Top Medical Billing Services Austin: 2026 Guide
If you're shopping for medical billing services in Austin, don't pick the vendor with the prettiest dashboard or the loudest promise about a 98% clean claim rate. Pick the one that can protect your cash flow in Texas and in your specialty. That's the difference between steady deposits and an aging A/R report that keeps getting worse.
We see the same situation all the time. A physician owner opens the monthly report, sees too much money sitting in A/R, and hears the same explanation from staff or a current vendor: denials are up, payers are slow, appeals are pending. Some of that is real. Most of it is operational. If your billing partner can't control denials, filing deadlines, modifier usage, and follow-up velocity, your practice loses revenue and your A/R days stretch.
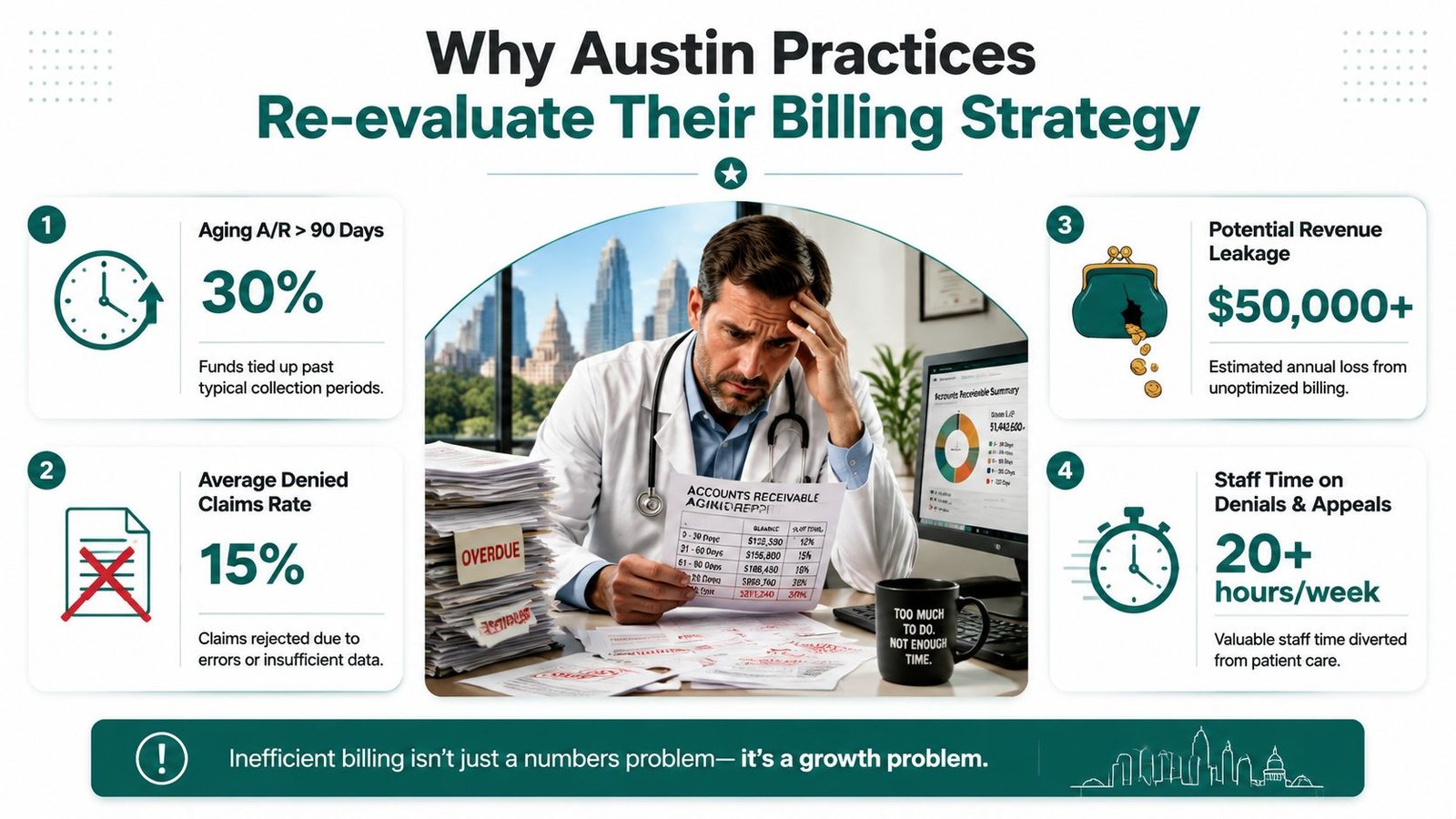
Why Austin Practices Re-evaluate Their Billing Strategy
A busy Austin practice usually doesn't start looking for a new billing partner because billing is interesting. It starts because the numbers feel wrong. Charges are going out, visits are happening, but cash isn't landing fast enough.
That pressure isn't isolated. The U.S. medical billing outsourcing market was valued at USD $5.7 billion in 2023 and is projected to grow at a CAGR of 11.78%, and in Texas 37% of practices struggle with revenue cycle inefficiencies. Poor billing practices cost providers an estimated $125 billion annually nationwide, according to this medical billing industry analysis. If your collections feel harder than they should, you're not imagining it.
The wrong question is should you outsource
The right question is whether your current billing model can reduce denials and speed up cash.
Some practices should keep parts of RCM in-house. Others should outsource aggressively. But the decision has to come down to revenue protection. If front-desk eligibility is sloppy, authorization workflows are inconsistent, and claim edits aren't specialty-aware, your team burns time fixing preventable problems after the claim is already denied.
That's why intake matters more than most owners realize. If you're tightening front-end controls, this guide on how to automate clinic patient intake is worth reading because better intake data directly lowers preventable denials before billing even begins.
What owners should actually evaluate
When physicians compare medical billing services in Austin, they often focus on generic promises. That's a mistake. Vet these areas instead:
- Texas payer fluency: Can the vendor manage state-specific deadlines and payment rules without excuses?
- Specialty coding depth: Do they understand your high-risk CPT and modifier patterns, not just family practice basics?
- Cash velocity: Can they show how they keep A/R moving and prevent old balances from stalling?
- Denial discipline: Do they fix root causes upstream, or just work denial queues after the damage is done?
A billing partner should make your cash arrive faster, not just submit claims on your behalf.
If you're weighing outsourcing against fixing a struggling internal process, this breakdown of Texas medical billing outsourcing considerations is a useful benchmark. The key point is simple. Outsourcing only works when the vendor is better than your current system at preventing leakage.
Navigating Austin's Unique Payer Landscape
National billing vendors love saying they understand local payers. In Austin, that's not enough. Texas has payer rules that directly affect whether you get paid, when you get paid, and whether a denied claim can still be recovered.

TMHP isn't forgiving
Austin practices dealing with Texas Medicaid can't afford a billing team that misses deadlines. 45% of Texas Medicaid claims are denied due to timing errors, driven by TMHP's strict 95-day filing clock, and Texas Prompt Pay Law enforcement can add penalties of up to 18% interest on slow payers, based on this Texas billing guide.
That has immediate financial consequences. If a claim misses the filing window, you don't have a workflow problem. You have a revenue loss problem.
In our experience, owners should stop asking, "Do you bill Texas Medicaid?" and start asking questions that expose whether a vendor controls the process.
Ask these questions before you sign
Use direct questions. If the vendor can't answer cleanly, move on.
How do you track the 95-day TMHP filing clock from date of service to submission?
You want a process answer, not marketing language.What happens when documentation is incomplete near deadline?
A strong partner has an escalation path, not a shrug.Who monitors underpaid or slow-paid claims for Prompt Pay recovery?
If nobody owns it, the practice leaves money on the table.How do you separate workflows for Medicare, commercial plans, TMHP, and TRICARE?
One generic queue usually means avoidable rework.
Practical rule: If a vendor can't describe its filing-deadline controls in operational detail, it will eventually miss one that matters.
Local familiarity isn't enough
Some Austin vendors sell proximity as if being nearby guarantees performance. It doesn't. You need payer rule execution, not a local zip code.
That applies beyond state rules too. Federal and payer-specific compliance matters. If your practice is also sorting out patient billing obligations and estimate workflows, the broader compliance issues around No Surprises Act requirements should sit on the same evaluation list. A billing partner who treats compliance as an afterthought creates downstream A/R friction.
A strong Austin billing operation should know when a claim needs immediate filing, when an authorization issue threatens reimbursement, and when payment delays require escalation. If they can't do that, your staff ends up babysitting the vendor. That's not outsourcing. That's adding another layer of overhead.
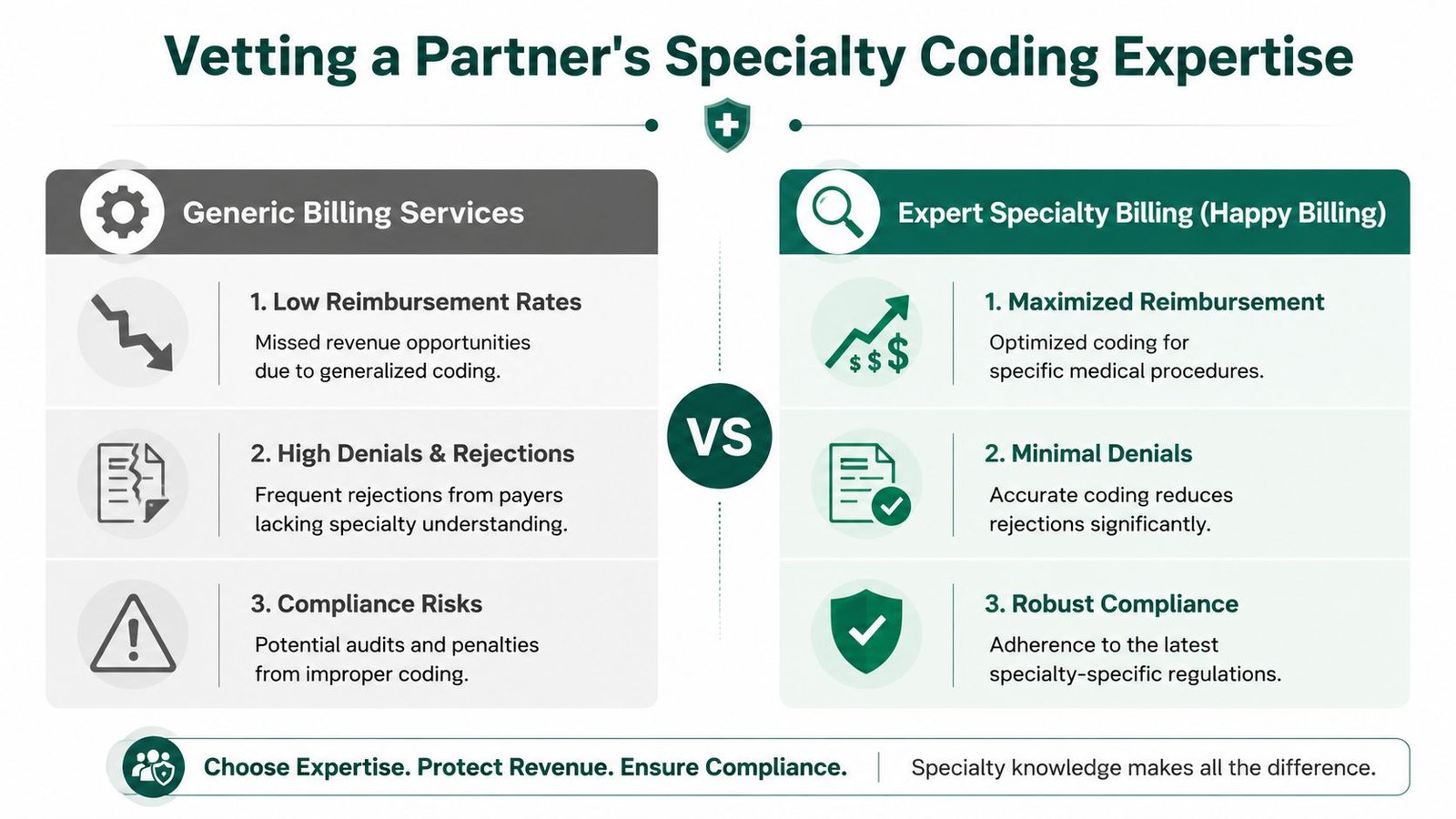
Vetting a Partner's Specialty Coding Expertise
Most medical billing services in Austin advertise the same thing. Clean claims, fewer denials, better follow-up. That's table stakes. A key question is whether the team understands the coding mechanics that drive reimbursement in your specialty.
Most Austin billing service pages highlight a 98% clean claim rate but omit how partners handle specialty-specific modifiers. Data shows 30% of anesthesia denials stem from modifier errors alone, according to this Austin billing analysis. That's exactly where generic billing teams fail.
Anesthesiology punishes generic billing
Anesthesia billing isn't just about sending out a claim with the right CPT. The money is in the details. Base units, time units, concurrency, and modifier handling all affect payment.
If a billing partner mishandles modifiers like QK, AA, or 63, your practice can lose reimbursement or trigger denials that slow collections. A vendor might still brag about a clean-claim metric even as they underbill or misbill anesthesia services. That's why owners need to ask how the team handles anesthesia time documentation, concurrency logic, and modifier selection under payer policy and AAPC-aligned coding standards.
If anesthesiology is your core service line, review a specialty-specific billing framework instead of relying on generic promises. This page on anesthesiology billing support gets closer to the level of detail you should expect from any serious vendor.
Orthopedics has different failure points
Orthopedic revenue leaks happen in different places. A generic biller may know the procedure code and still mishandle the global period.
Modifiers 58, 78, 79, and 59 matter because they determine whether a follow-up procedure gets paid correctly, denied, or bundled improperly. If your billing partner doesn't understand postoperative global logic, multiple procedure rules, and payer edits around procedural distinctness, your surgeons can perform legitimate work that never turns into collected revenue.
Here is the owner-level test. Ask the vendor to explain, in plain English, how they decide between those modifiers during a global period. If they answer with textbook language and no workflow detail, they probably don't have the depth.
What specialty depth looks like in practice
A capable specialty billing partner should be able to discuss:
- Modifier decision-making: Not just what modifier 59 is, but when its misuse leads to denials or audit risk.
- Procedure family logic: How they review related services inside orthopedic global windows or anesthesia concurrency scenarios.
- Documentation alignment: How they push providers and staff to capture the details needed before claim submission.
- Payer-specific edits: How they adjust for rules that differ across Medicare, Medicaid, TRICARE, and commercial plans.
Generic billing gets claims out the door. Specialty billing protects reimbursement.
CMS guidance and payer policies set the outer rules, but execution is where practices get paid or don't. That's why specialty coding knowledge should be part of vendor evaluation, not an afterthought after contract signing.
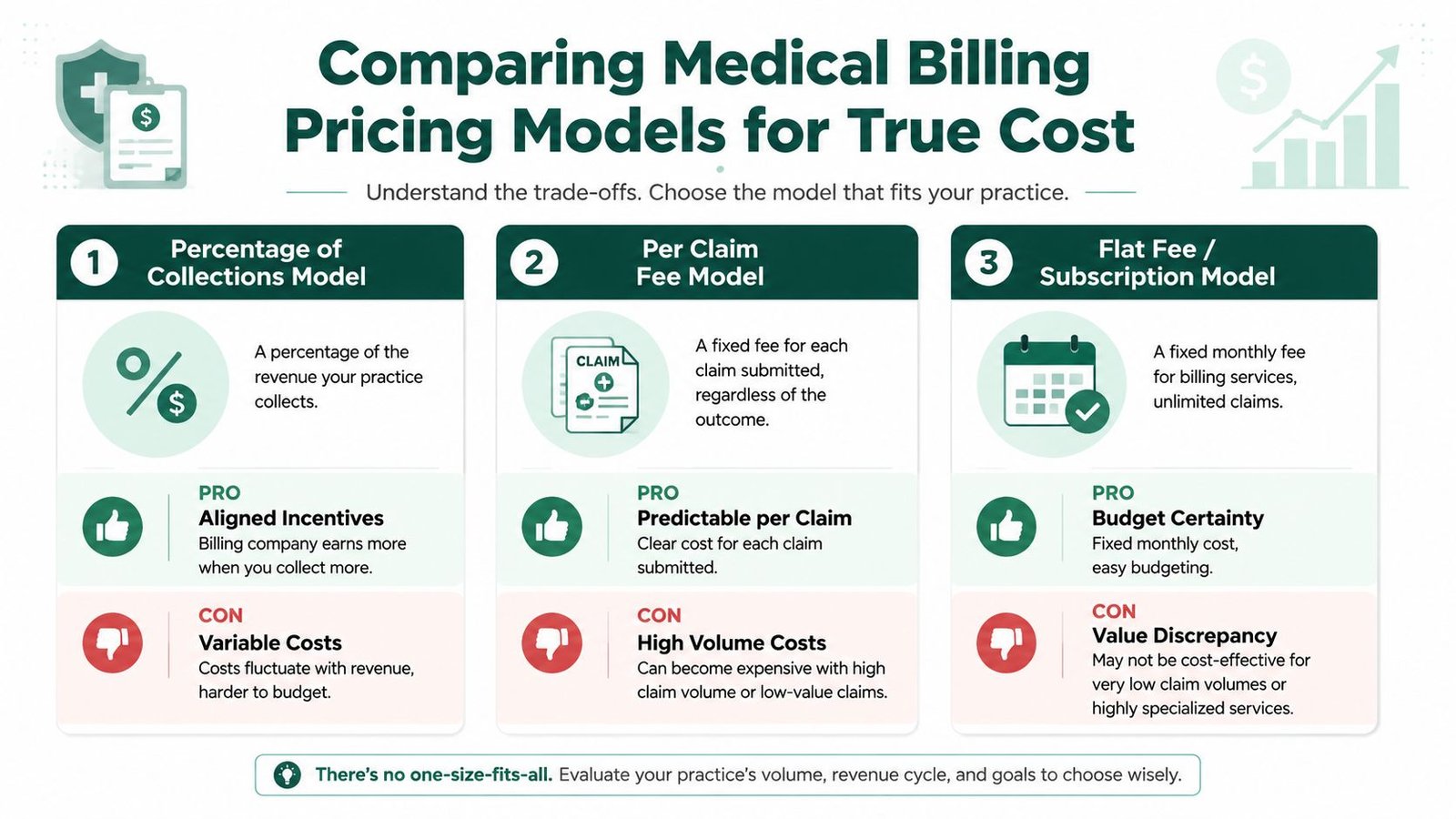
Comparing Medical Billing Pricing Models for True Cost
Most owners start by asking, "What's your percentage?" That's understandable, but it's not enough. The cheapest quote often becomes the most expensive arrangement once denials, hidden fees, and weak follow-up start dragging down collections.
Medical billing service costs in 2026 range from 4% to 10% of net collections, and hidden fees for setup and patient statements can increase true annual cost by 15% to 30%. The same analysis notes that a skilled partner can reduce denial rates by up to 30% through better intake alone, which is why surface-level pricing can be misleading. See the full breakdown in this guide to medical billing pricing ranges and hidden fees.
Three models and when each works
| Pricing model | Best fit | Main upside | Main risk |
|---|---|---|---|
| Percentage of collections | Many independent practices | Incentives stay aligned with collections | Cost rises with revenue |
| Per-claim fee | High-volume claim environments | Clear unit economics | Bad fit if claim count is high and values are low |
| Flat fee or hybrid | Predictable operations | Easier budgeting | Can hide gaps in service scope |
What to compare beyond the quote
A serious vendor comparison should include more than price.
- Included services: Does the fee include denial management, credentialing support, patient statements, and A/R follow-up?
- Front-end work: Will they handle eligibility and authorization workflow, or only back-end claim submission?
- Specialty complexity: A vendor billing cardiology or orthopedics should be stronger operationally than one built for basic office visits.
- Reporting depth: Can they tie cost to net collections, denial trends, and aging buckets?
The right pricing model is the one that leaves you with more collected revenue after fees, not the one with the lowest headline percentage.
If you want a cleaner way to compare proposals, use a total-cost framework like this guide on what outsourced medical billing really costs. Owners should evaluate the vendor's impact on collections, not just the invoice they send.
The Key Performance Indicators You Must Demand
A vendor can brag about clean claims all day and still leave your practice short on cash. Austin owners should judge billing partners on four numbers that show whether revenue is arriving on time, whether Texas payer friction is being controlled, and whether specialty coding mistakes are being caught before they turn into denials.
Start with initial denial rate. If a billing company cannot keep it below 5%, you have a process problem, not a reporting problem. In Austin, that usually traces back to preventable issues. Medicaid filing mistakes through TMHP, authorization gaps for imaging or surgery, modifier errors in orthopedics, or payer edits that were never built into the workflow.
Days in A/R comes next. This is your cash speed. If claims sit too long, payroll, rent, and provider comp get tighter. Ask for A/R broken out by payer and aging bucket, not a single blended number. A vendor that handles Texas plans well should be able to show where claims stall, who owns follow-up, and how quickly underpayments move to appeal.
Net collection rate tells you how much collectible revenue you get. Appeal success rate tells you whether the team can recover money after a payer says no. Those two metrics separate real operators from companies that just submit claims and send polite monthly summaries.
The KPIs that belong in your contract
Put these in writing.
- Initial denial rate: Target below 5%, with denial categories reported monthly.
- Days in A/R: Set a clear goal and require aging by payer, provider, and financial class.
- Net collection rate: Track how much allowed revenue is collected after contractual adjustments.
- Appeal success rate: Measure recovered dollars, not just appeal volume.
- First-pass resolution by payer: Require visibility into which Texas payers create repeat rework and underpayments.
A billing partner that works complex specialties should also report coding-related denials separately from eligibility, authorization, and filing-limit denials. That is how you see whether the problem is front desk discipline, payer follow-up, or specialty coding weakness.
What good reporting looks like
Monthly reports should answer three questions fast. Where is cash stuck? Why did claims deny? What changed from last month?
If the report cannot show performance by payer, provider, CPT family, and denial reason, it is not good enough. Generic dashboards hide the exact problems Austin practices need fixed. Blue Cross underpayments, TMHP timing issues, and specialty-specific modifier denials should never be buried inside a single denial total.
Use a practical medical billing KPI scorecard your team can track monthly to compare vendors side by side. The buying discipline is similar to how to choose a digital marketing agency. The smart move is to compare accountability, reporting depth, and process ownership, not presentation quality.
If your billing company cannot tie its work to faster cash, fewer denials, and lower A/R, you do not have a billing partner. You have a data-entry vendor.
An Actionable Vendor Selection Checklist
Most owners don't need more theory. They need a short list of questions that expose weak vendors quickly.
Use this checklist during calls and demos. It works the same way a strong procurement process works in other service categories. This article on how to choose a digital marketing agency gets one thing right: smart buyers compare process depth, accountability, and fit, not just pitch quality. The same rule applies here.
- Ask for Texas workflow detail: How do you control TMHP filing deadlines, Prompt Pay follow-up, and payer-specific escalation?
- Ask for specialty examples: Show me how you handle modifier QK in anesthesia or modifiers 58, 78, 79, and 59 in orthopedics.
- Ask for KPI accountability: What denial-rate, A/R, and net-collection targets will you commit to in writing?
- Ask what's excluded: Are setup, patient statements, credentialing tasks, and old A/R work billed separately?
- Ask who does the work: Who is reviewing denials, appealing underpayments, and managing payer follow-up day to day?
- Ask how they report: Will I see performance by payer, provider, and denial category every month?
For a fuller interview script, keep this list of questions to ask a medical billing company before hiring open during vendor meetings. Weak partners hate precise questions. Strong ones answer them fast.
FAQs From Austin Practice Owners
How long does onboarding usually take for a new billing partner
Judge onboarding by how fast collections stabilize, not how fast the contract gets signed. A vendor that rushes setup and misses front-end edits, charge capture gaps, or old A/R transfer issues will hand you more denials, slower cash, and extra cleanup work for the next 60 to 90 days.
Ask for a week-by-week implementation plan before you sign. It should cover payer enrollment status, EDI setup, claim edit configuration, A/R ownership, and who fixes rejected claims during the transition.
Can a billing company work inside our current EHR
Yes. That should be the baseline, especially if you want to avoid a slowdown in scheduling, charge entry, and provider workflow.
The central question is whether the billing team can produce clean work inside your current stack. Ask them to show how they manage claim scrubbing, denial tasks, posting, and payer follow-up in your existing EHR and PM system. If their answer is "we prefer you move platforms," expect disruption, retraining costs, and slower collections before you see any improvement.
What security standards should I expect from a billing vendor
Expect HIPAA compliance, encrypted data transfer, role-based access, audit logs, and clear rules for who can touch PHI. Ask how they handle remote access, password controls, device security, and file sharing.
Vague answers here are disqualifying. A billing partner handles patient data and payment data every day. Sloppy security creates legal risk, operational risk, and expensive distractions that pull attention away from collections.
Is a local Austin billing company better than a national one
Only if they can handle Texas payer rules and your specialty's coding risk better than the alternatives. Geography does not improve net collections.
Choose the partner that can explain Texas Medicaid workflows, payer-specific denial patterns, and specialty coding details without reading from a script. If you run anesthesia, orthopedics, cardiology, pain management, or another high-complexity specialty, generic billing support will cost you in underpayments, appeals, and aging A/R.
If your practice is dealing with recurring denials, old A/R, or a billing vendor that reports activity instead of results, get an outside review of the revenue cycle and compare that feedback against what your current team tells you. You can also explore Happy Billing to see what specialty-focused medical billing support should look like for an Austin practice.