Outsource Medical Billing: The 2026 Playbook
Outsource medical billing if your current billing team isn't reliably protecting collections, controlling denials, and keeping cash moving. The reason this decision has become mainstream is simple: the U.S. medical billing outsourcing market was estimated at USD 6.95 billion in 2025 and is projected to reach USD 17.69 billion by 2033, a projected 12.56% CAGR (Grand View Research on U.S. medical billing outsourcing).
You're probably looking at the same signals we see when a practice owner starts this search. A/R is aging. Denials keep resurfacing. Your physician time is getting pulled into billing questions that should never reach your desk. The right playbook isn't “in-house versus outsourced” as an abstract debate. It's a hard review of net collection rate, denial rate, and A/R days, then a vendor screen built around whether a partner can improve those numbers inside your current workflow.
A good billing partner doesn't just submit claims. They increase clean claims, reduce preventable rework, and shorten the time between encounter and payment. That's how you should evaluate every proposal in front of you.
The Framework for Deciding to Outsource Billing
Most owners wait too long to revisit billing. They tolerate slow cash flow because the problems look operational, not financial. That's a mistake. Billing problems are revenue problems.
If your A/R report shows too much aging, if your denial volume keeps forcing rework, or if your front desk is constantly cleaning up eligibility issues after the visit, you don't need another generic billing conversation. You need a decision framework tied to three outcomes:
- Will outsourcing increase net collections?
- Will it reduce A/R days?
- Will the vendor commit to a clean-claim standard that beats your current team?

Three numbers that matter
Owners often focus on control. I focus on leakage. A billing model is working only if it collects what should be collectible, does it fast, and keeps denials from stacking up.
Use this screen:
- Net collection rate: If you can't explain where reimbursement is leaking, you can't defend keeping billing in-house.
- Days in A/R: Slow money is expensive money. Every extra day in receivables strains payroll, hiring, and growth.
- Denial rate and first-pass performance: If claims need too much rework, your billing engine is inefficient no matter how loyal the team is.
Practical rule: Don't outsource because you're frustrated. Outsource because a partner can prove they'll outperform your current revenue cycle on the scorecard that matters.
Advanced practices already treat outsourcing as a normal operating strategy, not a rescue move. If you're comparing models, start with a grounded review of in-house vs outsourced medical billing and then move quickly to your numbers.
What a yes looks like
You should strongly consider outsource medical billing when any of these are true:
- Your lead biller is a single point of failure: One resignation shouldn't threaten collections.
- Your physicians are answering billing questions: Clinical leadership should manage care, not claims queues.
- Your specialty has payer friction: Modifier rules, global periods, prior auth, and procedure-heavy billing expose weak RCM fast.
If none of those are true, keeping billing in-house may be fine. But if two or more are true, this isn't a staffing issue. It's a business model issue.
Building Your Business Case with ROI Modeling
Most owners underestimate the cost of in-house billing because they count wages and ignore drag. The comparison isn't “salary versus vendor fee.” It's total cost to collect versus total cash recovered.
Global analyses consistently tie outsourcing to lower billing costs, faster cash flow, and fewer claim errors, and North America held 49.21% of global revenue in 2025 in this market, which tells you this is already a widely adopted financial strategy, not an experiment (Mordor Intelligence on the medical billing outsourcing market).
What belongs in your ROI model
Start with current-state cost. Include the obvious items, then force yourself to count the hidden ones.
- Direct labor: Billing staff wages, benefits, manager oversight, overtime.
- Technology stack: Practice management tools, clearinghouse fees, eligibility tools, reporting tools.
- Turnover risk: Recruiting, onboarding, retraining, short-term production drops.
- Physician and admin time: Time spent resolving claim issues, payer escalations, patient billing complaints.
- Denial carry cost: Revenue delayed because denials sit too long, get reworked slowly, or miss follow-up.
- Compliance upkeep: Coding updates, payer rule monitoring, process retraining.
In-House vs. Outsourced Billing Cost Analysis
| Cost Component | In-House Example | Outsourced Example |
|---|---|---|
| Staffing | Salaries, benefits, PTO, coverage gaps | Vendor fee tied to collections |
| Training | Ongoing CPT, ICD, payer rule updates | Included in vendor operating model |
| Software | PM system, clearinghouse, scrubber, reporting | Often handled within vendor workflow |
| Turnover | Hiring delays and lost knowledge | Shared team structure reduces dependency on one person |
| Physician time | Escalations, documentation clarification, billing questions | Lower if vendor owns claim follow-up well |
| Denials | Internal rework burden and aged receivables | Vendor should absorb active denial management |
| Reporting | Often manual or inconsistent | Should be scheduled and standardized |
That table isn't theoretical. It's the baseline you need before you evaluate a percentage fee.
How to model the upside
Don't ask, “What does the vendor charge?” Ask, “What revenue are we failing to collect now, and how quickly are we collecting the rest?”
Build your model around three comparisons:
- Current collections versus expected collections
- Current days in A/R versus target A/R
- Current denial rework burden versus outsourced rework burden
If your team posts payments accurately but doesn't aggressively work denials, the problem isn't labor cost. It's cash recovery. If your front office is missing prior authorization or eligibility details and your billers are fixing it after the visit, the cost isn't visible on payroll. It shows up in delays and write-offs.
A cheap billing setup that tolerates leakage is more expensive than a higher-fee partner that collects correctly the first time.
Before you sign anything, benchmark your proposals against your own internal math. A vendor should be compared to your real cost structure, not the simplified version sitting in your head. If you need a pricing lens before that conversation, review how outsource medical billing cost is typically structured and then pressure-test what is and isn't included.
The mistakes that ruin ROI analysis
Owners usually miss three things:
- They ignore unworked denials. Revenue that sits untouched is still a cost.
- They treat physician interruptions as free. They aren't.
- They compare a full-service vendor to a partial in-house scope. That distorts the decision.
A clean ROI model will tell you whether to outsource, keep billing in-house, or use a hybrid arrangement. Gut feel won't.
Your Vendor Evaluation Checklist
Most billing companies sound similar until you ask operational questions. That's where weak vendors fall apart.
High-performing outsourced teams typically achieve a 10 to 20% higher claim approval rate than in-house staff, and the benchmark for first-pass acceptance is the mid-to-high 90s. If a vendor can't talk clearly about clean claims, they're not serious about revenue performance (CPA Medical Billing on outsourced billing performance).
Ask these questions before you sign
Use these in vendor interviews. If the answers are vague, move on.
What first-pass acceptance rate do you target for my specialty?
A good answer is specific and tied to workflow. A bad answer is “we work hard to minimize errors.”How do you prevent denials before claim submission?
Listen for eligibility verification, authorization checks, coding review, modifier review, and claim scrubbing.How do you categorize and work denials?
You want denial buckets by root cause, payer, and aging, not a generic promise to “follow up.”Will you work inside our current EHR and PM system?
Forced migration is often a red flag unless there's a compelling technical reason.What security controls protect PHI?
Ask about encryption, access controls, audit logs, secure environments, and breach response.
What a strong answer sounds like
A strong vendor can explain how they handle errors tied to real claim logic. They should discuss modifier mismatches, diagnosis-to-procedure edits, prior auth gaps, and payer-specific documentation issues. If they can't speak in that level of detail, they're a claim processor, not an RCM partner.
For the security side, don't stop at HIPAA buzzwords. Your billing partner is part of your operational risk surface. If you want a practical parallel for vetting infrastructure vendors, the checklist for selecting co-managed IT services is useful because it forces the same discipline around accountability, systems access, and oversight.
If a vendor won't commit to measurable reporting, they're asking you to trust what should be audited.
Red flags that should kill the deal
- No specialty examples: They keep describing generic workflows.
- No KPI reporting cadence: You should get scheduled visibility into claims, denials, A/R, and collections.
- No denial ownership: If they “submit and notify,” you still own the hardest part.
- Manual workarounds everywhere: Spreadsheets and file dumps create blind spots.
- Opaque handoffs: You can't tell who is responsible when a claim stalls.
A practical shortlist should leave you with only vendors who can defend process, technology, and accountability. If you need a side-by-side rubric, use this guide to the best medical billing company as a checklist, not as a directory.
Why Specialty-Specific Billing Expertise Matters
Generic billing is where specialized practices lose money.
The central question isn't whether a vendor can submit claims. It's whether they can materially reduce leakage in your specialty, especially when reimbursement depends on coding logic like base-unit math, global periods, or multiple-procedure reductions (Pharmbills on specialty-specific outsourcing questions).
Where generalist vendors miss revenue
In anesthesiology, billing isn't just CPT entry. Payment depends on time units, base units, physical status modifiers, concurrency, medical direction rules, and clean documentation. A vendor that doesn't understand these mechanics will create underbilling, overbilling risk, or both.
In orthopedics, the mistakes look different. If a procedure falls inside a global period, if a related E/M should carry modifier 24 or 25, or if multiple procedures trigger payment reductions, your collections depend on judgment, not just data entry. Modifier 22 can matter on unusually difficult procedures, but only when documentation supports it and the team knows how to present it to the payer.
Specialty examples owners should test for
- Anesthesiology: Ask how the vendor handles concurrency, modifiers such as AA, QK, QX, and physical status modifiers. If they can't answer cleanly, they shouldn't touch your claims.
- Orthopedics and pain management: Ask how they manage global periods, modifier 22, modifier 24, modifier 25, and multiple procedure reductions.
- Mental health: Ask how they prevent authorization-related denials and manage visit frequency limits.
- Cardiology and imaging-heavy specialties: Ask how they handle diagnostic edits, procedural bundling, and payer documentation expectations.
The more your reimbursement depends on specialty nuance, the less room you have for a commodity billing vendor.
That's also why front-desk systems matter. In behavioral health, for example, scheduling and patient communication can affect authorization timing and continuity of care. If you're evaluating workflow support around intake and communication, this example of My AI Front Desk for therapy shows the kind of operational layer that can reduce missed handoffs before claims are even created.
What to look for instead
You want a partner that can describe your specialty's actual failure points. Not “we handle all specialties.” That's marketing. You want “here's how we prevent leakage in your claims.”
A useful starting point is reviewing vendors against the specialties they actively support. This list of specialty medical billing services is the right idea. Match any vendor's pitch to your own specialty's billing reality before you sign.
Managing the Transition A 90-Day Go-Live Plan
Most practices delay outsourcing because they expect a messy cutover. That fear is reasonable. A bad transition can freeze claims, break payer workflows, and confuse staff.
A good transition is structured, short, and visible.
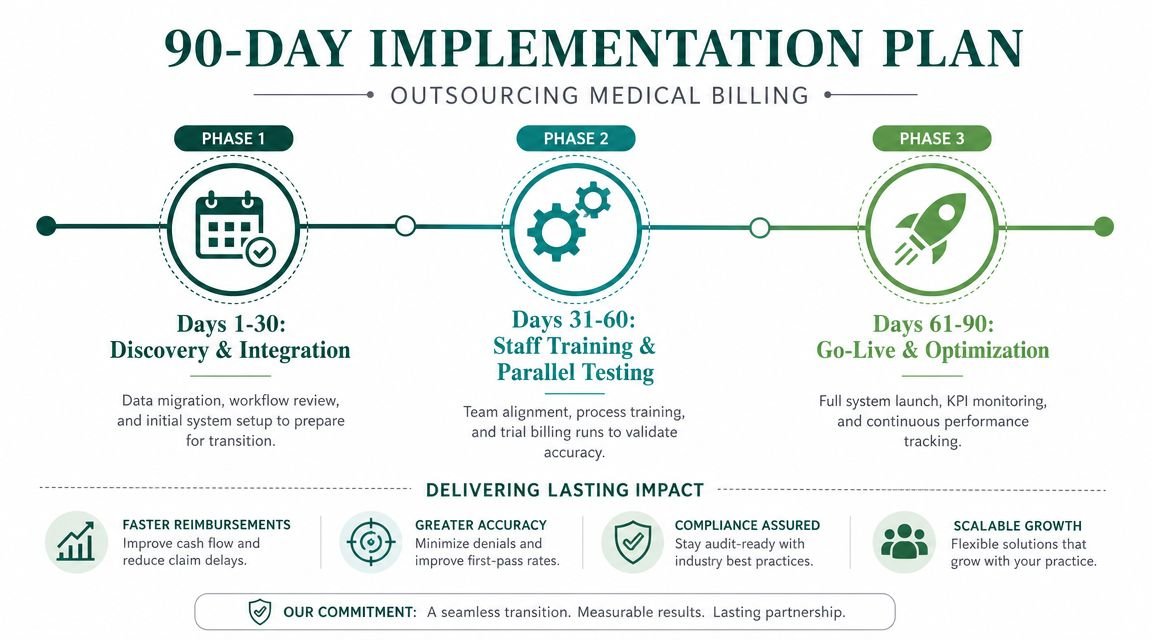
Days 1 to 30
The first month is about setup and risk control.
Your practice should provide system access, payer lists, fee schedules, aging A/R detail, denial reports, and current workflow maps. The vendor should validate user permissions, reporting fields, payer enrollment status, and claim-routing logic.
Focus on these tasks:
- System access: Role-based access inside the current EHR and PM system.
- Payer readiness: Enrollment checks, ERA and EFT validation, claims routing review.
- Workflow ownership: Who handles front-end eligibility, auth, coding review, denial escalation, and patient balance calls.
If you're adding providers or opening locations, credentialing status has to be verified early. For this reason, a realistic credentialing timeline for a new practice becomes operationally important, because enrollment gaps can cripple a launch.
Days 31 to 60
This is the stabilization window. Claims are moving, but the real work is catching friction before it spreads.
The vendor should reconcile daily posting activity, monitor first submissions closely, and flag denial patterns immediately. Your internal team should escalate documentation gaps and front-desk errors in real time.
Look for fast feedback on:
- Eligibility misses
- Authorization gaps
- Charge lag
- Modifier-related edits
- Payer-specific rejections
Early go-live problems are useful if they get surfaced fast. Hidden problems are what wreck a transition.
Days 61 to 90
By this point, you should have enough reporting to judge whether the relationship is working.
Review the first full performance cycle and ask direct questions. Are denials tied to front-end intake, coding, or payer behavior? Is charge entry timely? Is A/R aging improving in the right buckets? Are underpayments being identified and pursued?
This is also the right time to tighten operating rules with the front desk and providers. If repeat issues stem from missing referrals, unsigned notes, or weak documentation support for modifiers, the vendor and practice need a closed-loop process. Without that, outsourcing becomes a downstream cleanup job instead of a real RCM improvement.
Measuring Success KPIs and Your Next Step
If outsource medical billing is the right move, the proof will show up in monthly reporting. Not in promises.
Published summaries report that outsourcing firms often achieve collection rates of 95% or higher, compared with an in-house average around 70%, and some practices report a net revenue increase of over 5% when the vendor gets pre-service verification, claim scrubbing, and denial follow-up right (MEG Business on outsourcing and collections).
The KPI scorecard that matters
Track these every month:
- Denial rate: If it isn't falling, your process still has front-end or coding failures.
- Net collection rate: This tells you whether collectible dollars are being recovered.
- Days in A/R: This shows whether cash is moving or stalling.
You should also require root-cause reporting. “Denials were worked” is not reporting. You need payer trends, aging by bucket, top edit categories, and an action plan.
Put accountability in the contract
Your service agreement should define reporting cadence, ownership of denials, escalation timeframes, and workflow responsibilities between your staff and the vendor. If it's not explicit, it will become ambiguous the first time a payer problem hits.
We've seen that the best outsourcing relationships aren't built on enthusiasm. They're built on disciplined review. If you want a simple benchmark sheet before changing vendors, start with these medical billing KPIs to track.
If your current billing reports are inconsistent, your denial trends are unclear, or your A/R feels worse than it should, the next step is simple. Get an outside audit before you make another staffing or vendor decision.
Frequently Asked Questions About Outsourcing
Will I lose control if I outsource medical billing
Only if you choose the wrong partner.
A well-run outsourced model gives you more visibility, not less. You should expect scheduled KPI reporting, documented denial workflows, and clear ownership by task. If a vendor can't show you what's happening in claims, A/R, and denials, you aren't outsourcing. You're going blind.
Should I outsource everything or keep some billing tasks in-house
That depends on where your practice creates the most friction. Many groups keep patient-facing intake and documentation support in-house while outsourcing coding review, claim submission, denial management, and A/R follow-up. The right split is the one that preserves accountability. If two teams are involved, responsibilities must be explicit.
How long does it take to know whether a new billing partner is working
You should see leading indicators early, especially around cleaner submissions, faster denial handling, and tighter reporting. The deeper financial impact takes longer because older A/R and payer lag don't disappear overnight. What matters most at the start is whether the vendor is catching problems fast and showing you exactly how they're fixing them.
What's the biggest mistake practice owners make when switching billing vendors
They buy on fee instead of performance. A lower percentage means nothing if denials rise, A/R stretches, or specialty-specific coding errors keep leaking revenue. The best vendor isn't the cheapest. It's the one that protects collections in your actual specialty and proves it with reporting.
If you're deciding whether to outsource medical billing, fix an underperforming RCM team, or replace a billing company that isn't moving the numbers, book a free billing audit with Happy Billing. We'll review your denial patterns, A/R bottlenecks, and revenue leakage so you can make the decision based on facts, not frustration.