance concept. It is a production issue. If registration captures the wrong subscriber, if eligibility is checked against the wrong coverage, or if the secondary claim goes out without the primary EOB data, payment stops. The claim may be coded correctly and still fail for administrative reasons.
That is why COB belongs inside front-end intake, charge review, and claims submission controls. Specialty groups feel the effect faster because their claims often involve larger allowed amounts, more modifiers, or episode-based billing rules. In anesthesia, a payer sequence problem can delay claims that also require careful handling of medical direction modifiers. In orthopedics, COB errors can complicate claims tied to global periods and related follow-up services. In cardiology, they can stall procedure claims long before the team gets to underpayment review.
The financial impact is straightforward. Staff lose time chasing other active coverage, correcting subscriber records, obtaining primary adjudication, and resubmitting in the right order. AR ages while the claim waits. If you want a broader view of how COB fits into intake, claim submission, posting, denials, and collections, this guide to what revenue cycle management means in practice connects the full workflow.
Practical rule: If the payer says another plan may be responsible, treat the claim as a sequencing and data-capture problem first. Review COB setup before you question the CPT, diagnosis, or modifier.
Understanding the Payer Hierarchy in COB
Payer order isn’t guesswork. It follows a hierarchy, and your staff needs a repeatable decision path before the claim ever leaves the practice management system.
Start with the coverage type, not the card order
Front-desk teams often document insurance in the order the patient presents cards. That doesn’t establish primary versus secondary status. The right question is which coverage is primary for the date of service under COB rules.
That means verifying:
- Effective dates: The policy must be active on the service date.
- Subscriber status: Is the patient the subscriber or a dependent?
- Coverage source: Employer group plan, spouse plan, Medicare, Medicaid, or another form of coverage.
- Accident context: Work-related and accident-related claims can trigger different primary payer logic.
If your billers skip those checks, the claim may look complete but still route to the wrong payer.
The hierarchy your team should apply
The most useful working model is a simple order of analysis.
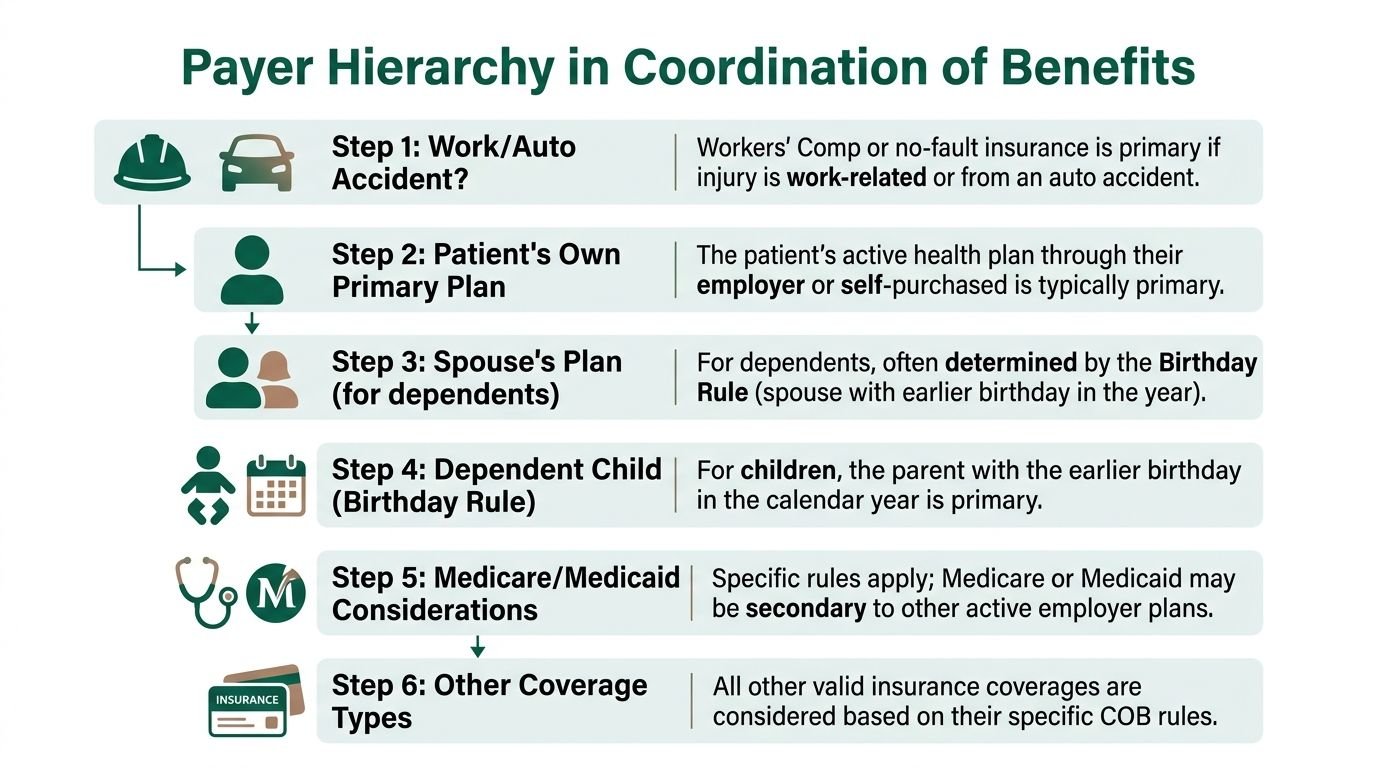
Accident-related coverage comes first in its own lane
If the visit is tied to a work injury or auto claim, your team should identify that before treating the account as standard commercial COB. On procedure-heavy specialties, this matters because high-dollar claims can sit for weeks if the accident indicator is wrong.The patient’s own active employer plan usually outranks dependent coverage
If the patient has active coverage through employment and also appears as a dependent on a spouse’s plan, the active employee plan is commonly primary.Dependent status changes the analysis
For children covered under both parents’ plans, many teams use the birthday rule operationally. The parent whose birthday falls earlier in the calendar year is generally treated as primary unless another legal rule overrides it.Medicare rules are specific, not intuitive
When Medicare coordinates with employer coverage, employer plans with more than 20 employees are primary and Medicare pays secondary. For employers with fewer than 20 employees, Medicare is primary. In Medicare and Medicaid situations, Medicare is always primary and Medicaid is payer of last resort. Practices that miss effective dates, dependent status, or active coverage details can trigger rejection cycles that add 7-14 days to initial adjudication according to this COB payer sequencing explanation.
COB payer sequencing rules
| Scenario | Primary Payer | Secondary Payer | Key Consideration |
|---|---|---|---|
| Patient has active employer coverage and spouse coverage | Usually patient’s own active employer plan | Spouse’s plan | Confirm subscriber vs dependent status |
| Child covered by both parents | Usually parent with earlier birthday in the calendar year | Other parent’s plan | Check for custody or court-order exceptions |
| Medicare with employer group coverage at firm over 20 employees | Employer group health plan | Medicare | Verify current employment status |
| Medicare with employer coverage at firm under 20 employees | Medicare | Employer plan | Don’t assume employer coverage is primary |
| Medicare and Medicaid | Medicare | Medicaid | Medicaid is payer of last resort |
| Commercial primary already paid and secondary is reviewing balance | Commercial primary | Secondary payer | Secondary needs prior adjudication details |
Where specialty billing gets tripped up
The hierarchy sounds straightforward until you apply it to actual claims. An anesthesia claim billed with 01967 plus time units and modifiers QK or QX can deny for payer order before anyone evaluates the medical direction logic. An orthopedic post-op service tied to 27447 may look like a coding issue, but the underlying problem can be that the wrong primary was billed first.
That’s why payer order should be validated before anyone debates modifier logic. The same discipline behind payer sequencing also improves modifier accuracy on difficult claims, especially where status indicators and noncovered logic overlap, as seen in this breakdown of the GY modifier meaning and denial context.
The fastest way to create a repeat denial is to let registration “pick” the primary payer and let billing discover the mistake later.
How to Operationalize COB Data Collection and Claim Submission
COB fails at the front desk long before it fails in the clearinghouse. If intake captures incomplete insurance relationships, billing inherits an account that can’t be submitted correctly.

The intake script that actually surfaces other coverage
Most practices ask, “Do you have secondary insurance?” That question is too narrow, and patients often answer based on what they think should pay, not what is active.
A better script is operational and specific:
- Ask about all active plans: Employer plan, spouse plan, retiree coverage, Medicare, Medicaid, student coverage, and any recent plan change.
- Ask who holds each policy: Subscriber name, relationship, employer, and whether the patient is listed as dependent.
- Ask what changed since the last visit: New job, termination, marriage, divorce, aging off a parent plan, or Medicare enrollment.
- Ask whether another payer should be billed first for this visit: Especially for injuries, surgeries, or hospital-related episodes.
These details need to live in structured fields, not free-text notes. If your PMS stores a second payer but doesn’t carry the subscriber relationship or policy dates cleanly into claim data, the claim file won’t support secondary submission.
The claim file matters more than many teams realize
COB isn’t just a registration concept. It has to be transmitted correctly in the electronic claim format. Under HIPAA, HHS adopted Version 5010 of the ASC X12N 837 standard for coordination of benefits transactions, and these standards define the technical specifications for COB data exchange according to CMS guidance on coordination of benefits transactions.
For professional claims, billers usually need to think about the other payer segments that carry prior payment and subscriber details. In day-to-day operations, that often means making sure:
- Other subscriber information is complete so payer relationship and sequencing are clear.
- Other payer name data is correct so the secondary payer can identify the primary adjudicator.
- Primary adjudication details are preserved including paid amount, adjustments, and patient responsibility.
If the claim has to be manually rebuilt because posting didn’t preserve primary payment data, the process slows down fast.
What works and what doesn’t
What works is a closed-loop workflow between scheduling, registration, eligibility, posting, and secondary billing.
What works
- Re-verify at each major encounter: Surgeries, imaging, hospital rounds, and recurring therapy episodes often expose coverage changes.
- Lock payer sequence before charge release: Don’t let coding finalize and claim scrubbing proceed until payer order is validated.
- Post the primary EOB at line level: Secondary claims depend on exact prior adjudication data.
What doesn’t
- Relying on scanned insurance cards alone: Cards don’t tell you payer order.
- Using free-text registration notes as COB documentation: Billers can’t transmit what the system can’t structure.
- Running older transaction logic: CMS notes that practices using legacy transaction standards risk rejection or rerouting, adding 5-10 business days to secondary payment cycles in the absence of clean COB transmission.
If your team needs a clean operational reference for how payer, subscriber, and claim details should map before submission, this guide to the medical claim form and its practical use in billing workflows helps tie the intake side to the claim side.
Navigating Medicare Secondary Payer Scenarios
Medicare Secondary Payer work is where many practices lose time because staff know the general COB concept but not the CMS-specific workflow. Medicare is not just another payer in the stack. It follows its own sequencing and data-sharing rules.
The BCRC is central to MSP administration
The Benefits Coordination & Recovery Center (BCRC) was established to consolidate other insurance coverage data for Medicare beneficiaries. It shares eligibility and crossover claims with supplemental insurers only when formal agreements exist. That distinction matters because many offices assume secondary transmission is automatic when Medicare pays first or second.
It isn’t always automatic. If no formal crossover arrangement exists, the patient or provider may need to handle secondary coordination manually.
The same operational picture is why prospective coordination tools matter. The CAQH COB registry maintains data on over 225 million members and helps plans coordinate benefits before claims are paid, saving the industry about $1 billion annually according to CAQH’s coordination of benefits overview. For practice managers, the takeaway is practical: better coverage intelligence upstream reduces secondary billing chaos downstream.
MSP scenarios that deserve separate workflows
Treat these as distinct work types inside your billing office.
Group health plan versus Medicare
If the patient has Medicare and active employer group coverage, payer order depends on employer size and employment status. Registration has to capture whether the coverage is tied to current work, not just whether the card is active.
For physician practices, this becomes especially important on recurring cardiology and orthopedic patients where treatment spans multiple dates of service. One wrong assumption at registration can contaminate every claim in the episode.
Liability and accident-related claims
When the encounter is connected to liability, no-fault, or workers’ compensation, MSP rules can shift responsibility away from standard health coverage sequencing. That changes both claim routing and follow-up expectations.
A procedural practice shouldn’t release an operative claim, imaging claim, or interventional claim under routine payer sequencing if the injury context hasn’t been resolved. Otherwise billing teams end up correcting both COB and accident-related responsibility after adjudication fails.
What your team should document before claim submission
A strong MSP workflow usually includes:
- The MSP questionnaire result: Stored in the patient account and tied to the date of service.
- Employer details when applicable: Especially whether coverage is tied to active employment.
- Secondary crossover expectations: Confirm whether a formal agreement exists or manual submission will be needed.
- Supporting account notes for billing staff: Clear enough to prevent duplicate rework.
Medicare COB errors are expensive because they often look administrative at first, then turn into take-backs, rebills, and aged secondary balances later.
When a Medicare-related denial does appear, billers need to separate a true MSP sequencing issue from a standard claim edit or posting issue. This practical reference on the PR 119 denial code and related payer responsibility problems is useful when accounts start mixing responsibility questions with sequencing mistakes.
Specialty-Specific COB Challenges and Solutions
Generic COB guidance usually stops at “bill the primary first, then the secondary.” That advice isn’t enough for high-acuity specialties where payment depends on modifiers, units, global packages, and line-level adjudication.

Existing COB guidance provides no real framework for determining which payer adjudicates modifier-dependent payments first or how a secondary payer should process reduced fees after the primary’s determination. That gap is particularly painful in anesthesiology and cardiology, where billing teams often end up reverse-engineering payer behavior through trial and error, as noted in CareCloud’s discussion of COB gaps in specialty billing.
Anesthesiology claims need payer order before modifier analysis
Anesthesia billing is a good example of why sequence comes first. A claim may include 00840, 01967, or another anesthesia CPT with time units and modifiers such as AA, QK, QX, or QY. If the primary payer adjudicates medical direction differently than the secondary payer, the downstream math changes.
Effective strategies:
- Send the claim to the correct primary first so the secondary sees the first payer’s treatment of units and modifiers.
- Preserve line-level adjudication details because a secondary payer may mirror, reduce, or ignore parts of the primary logic depending on policy.
- Audit concurrency-related documentation before secondary billing if the primary reimbursement reflects modifier-sensitive payment.
What doesn’t work is resubmitting the same anesthesia charge set to a secondary payer without carrying forward the primary adjudication outcome. That creates mismatched expectations and unnecessary denials.
Cardiology claims often combine COB and coding complexity
Cardiology groups deal with procedures where claim value is concentrated in a small number of lines. Think 93000 for ECG services, 93458 for coronary angiography with left heart catheterization, or imaging-heavy encounters where prior authorization and payer edits already make the workflow tight.
Now layer secondary coverage onto that. If the wrong payer goes first, the claim can deny before anyone reaches the actual coding or authorization issue. If the right payer goes first but the posting team fails to capture line-level adjustments, the secondary may process incorrectly or suspend for additional information.
A practical fix is to hold secondary cardiology claims until the primary EOB has been posted accurately at the service-line level. Summary posting is not enough on interventional work.
For more on how procedure complexity and denial prevention intersect in this specialty, this resource on cardiology revenue cycle management is worth keeping in your SOP library.
Orthopedics brings global packages into the COB problem
Orthopedic claims create a different type of COB confusion because the payment issue may be hidden inside a global period. A surgery such as 27447 carries a global package, and post-op services may be bundled by the primary payer. The secondary payer then has to decide how, or whether, it recognizes any remaining liability after the primary’s global determination.
That means your team should document:
- The primary payer’s global package treatment
- Whether post-op E/M lines were denied as included
- Whether any modifiers such as 24, 25, 57, 58, 78, or 79 changed the primary outcome
Without that context, staff can misclassify a valid global-package issue as a COB problem, or vice versa.
Specialty COB work breaks when billing staff treat the secondary claim as a copy of the primary claim. It isn’t. It is a response to the primary adjudication.
Decoding and Resolving Common COB Claim Denials
A common Monday problem in specialty billing looks like this. An anesthesia claim with multiple time units is denied by the secondary for missing prior payment information. A cardiology stress test claim clears the primary, but the secondary rejects it because the line-level adjudication did not carry over correctly. An orthopedic post-op visit gets parked as patient balance when the account should still be in COB review.
Those are not abstract COB issues. They are workflow failures tied to payer sequence, posting accuracy, and claim construction.
Read the denial like an operations signal
Start with the denial text and the remit details. COB denials usually point to one of three failures: the wrong payer was billed first, the secondary did not receive usable primary adjudication data, or the account has a coding issue mixed in with the COB issue.
The practical question is simple. What does this payer need to process this exact claim line?
That matters more in specialty work than on straightforward office visits. If the primary payer adjudicated only part of an anesthesia claim, or bundled one cardiology line but paid another, the secondary decision depends on those service-line results. If the account was posted in summary form, staff cannot build a clean secondary submission.
A corrective workflow that closes the account faster
Use a fixed process. COB denials age quickly when each biller works them differently.
Confirm active coverage for the date of service
Verify subscriber information, dependent status, effective dates, and whether another plan became primary before the encounter.Rebuild the payer order from the record, not from habit
The sequence stored in the PM system may be wrong. Check the registration notes, eligibility response, and any COB questionnaire on file.Get the primary EOB or ERA before touching the secondary claim
The next payer needs the first payer’s allowed amount, paid amount, patient responsibility, and denial reasons. If crossover failed, assume manual secondary work is required until proven otherwise.Post adjudication at the line level
This step decides whether the rebill works. For cardiology and anesthesia, summary posting causes repeat denials because the secondary cannot interpret bundled lines, reduced lines, or unpaid lines correctly.Review code and modifier impact before resubmission
Orthopedic claims may turn on whether modifier 24, 25, 57, 58, 78, or 79 changed the primary outcome. Anesthesia claims may require accurate handling of qualifying circumstances, medical direction modifiers, or time-based reimbursement logic. If the primary processed a line differently because of coding, the secondary claim has to reflect that adjudication.Resubmit with complete COB information
Send the prior adjudication data electronically when the payer accepts it. Attach the primary EOB when the payer requires documentation.Stop patient billing until the sequence is resolved
Early statements create avoidable calls, complaints, and payment reversals.
Common COB denial patterns and what they usually mean
| Denial pattern | What it usually means | Best next action |
|---|---|---|
| Another payer may be primary | Payer sequence is wrong or outdated | Verify coverage and rebill in the correct order |
| Secondary needs prior payment information | Primary EOB details were not transmitted or posted correctly | Obtain the EOB or ERA, post line by line, then resubmit |
| Claim has COB denial plus coding concern | The account has two separate defects | Correct the COB sequence first, then address coding based on the primary adjudication |
| Patient balance dropped before secondary billing | Posting or work queue controls failed | Pull the statement, return the account to COB review, and complete secondary billing |
Specialty practices need denial resolution tied to the claim detail
In anesthesia, COB denials often hide inside unit-based reimbursement. If the primary payer reduced billable units or applied modifier logic that changed payment, the secondary claim cannot be built from the original charge ticket alone.
In cardiology, the risk sits in multi-line technical and professional claims. A primary payer may pay one diagnostic line, deny another as inclusive, and shift cost sharing on a third. The secondary decision depends on that exact line structure.
In orthopedics, the confusion often comes from global surgery rules. A post-op E/M denial can look like a COB issue but is a global package determination by the primary payer. Staff need to separate those two problems before they rebill anything.
COB denials do not resolve with generic follow-up. They resolve when the billing team reconstructs the payer sequence, posts the primary adjudication correctly, and submits a secondary claim that matches how the first payer processed each line.
Happy Billing's Blueprint for Proactive COB Management
Reactive COB follow-up is expensive because every fix happens after charge entry, claim submission, denial posting, and account aging have already consumed labor. The better model is to catch sequencing conflicts before the claim drops.
At Happy Billing, we treat COB as a front-end control, not a denial category. We combine automated multi-payer eligibility checks with human review to catch mismatches in subscriber data, effective dates, and payer sequence before submission. That matters because proper COB directly supports high first-pass clean claim performance and healthier A/R in specialty RCM operations, especially in anesthesia, cardiology, orthopedics, and behavioral health.
We also build workflows around the technical realities of COB. If crossover won’t occur automatically, we flag the account for manual secondary handling early instead of discovering it after payment posts. If a specialty claim includes modifiers that could change downstream secondary behavior, we make sure the primary adjudication is posted in a way the next payer can process cleanly.
The practical result is fewer denial loops, less rebilling, and less account confusion between front office, billers, and patients. This matters most in specialties where a single payer-order mistake can distort reimbursement across units, modifiers, or global surgical logic.
Frequently Asked Questions About COB
What is the difference between COB and subrogation
COB determines the payment order between multiple health plans covering the same patient. Subrogation is different. It usually involves a health plan seeking reimbursement from a third party that is legally responsible for the injury or expense, such as an auto liability carrier.
For billing teams, the operational difference is important. COB asks, “Which health plan pays first?” Subrogation asks, “Who is legally responsible to repay the health plan?”
How does COB work with high-deductible health plans
If a patient has a traditional primary plan and an HDHP as secondary, the primary plan adjudicates first. The HDHP then evaluates the remaining balance under its own deductible and benefit design.
That doesn’t mean the patient automatically owes nothing. The secondary plan may apply the remaining amount toward the deductible before making payment. Your posting team still needs the primary adjudication details to determine the final patient balance correctly.
Can a provider write off the balance after primary and secondary payers have paid
Sometimes yes, but only when the contract supports it. If the practice is in-network with both payers, the combined allowed amount may represent payment in full except for valid patient responsibility such as copay, deductible, or coinsurance.
The key is to classify the remaining balance correctly. A contractual adjustment is not the same thing as collectible patient responsibility. Collecting the wrong amount from the patient after both payers have processed is how practices create avoidable complaints and refund work.
Why do specialty practices see more COB friction
Because their claims carry more variables. Anesthesia adds time units and modifiers. Cardiology adds high-value procedural lines and payer edits. Orthopedics adds global periods and modifier-sensitive post-op billing.
Generic COB advice doesn’t resolve those details. Specialty practices need payer-order discipline plus line-level posting accuracy, or the secondary claim won’t reflect what the primary did.
If your practice is losing time to dual-coverage denials, secondary claim lag, or specialty-specific payer sequencing issues, Happy Billing can help you tighten the workflow before those claims age into avoidable A/R.