Anesthesia Codes CPT: A Practice Owner’s Financial Guide
A profitable anesthesia practice can lose revenue on a clean-looking claim if the coding workflow misses one operational detail. I see it when a case is billed with the correct anesthesia CPT, but the time record is incomplete, the modifier does not match the staffing model, or the documentation cannot support the level reported. The claim leaves the office, but reimbursement drops, denials rise, and A/R stretches for reasons that are hard to spot unless you review anesthesia coding as a revenue diagnostic, not just a coding task.
That is the use of anesthesia codes CPT for an owner. They help expose where money is leaking across the billing process, from charge capture to payer adjudication. A practice with solid case volume can still underperform if anesthesia records, modifier selection, and payer edits are not aligned with the billing rules your team is using every day.
For anesthesia groups, surgery centers, and physician owners, margin disappears in those small misses. A few undercoded minutes, one unsupported physical status modifier, or a supervision modifier that conflicts with the documentation can turn a payable claim into a reduced payment, a denial, or an audit risk. That is why strong RCM for physician practices starts with understanding how anesthesia coding affects cash, not just compliance.
The Anesthesia Billing Formula That Dictates Your Revenue
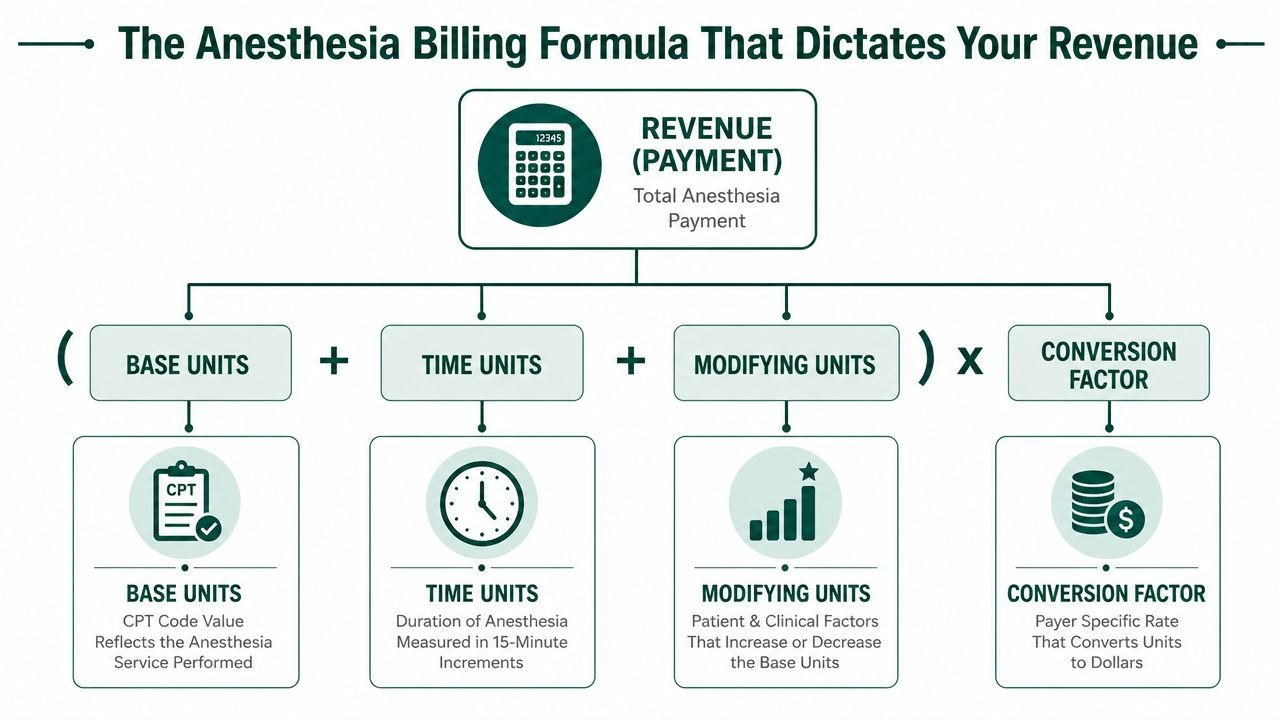
Anesthesia revenue is won or lost in a simple payment formula. Every claim is built from base units, time units, and modifying units, then priced under the payer's anesthesia conversion factor. If one input is wrong, the claim may still go out clean and still pay short.
That matters to owners because anesthesia billing errors often hide inside claims that look complete. The CPT may be correct. The money still slips if time is understated, the provider role modifier does not match the staffing model, or the documentation does not support the physical status reported.
Where the formula breaks down financially
Owners often assume reimbursement starts and ends with the anesthesia CPT code. In practice, the formula has several failure points. A claim billed with the right anesthesia code can still be reduced if the record does not support reported minutes, if AA, QK, QX, QY, QZ, or QS is assigned incorrectly, or if P1 through P6 is added without clear clinical support.
Those are revenue leaks, not abstract coding issues. They show up as avoidable denials, underpayments that no one appeals, and longer A/R because staff have to rework claims that should have paid correctly the first time.
I see one pattern repeatedly. Practices track denials by payer, but they do not track which part of the anesthesia formula failed. That makes root-cause work harder than it needs to be.
What strong RCM teams do
The strongest teams treat the formula as a pre-bill financial checkpoint:
- Match charge entry to the finalized anesthesia record. Start and stop times, discontinuous time, and documentation gaps should be resolved before claim release.
- Validate modifier logic against the staffing model. If the chart supports medical direction, the claim has to reflect medical direction rules. If it supports personally performed anesthesia, the modifier should say that clearly.
- Review payment variance by formula component. A payer trend tied to time reduction, physical status downgrades, or role modifier edits points to a fixable process problem.
Owners can now exert control. Instead of waiting for denials to reveal weak spots, the billing team can use the formula to spot where net collections are being diluted upstream. That approach is part of disciplined RCM for physician practices.
Practical rule: A submitted anesthesia claim is only valuable if every payment element in the formula is supported before it reaches the payer.
Navigating Anesthesia CPT Code Ranges 00100-01999
The anesthesia section of CPT is one of the most distinct parts of the code set. It spans 00100-01999 and is organized by anatomy and procedure type, not by a single generic service category. Key ranges include 00100-00222 for head, 00300-00352 for neck, 00400-00474 for thorax, 00500-00580 for intrathoracic procedures, and 00600-00670 for spine and spinal cord. The range ends at 01999, which is used for unlisted anesthesia procedures when no more specific code fits (Anesthesia Business Consultants overview of anesthesia CPT ranges).
For a practice owner, that structure matters because anesthesia code selection is not just clerical routing. It determines the clinical bucket the payer will use to interpret the service. When the code is off, the claim starts from the wrong place.
The ranges are a financial map
Here is the body-region layout commonly used in anesthesia billing:
| Range | Region or category |
|---|---|
| 00100-00222 | Head |
| 00300-00352 | Neck |
| 00400-00474 | Thorax |
| 00500-00580 | Intrathoracic procedures |
| 00600-00670 | Spine and spinal cord |
| 00700-00797 | Upper abdomen |
| 00800-00882 | Lower abdomen |
| 00902-00952 | Perineum |
| 01112-01173 | Pelvis |
| 01200-01274 | Upper leg |
| 01320-01444 | Knee and popliteal area |
| 01462-01522 | Lower leg |
| 01610-01680 | Shoulder and axilla |
| 01710-01782 | Upper arm and elbow |
| 01810-01860 | Forearm, wrist, and hand |
| 01916-01999 | Radiology, burn, obstetric, and other special anesthesia services |
A practice that doesn't understand this framework usually makes one of two mistakes. It either chooses a nearby code because it “looks close enough,” or it overuses unlisted reporting when a specific code exists. Both problems create payment friction.
Where the leak shows up
Owners usually notice this issue through downstream symptoms, not through the code itself:
- More payer edits: Claims pause because the anesthesia code doesn't align cleanly with the operative site or service type.
- Longer A/R: Staff spend time correcting claims that should have been right on first pass.
- Underpayments that slip through: A claim may process, but from the wrong reimbursement starting point.
- Manual review exposure: Unlisted code 01999 can be necessary, but it also increases documentation burden and slows payment.
When I review anesthesia groups with unstable cash flow, code-range confusion often sits upstream of bigger problems. The owner sees denials. The underlying issue is that the charge never matched the operative reality well enough to move cleanly through payer logic.
How Base Units Form Your Revenue Foundation
Base units are the financial floor of an anesthesia claim. Before time is added and before modifiers affect payment logic, the anesthesia CPT code establishes the starting value for the case. If that starting point is wrong, every claim built on top of it is wrong too.
This is why a practice can have decent charge volume and still underperform on net collections. The team may submit claims quickly, but if they repeatedly start from the wrong anesthesia code, they normalize underbilling. Those losses don't always create denials. They often show up as lower payment per case and missed revenue that no one appeals because nothing was formally rejected.
The code sets the starting point
The biggest operational mistake is assuming adjacent anesthesia codes are financially interchangeable. They aren't. Similar surgeries in the same broad region can still map to different anesthesia codes, and that changes the claim's reimbursement foundation.
Owners don't need to memorize every code. They do need to know what to ask when payment looks light:
- Was the anesthesia code selected from the correct operative site and service family?
- Did the team verify the final anesthetic service against the actual procedure performed?
- Are underpayments being compared to the expected unit logic, or only posted and closed?
If your current process doesn't answer those questions consistently, your billing team is likely relying too heavily on habit. That's how underbilling becomes systemic.
What a healthy review process looks like
In our experience, the strongest anesthesia revenue workflows treat code selection as a financial control point. They don't separate coding accuracy from reimbursement performance.
That means:
- Charge capture reviews include the operative context, not just the claim form
- Payments are checked for variance when a code family repeatedly pays lower than expected
- Teams escalate patterns, not just isolated claim errors
A practice can have a low visible denial rate and still lose money every day if the wrong base-unit foundation is being used consistently.
For owners evaluating whether to fix an in-house workflow or outsource, this is one of the first places to inspect. If your partner or internal team can't clearly explain how the anesthesia code determines the claim's starting value, they're not managing anesthesia revenue with sufficient depth. A specialty-focused operational view is what separates generic billing from true anesthesiology billing services.
The Financial Impact of Anesthesia Time Calculation
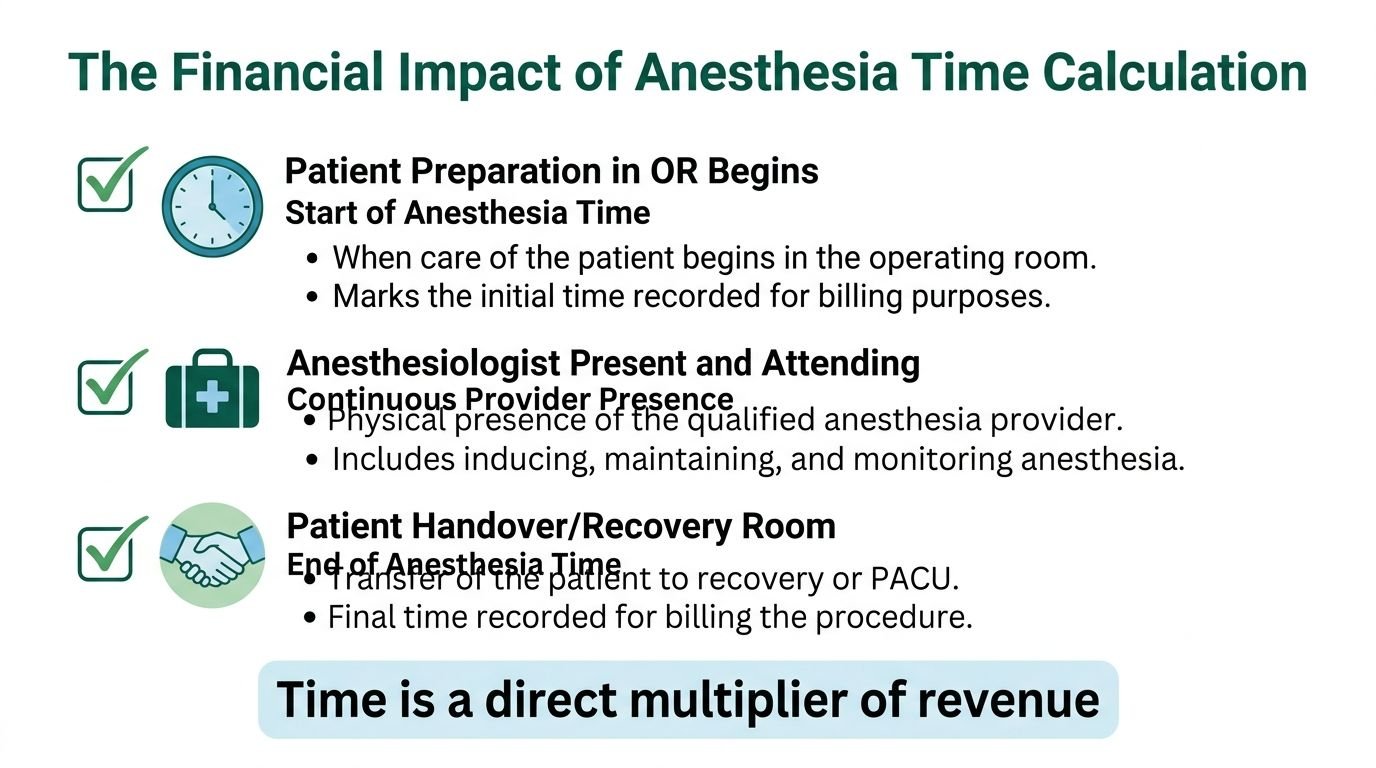
Time is where many anesthesia groups inadvertently lose revenue.
Every anesthesia claim is priced off units, and time units are the variable most likely to be lost through documentation drift, late charge review, and handoff errors. In anesthesia billing, time is generally reported in 15-minute increments. That makes the start time, stop time, and continuity of the record financial data, not clerical detail.
A one-time error is manageable. Repeated time leakage is expensive because it hits three metrics at once. Net collections fall when supported minutes never make it onto the claim. A/R days rise when the billing team has to stop claims and chase missing documentation. Denial risk increases when billed time does not reconcile to the anesthesia record.
The pattern is usually operational, not educational. Anesthesiologists and CRNAs know time matters. The problem is that the anesthesia record, charge entry workflow, and final claim often rely on different people, different timestamps, and different assumptions about when anesthesia time ends.
Common examples include a missed pre-induction start, relief coverage that is documented clinically but not translated correctly for billing, and a stop time entered after the patient leaves the provider's care path. Each one changes units. Each one changes expected reimbursement.
Where time calculation turns into a revenue leak
Owners should look at time capture the same way they look at fee schedule variance or denial write-offs. It is a diagnostic point.
The biggest failure points are usually these:
- Missing endpoints: No clear anesthesia start or stop time leaves the claim weak on support and often forces manual review.
- Handoff inconsistency: Relief cases can break the time trail if provider transitions are not reconciled before billing.
- Rounded documentation: Repeatedly neat times often signal habit-based entry rather than chart-based billing.
- Charge lag: Claims sit unbilled while staff look for clarification, which pushes aging up before the claim even reaches the payer.
- Mismatch between record and claim: If the billed units do not tie back to the finalized anesthesia record, underpayments and payer questions follow.
I tell practice owners to audit paid claims, not just denied ones. Denials show visible failure. Paid claims often reveal the quieter problem. Cases that should have carried more time units but were submitted short. That is a direct net collection loss, and it rarely gets appealed because the payment posts without an obvious edit.
A useful contrast is other time-based reimbursement models, where documentation discipline also determines what gets paid. This overview of the 8-minute rule for time-based billing is a good comparison point, even though anesthesia follows its own unit methodology.
Missed anesthesia minutes usually do not create one large write-off. They create a steady pattern of smaller underpayments that reduce monthly collections and are easy to miss in posted-payment reports.
What improves results
The practices with tighter anesthesia cash flow usually enforce a few simple controls:
- Bill from the finalized anesthesia record, not a provisional charge note
- Hold incomplete time entries for same-day correction before claim submission
- Review recurring exceptions by facility, provider, and scheduler
- Match paid time units against expected units on sampled claims
- Track whether time-related corrections are increasing charge lag or payer scrutiny
This work pays off fast because anesthesia time errors affect more than coding accuracy. They affect how quickly claims leave the door, how defensible those claims are, and how much reimbursement the practice keeps once payment arrives.
Using Physical Status Modifiers to Reflect Case Complexity
Physical status modifiers often look minor on the claim. They are not minor in the revenue cycle.
P1 through P6 tell the payer how sick the patient was at the time of anesthesia care. For an owner, that matters because these modifiers affect reimbursement under some payer contracts, trigger review under others, and expose weak documentation habits almost immediately. If your team treats physical status as a box to fill instead of a coding decision that must be supported, you usually see the result in higher denial touch rates, more chart chases, and slower cash.
The operational problem is usually one of two failures. The practice bills higher-acuity status without enough support in the pre-anesthesia evaluation, comorbid condition documentation, or intraoperative record. Or the practice avoids higher-acuity status even when the record supports it, which leaves legitimate reimbursement on the table.
Both errors cost money.
Where physical status coding creates revenue leaks
Physical status does not work the same way across all payers. Some contracts recognize additional payment for higher-acuity statuses. Some bundle the effect into their own pricing logic. Some scrutinize the modifier closely and request records when the documentation does not match the severity reported. That variability is exactly why owners should audit payer-specific behavior instead of assuming one billing rule fits every book of business.
Here is the practical view:
| Modifier set | Common failure point | Financial effect |
|---|---|---|
| P1-P2 | Added by habit with little review | Usually limited payment impact, but inconsistent use weakens claim integrity and creates noise in audits |
| P3-P5 | Underreported or poorly supported | Can reduce reimbursement where the payer recognizes physical status units, or lead to denials and record requests when support is thin |
| P6 | Rarely used and heavily reviewed | High audit risk if unsupported, with significant delay before payment is released |
A billing manager who knows anesthesia will not ask only, "Was a P modifier present?" The better question is, "Did the record justify the level billed, and does this payer pay for it?" That is the difference between coding for appearance and coding for collections.
What support should exist in the chart
The record should make the severity obvious without a retrospective rescue effort. That usually means the anesthesia note, assessment, and associated diagnoses line up. A patient billed as P3, P4, or P5 should not read like an uncomplicated routine case.
This is similar to other modifier-sensitive claim work. Clean modifier use depends on documentation discipline, not coder intuition. The same principle shows up in broader modifier compliance work, including modifier 59 billing rules and misuse risks, even though the anesthesia payment methodology is different.
Questions owners should ask every month
- Which payers in our mix recognize physical status in payment, and which do not?
- How often are P3-P5 cases getting downcoded, denied, or sent for records?
- Are providers documenting patient severity clearly enough for coders to bill the highest supportable status on first pass?
- Is the team avoiding higher-acuity modifiers to reduce scrutiny, even when the chart supports them?
Those answers show where revenue is leaking. If a payer routinely pays P3-P5 differently and your practice rarely reports them, undercoding is likely depressing net collections. If claims with higher-acuity status sit in A/R while staff chase records, the issue is not the modifier itself. The issue is weak source documentation and preventable rework.
The standard that improves cash
Use the highest supportable physical status. Audit it by payer. Teach providers what documentation supports P3, P4, and P5 in real cases.
That approach protects two margins at once. It reduces underbilling on legitimate high-acuity cases, and it cuts the denials that come from unsupported severity coding. Practices that get this right usually post cleaner payments, spend less staff time on retroactive chart review, and get a more accurate read on which cases and facilities are profitable.
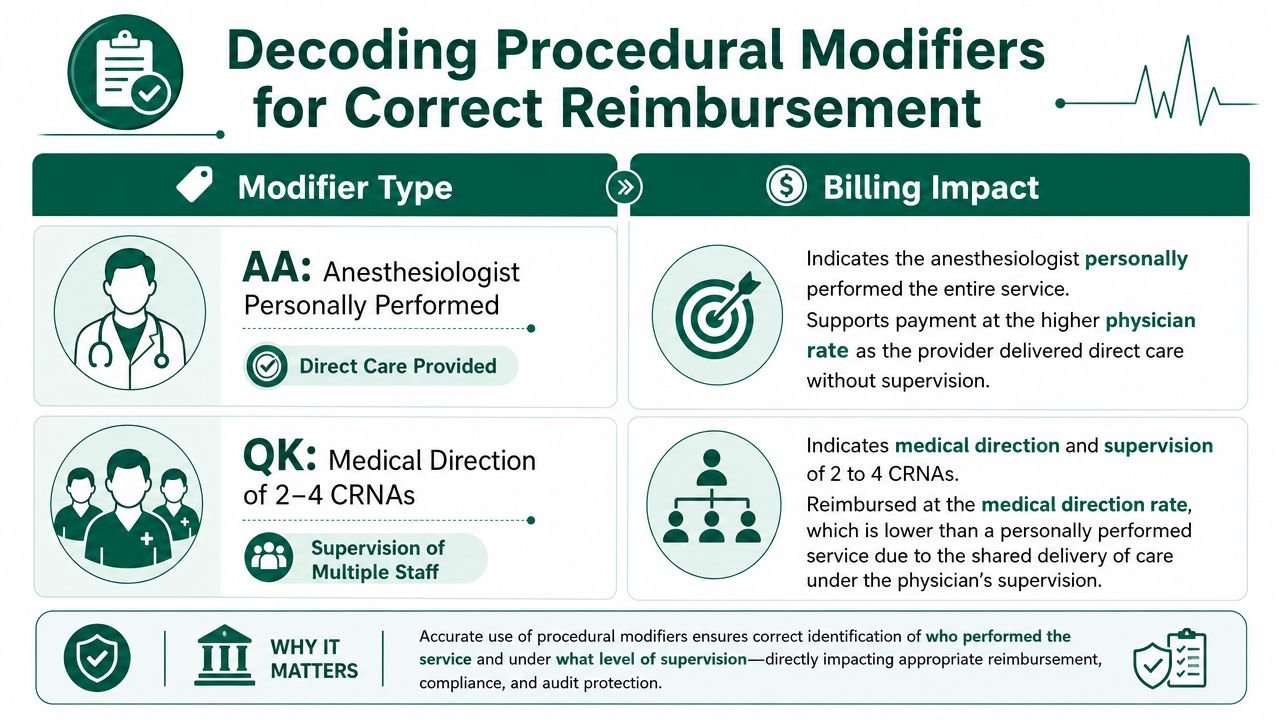
Decoding Procedural Modifiers for Correct Reimbursement
Modifier errors are one of the fastest ways an anesthesia practice gives away revenue. A single wrong modifier can cut payment, trigger a denial, or force staff into avoidable rework that stretches A/R for weeks.
Procedural modifiers on anesthesia claims do more than describe the case. They tell the payer who performed the service, whether the case involved medical direction, and whether special pricing logic applies. If that claim signal is wrong, the claim may still leave the office clean, but it will not land clean financially.
The modifier set owners should recognize
Owners do not need to memorize every coding rule, but they do need to recognize the modifiers that change reimbursement and audit risk on anesthesia claims. The set that shows up most often includes AA, QK, QX, QY, QZ, and QS.
| Modifier | What it signals on the claim | Revenue risk if used incorrectly |
|---|---|---|
| AA | Anesthesia service personally performed by an anesthesiologist | Overpayment risk, recoupment risk, or denial if staffing records do not support personal performance |
| QK | Medical direction of 2 to 4 concurrent anesthesia procedures | Denial or downcoding if concurrency or direction requirements are not supported |
| QX | CRNA service with medical direction by a physician | Mismatch denials if the physician side of the claim is not coded consistently |
| QY | Medical direction of one CRNA by an anesthesiologist | Incorrect split payment or denial when paired billing logic is wrong |
| QZ | CRNA service without medical direction by a physician | Audit exposure if documentation suggests direction occurred but the claim reports none |
| QS | Monitored anesthesia care indicator | Medical necessity review or inconsistent payment if the underlying case documentation is weak |
The practical issue is not whether a modifier exists in the code set. The issue is whether your documentation, staffing model, and payer edits all point to the same answer.
Where owners usually lose money
I see three recurring failure points.
First, modifier selection gets treated like a billing-office cleanup task instead of a front-end operational control. By the time coders are guessing whether a case should be AA, QX, or QZ, the practice has already created denial risk.
Second, paired claims do not match. If the physician claim and CRNA claim tell different stories about the same case, payers often suspend or reject one side. That creates rework, pushes aging higher, and delays cash on claims that should have paid on first pass.
Third, practices assume procedural modifiers are standardized financially across payers. They are not. The code definition may be stable, but contract treatment is not. Owners should review modifier-level payment outcomes by payer, then ask where underpayments, denials, and manual touches are clustering.
The operational check that protects cash
Use modifiers as a diagnostic tool, not just a coding requirement. Pull a monthly report by payer and modifier, then look for patterns such as:
- higher denial volume on QK/QX combinations
- underpayments tied to AA cases at specific facilities
- repeated medical review on QS claims
- unusual use of QZ relative to your actual staffing model
Those patterns usually point to a process problem upstream. It may be poor charge capture, inconsistent staffing documentation, or a payer configuration issue in the billing system.
A useful adjacent reference is this guide to modifier 59 billing rules and misuse risks. It is not anesthesia-specific, but the management lesson is the same. Modifier misuse looks small at the claim level and expensive at the practice level.
The standard to hold your team to
Every procedural modifier should answer a factual question about the case. Who performed the anesthesia service? Was the case medically directed? Does the record support monitored anesthesia care? If the chart and the modifier do not match, net collections fall and follow-up costs rise.
Practices that tighten modifier controls usually see cleaner first-pass payments, fewer avoidable denials, and less staff time wasted on corrected claims. That is why modifiers belong on the owner's revenue leakage dashboard, not just the coder's checklist.
Mastering Concurrency and Medical Direction Rules
Concurrency errors drain anesthesia revenue faster than many owners realize. A case can be coded with the right anesthesia CPT and the right time, then still pay incorrectly or trigger recoupment because the staffing record does not support the modifier set.
The loss shows up in two places. First-pass payment slows because claims hit medical review or come back for correction. Net collections fall later when payers recast medically directed cases as personally performed, supervised, or unsupported based on the documentation trail.
The modifier logic that affects payment
For Medicare, modifier selection has to match the actual delivery model. AA reports anesthesia services personally performed by an anesthesiologist. QK applies when the anesthesiologist medically directs two, three, or four concurrent anesthesia procedures. QY applies to medical direction of one CRNA by an anesthesiologist. The CRNA side of the claim commonly carries QX for CRNA service with medical direction by a physician or QZ for CRNA service without medical direction by a physician. CMS publishes these anesthesia modifier definitions in its HCPCS modifier file and anesthesia payment guidance.
Owners should care because these are not minor coding distinctions. A group that defaults to QK or QX without reconciling the actual staffing pattern builds rework into the claim before it ever leaves the practice.
Where practices lose money
I usually see concurrency revenue leakage start upstream, not in the billing system. The physician covers too many overlapping rooms for the documented model. Relief breaks are not captured clearly. Start and stop times line up, but the record of who was medically directing whom does not.
That creates predictable financial problems:
- claims suspended for manual review because the modifier combination does not fit the documented provider roles
- downcoded or denied cases when physician participation is not supported in the record
- refund risk across multiple dates of service if an audit finds a repeated concurrency pattern
- longer A/R because staff have to rebuild the staffing story after submission
One bad claim is a nuisance. A repeated concurrency defect by facility or provider becomes a margin problem.
The operational controls that protect collections
Practice owners need a monthly concurrency audit, not just coder spot checks. Pull cases billed with AA, QK, QY, QX, and QZ and compare the submitted modifiers against the anesthesia record, staffing assignment, and physician documentation. If those three sources tell different stories, cash is already leaking.
Focus on four controls:
Room overlap review
Confirm that concurrent case counts support the modifier billed for the physician and the nonphysician provider.Provider role matching
The anesthesia record, charge ticket, and final claim need the same staffing model. If one says medically directed and another reads like supervision or independent CRNA care, expect denials or takebacks.Relief and handoff capture
Breaks, relief coverage, and late physician involvement often create documentation gaps that billing teams discover after the claim drops.Denial pattern tracking
Monitor concurrency-related denials by facility, payer, and rendering provider. That gives owners a usable denial management workflow instead of isolated corrections. A structured medical billing denial management process helps identify whether the root cause sits with staffing, documentation, or claim configuration.
Concurrency should be managed like a revenue control, not a coding footnote.
Groups that handle this well usually collect faster because the claim matches the staffing reality the first time. Groups that do not usually blame payer behavior, even though the underlying issue is internal inconsistency between documentation, modifiers, and the medical direction model.
Proactive Denial Prevention for Anesthesia Claims
Most anesthesia denials are preventable. Medicare NCCI policy is explicit that CPT 00100-01999 describes the anesthesia service itself, and providers should not separately report integral components such as certain pain-management injections when they are part of the anesthetic. Proper documentation becomes critical when a separate postoperative pain service may be reportable under narrow circumstances (CMS NCCI policy manual chapter for CPT 00100-01999).
For owners, denial prevention becomes a margin strategy. If your team is routinely sending claims that trigger bundling edits, missing-time edits, or modifier conflicts, your A/R problem is self-inflicted. You're paying staff to create rework, then paying them again to fix it.
The pre-submission checks that matter
A useful anesthesia claim scrub should verify more than demographics and eligibility. It should check whether the billed anesthesia service makes sense as a full anesthetic claim under payer rules.
Focus on these checkpoints:
- Code integrity: The anesthesia CPT should match the operative site and service category.
- Time support: Start and stop documentation must support the billed units.
- Modifier alignment: Procedural and physical status modifiers must match the staffing record and chart.
- Bundling review: If an additional pain service appears on the claim, someone should confirm whether it is separate and supportable.
- Documentation completeness: The record should make the route, timing, and distinct nature of separately billed services clear when permitted.
What not to tolerate
What doesn't work is relying on denial management as the main control. If claims go out wrong and your team waits for payer feedback to correct them, the practice absorbs avoidable delay on nearly every weak claim. Cash slows. Staff burnout rises. Owners lose visibility into whether the problem is coding, documentation, or payer behavior.
A stronger model is to catch predictable failure points before submission. That's especially important for anesthesia because payer edits often center on claim integrity rather than on the code list alone.
If you're trying to tighten this process internally, a broader framework for medical billing denial management helps. But anesthesia groups usually need a narrower checklist built specifically around units, modifier logic, and bundling risk.
Clean claims are not created by luck. They come from a repeatable review process that prevents the same anesthesia errors from leaving the practice twice.
Practices that install those controls usually see cleaner first-pass performance, fewer preventable payer touchpoints, and faster cash conversion. Practices that don't often misread recurring denials as “just how anesthesia billing is.”
FAQs for Anesthesia Practice Owners
What is the biggest financial red flag in anesthesia billing right now
The biggest red flag is a practice that can't explain payment variance by time, modifier set, and staffing model. If leadership only sees total charges and total payments, significant leaks stay hidden. In our experience, the most expensive problems are the quiet ones: incomplete time capture, unsupported modifier use, and claims that pay without anyone checking whether they paid correctly.
Should we focus more on denials or underpayments
Underpayments deserve as much attention as denials. A denied claim is visible. An underpaid anesthesia claim often gets posted and forgotten, even when the documentation supported more. For owners, that means a low denial rate doesn't automatically mean healthy RCM. You need claim-level review logic that asks whether the payment matches the service, not just whether the payer responded.
How much should we worry about paperwork and intake workflow
More than most groups expect. Clean anesthesia billing starts before the case, not after it. Demographic errors, missing authorizations where required, and poor documentation handoffs create downstream billing friction. Standardized, HIPAA-compliant medical forms can help reduce intake inconsistency and documentation gaps that later slow claims, especially in multi-site or high-volume environments.
When is it time to audit or outsource anesthesia billing
It's time when leadership keeps seeing one or more of the same symptoms: cash arriving slower than expected, repeated modifier corrections, unexplained payer variation, or growing A/R tied to anesthesia claims that should have been straightforward. At that point, the question isn't whether your team is working hard. It's whether the workflow is built for anesthesia-specific reimbursement logic.
If you want a specialty-specific benchmark, compare your current process against an anesthesiology billing partner or request a free billing audit focused on units, modifiers, concurrency, denials, and payment variance. That kind of review usually quickly gets to the heart of the ownership question: are you dealing with isolated mistakes, or a system that leaks revenue by design?
Happy Billing helps physician practices tighten claim integrity, reduce anesthesia revenue leakage, and accelerate cash flow without forcing an EHR change. If your group needs a sharper view of where denials, underpayments, and aged A/R are coming from, Happy Billing is a practical place to start.