Pain Management CPT Codes: A Guide to Revenue & Denials
Most pain practices don't lose revenue because they chose the wrong pain management CPT codes. They lose revenue because the code, the note, and the payer rule don't line up. In this specialty, a claim can be technically coded and still be financially dead on arrival.
If you own a pain practice, this isn't a back-office detail. It directly affects denial rate, cash flow, and A/R days. Generalist billing teams often treat pain coding like standard office billing. That's a mistake. Pain management combines dense procedural coding, modifier-sensitive claims, and payer-specific medical necessity rules that punish sloppy documentation and weak follow-up.
Why Pain Management CPT Codes Are a Major Financial Risk
Pain management coding is a margin issue, not a paperwork issue. One wrong CPT code, one wrong level, or one missing modifier can turn a high-value procedure into a denial, a downcode, or a refund risk.
This specialty gives owners more financial exposure than general outpatient billing because reimbursement depends on procedural precision. Pain claims often rise or fall on exact code selection, spinal region, imaging guidance rules, laterality, diagnosis linkage, and payer-specific medical necessity standards. CMS publishes the underlying code set and descriptors for many of the procedures pain practices bill every day, including injection and neuraxial services, in its HCPCS and CPT code resources.
Generic billing teams miss that distinction. A family medicine workflow can absorb minor coding mistakes. A pain practice cannot. If your physician documents one service and your claim reflects a less specific or mismatched service, you lose money immediately and invite payer scrutiny on the next claim.
Where owners lose money first
Revenue loss in pain management shows up in a few repeatable failure points:
- Procedure detail is undercoded: The physician performs and documents a billable service, but the claim goes out with a narrower code that pays less.
- Code selection does not match the note: The record supports one spinal region, level, or approach, and billing submits another.
- Modifier use is weak: Claims lack the detail needed to support bilateral work, distinct procedural services, or separate E/M reporting when allowed.
- Authorization does not match the final claim: Staff obtains approval for one description, then the billed procedure varies enough to trigger denial.
- Denials sit too long: Payment slows, staff time shifts to rework, and A/R ages on services that should have paid cleanly the first time.
Owners should audit this chain, not just the final claim file. If your team is posting payments but not preventing repeat denials, your process is underbuilt for this specialty. Review your denial management workflow for medical billing and look for where preventable pain denials start. In many practices, the problem begins before the patient is seen, with scheduling, intake, diagnosis capture, or template design.
One hard rule applies here. In pain management, reimbursement is operational. Front desk, prior auth staff, clinical documentation, and coding all determine whether the payer sees a payable procedure or a claim to reject.
That is why owners who wait until remits arrive are already behind. Pain practices need front-end control over authorization language, diagnosis support, and procedure scheduling rules. If your current process is weak before the encounter starts, this guide on selecting prior authorization services is worth reviewing because it treats prior auth as revenue protection, which is exactly what it is.
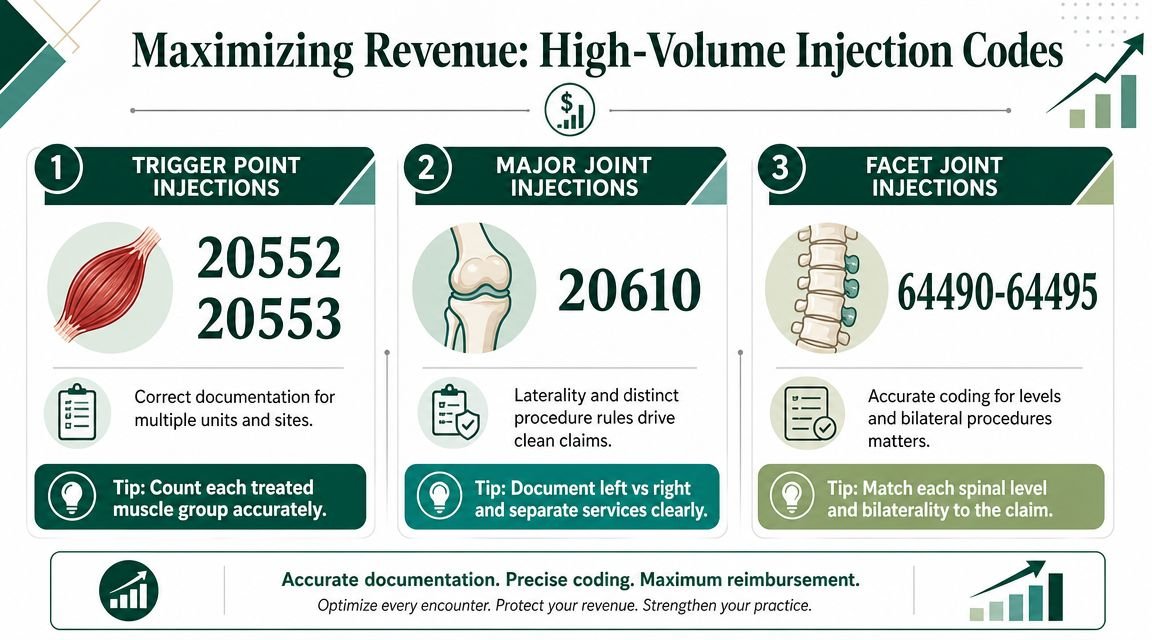
Securing Revenue from High-Volume Injection Codes
High-volume injection coding is where pain practices bleed cash. One wrong default in your workflow can underpay the same service dozens of times a month, and repeated documentation gaps turn routine injections into predictable denials.
Trigger-point injections prove the point. CPT 20552 is used for injections involving 1 or 2 muscles. CPT 20553 is used for 3 or more muscles. If the physician treated enough muscles for 20553 but your note template never captures muscle count clearly, your practice will keep billing the lower-paying code or invite denials when coders try to correct it. That is not a coding nuisance. It is a margin problem.
The injection codes owners should actually monitor
| CPT Code(s) | Procedure | Key Billing Nuance | Common Denial Reason / Revenue Loss |
|---|---|---|---|
| 20552, 20553 | Trigger-point injections | Code selection depends on whether 1 to 2 muscles or 3 or more muscles were treated | Undercoding when the note supports more muscles than billed, or denial when the muscle count is missing |
| 20610, 20611 | Joint injections | Payer review often turns on laterality, imaging support when required, and precise site documentation | Downcoding or denial when the note is vague about the joint, side, or technique |
| 62321, 62323 | Epidural injections | Higher scrutiny on diagnosis linkage and medical necessity support | Payment delay when the chart does not justify the intervention |
| 64490 to 64495 | Facet joint interventions | Level-specific coding and payer policy rules drive payment | Denial even with the right code if the record does not support the billed level or indication |
What to audit in your own reports
Start with frequency, then compare it to payment. A code that appears constantly but pays inconsistently deserves immediate review.
Look for these patterns:
- 20552 appears far more often than 20553: That usually means the physician template is weak, the coder is defaulting low, or both.
- 20610 and 20611 get edited often before submission: Your team likely has a site, laterality, or imaging documentation problem.
- Facet injections are billed regularly but collect slowly: The issue is often payer rule mismatch or poor level-specific documentation, not claim volume.
- One physician gets paid cleanly and another does not: Your revenue problem is probably inside the note, not inside the payer.
Review a sample of paid claims against denied claims for the same code and the same payer. You will usually find a pattern fast. One provider states the exact muscles treated, laterality, imaging guidance, and diagnosis link. Another provider documents the procedure in broad terms and leaves the billing team to guess. Guessing gets claims denied or downcoded.
Owners should also watch for silent underbilling. That is the revenue loss many generalist billers miss because the claim still gets paid. Paid wrong is still lost revenue.
If your practice performs occipital or peripheral blocks, review your coding rules against this guide to the occipital block CPT code and billing requirements. It is a good example of how a commonly performed injection can pay cleanly or create repeat write-offs depending on code selection and chart support.
Coding for High-Value Epidural and Nerve Block Procedures
High-value pain procedures do not guarantee high-value collections. Epidural and nerve block claims are some of the fastest ways for a practice owner to lose revenue on paper-correct coding.
The mistake is simple. Teams focus on the CPT range and ignore the payment trigger. Payers do not reimburse these cases because your scheduler marked “epidural” on the calendar. They reimburse when the claim, diagnosis, and procedure note line up with payer rules well enough to survive review. If that alignment fails, you get a denial, a downcode, or a payment delay that drags out A/R and ties up staff time.
Pain practices commonly bill 62321 and 62323 for epidural injections and 64400 through 64530 for nerve blocks. Those codes carry real revenue, which is exactly why they attract scrutiny. Owners should treat every one of these claims as a financial control point, not a routine charge ticket.
High reimbursement attracts high scrutiny
A clean code with a weak chart still produces bad cash flow. That is the part many generalist billers miss.
For epidural and nerve block procedures, payers expect the diagnosis to support the service, the target anatomy to be unmistakable, and the medical necessity story to make sense from start to finish. If the note says “back pain” and the claim bills a level-specific epidural without clear clinical support, your practice is asking for a denial. If the procedure note is vague about region, laterality, or nerve target, your billing team is left guessing. Guessing costs money.
Owners should watch these claims closely because the dollars at risk are larger than with routine office services. One preventable denial on a higher-paying injection is not just a billing issue. It becomes rework, appeal labor, delayed deposits, and often a write-off when the team cannot repair the record after the fact.
What your clinicians must document before the claim goes out
Do not accept generic procedure notes on these cases. Require documentation that supports payment without interpretation by the billing office.
Your chart should clearly show:
- A diagnosis that matches the procedure: The condition billed must support why this exact epidural or nerve block was performed.
- The precise treatment target: Document the spinal region, level, nerve, and laterality when applicable.
- The clinical rationale: The note should explain why the intervention was appropriate for this patient at this visit.
- Any required imaging or procedural detail: If payer policy expects imaging guidance or diagnostic support, the chart has to show it.
- A procedure note that matches the charge: The submitted CPT code should read like the natural result of the documentation, not a billing-office interpretation.
Effective documentation determines whether practices either protect margin or give it away. A physician who documents “lumbar epidural performed” creates billing risk. A physician who documents the diagnosis, level, approach, and supporting findings gives the claim a fair chance to pay the first time.
If your physicians are inconsistent on diagnosis specificity, tighten that process now. Use this guide to pain management ICD-10 coding and documentation logic to make sure the diagnosis side of the claim supports the procedure side.
High-value injection claims fail for ordinary reasons. Missing specificity, weak diagnosis linkage, and incomplete procedure details. Those ordinary mistakes create very expensive revenue loss.
Practice owners do not need to memorize every rule in the CPT book. You do need to know when your documentation standard is too weak to support the revenue your physicians are producing. On epidural and nerve block claims, weak notes turn strong production into slow cash.
Navigating Neurostimulation and Device Reimbursement
Neurostimulation cases expose whether your revenue cycle is disciplined or fragile. These claims carry more financial friction than routine injections because the risk starts before the procedure date. If the authorization packet, medical necessity file, and implant documentation aren't tight, your cash flow can take a serious hit.
Practice owners often treat device reimbursement as a coding problem. That's too narrow. It's really a workflow control problem involving scheduling, payer communication, clinician documentation, and claim assembly.

Where practices lose control
For neurostimulation and implantable pain procedures, owners should watch for three operational failures.
First, the authorization request is often incomplete. Staff submit a basic clinical summary when the payer expects a much more developed record. That creates delays, repeated requests for records, or a denial before the patient even reaches the facility.
Second, the documentation chain breaks between clinical evaluation and surgery scheduling. A provider may document the rationale well in one note, but the final packet lacks the exact elements the payer asked to review.
Third, the claim itself doesn't mirror the approved service description. Even when the procedure was appropriate, discrepancies between approved language and billed language can trigger payment holds.
What a disciplined workflow looks like
A stronger process usually includes these checkpoints:
- Before scheduling: Confirm the payer's current prior authorization criteria and required records.
- Before submission: Verify that the physician note, supporting evaluations, and any device-related documentation all tell the same story.
- Before claim release: Reconcile the final operative documentation against the authorization record so the billed service matches what was approved.
Owners should also insist on a single accountable person or team for pre-service reconciliation. When scheduling blames billing, billing blames clinical staff, and clinical staff blames payer rules, nobody owns the denial.
The most expensive denied claims are often denied long before the remittance arrives. The failure happened in intake, auth, or record assembly.
For a pain practice, that means neurostimulation revenue should be managed like a project, not processed like a routine office visit.
Maximizing Chronic Pain Management Revenue
Many pain practices still ignore chronic pain management revenue because it doesn't look like traditional procedural billing. That's a mistake. If your clinicians and care team already spend time managing chronic pain patients between visits, you may be leaving legitimate recurring revenue unbilled.
CMS implemented a chronic pain management framework after the SUPPORT Act. Under that framework, HCPCS G3002 covers the initial 30 minutes of monthly chronic pain management and G3003 covers each additional 15 minutes, as described in this CMS chronic pain management overview. The bundled service includes diagnosis, assessment, care planning, medication management, counseling, and care coordination. The initial visit is not billed separately as an E/M service under the program rules in that framework.
Why this matters to owners
This is not side revenue. It's a way to monetize structured monthly care that many practices already deliver informally.
The financial upside depends on process discipline:
- Time has to be tracked monthly: This is not a single-encounter mindset.
- Required service elements have to be documented: If the record lacks care planning, assessment, or coordination support, the claim gets weak fast.
- The team must capture cumulative work, not just face-to-face time: Otherwise you underbill work you already performed.
How to operationalize G3002 and G3003
The 2025 coding update described G3002 as the monthly base bundle and G3003 as the add-on for each additional 15 minutes, with the bundle including diagnosis, validated pain-rating assessment, care-plan development and revision, medication management, counseling, crisis care, and coordination with behavioral health and other practitioners, according to this chronic pain management coding update. That same guidance makes the operational shift clear. Documentation has to move from a single encounter focus to monthly cumulative time and service-element capture.
For owners, the recommendation is simple:
- Build a monthly CPM tracking workflow inside the EHR.
- Standardize note templates around the required service elements.
- Audit whether your staff are accumulating time correctly across the month.
- Stop letting clinically meaningful follow-up work disappear into nonbillable labor.
If your current billing partner only knows procedural pain claims, they may completely miss this revenue category.
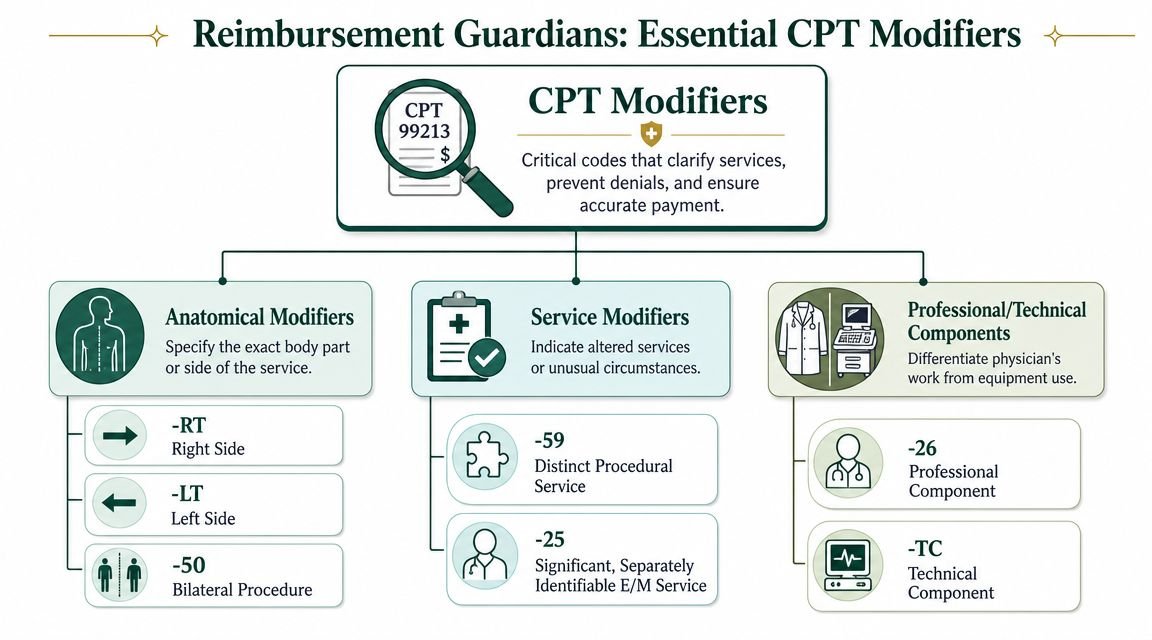
Essential Modifiers That Protect Your Reimbursement
Modifiers are revenue controls. Treating them as coding trivia is how practices get paid for half the work, or not at all.
In pain management, a clean claim often depends on whether the modifier tells the payer exactly what happened. Owners don't need to memorize every modifier in the CPT universe, but they do need to know which ones materially affect reimbursement visibility.
The modifiers that usually matter most
Here's the owner-level view:
- Modifier 25 supports a significant, separately identifiable E/M service on the same day as a procedure when the documentation supports both.
- Modifier 59 may be used to show a distinct procedural service when payer edits would otherwise bundle the work.
- Modifier 50 is central when the service was bilateral and payer policy allows bilateral reporting in that manner.
- RT and LT identify side-specific services and can be decisive for clean adjudication.
Why missing modifiers cost real money
A claim without the needed modifier doesn't just risk a denial. It can trigger partial payment, bundling, or payer edits that force your staff into manual rework.
Here's how that usually plays out:
| Modifier | Revenue function | What goes wrong without it |
|---|---|---|
| 25 | Separates a billable E/M service from the procedure when documentation supports both | The visit gets bundled and your practice gives away physician work |
| 59 | Identifies a distinct procedural service when edits would otherwise combine services | A legitimate additional service may deny as included |
| 50 | Signals bilateral performance when payer rules call for bilateral reporting | The claim may pay as though only one side was treated |
| RT/LT | Clarifies laterality for side-specific services | Claims stall, deny, or require correction because the service lacks anatomical clarity |
| 26/TC | Distinguishes professional and technical components when relevant | Payment can go to the wrong component or deny for duplicate billing logic |
Don't assume your billing team applies these consistently. Review claims by physician and by payer. Some teams apply modifiers correctly for one carrier and miss them for another because they rely on habits instead of policy review.
Owner check: If you see recurring bundling denials or corrected claims on routine procedures, modifier discipline is one of the first places to investigate.
If you're cleaning up modifier usage more broadly, this reference on the GY modifier meaning and payer implications is a useful reminder that modifier selection affects both compliance and payment logic.
Creating Documentation That Satisfies Payer Scrutiny
Documentation decides whether your high-value pain procedures turn into cash or avoidable write-offs. A clean claim with a weak chart still loses.
For spinal pain procedures, payers expect the chart to prove medical necessity, not merely name a CPT code. If your physician bills an epidural steroid injection or facet work in the CPT 64490 to 64495 range, the record needs a coherent history, exam findings, and imaging support that match the intervention. Owners who treat documentation as a back-office detail end up funding denials, appeals, and staff rework out of their own margin.
What a payer-ready note actually includes
A defensible pain procedure note has four jobs. It identifies the pain complaint with enough specificity to sound like a real patient, not cloned text. It ties physical exam findings to the planned intervention. It shows imaging or other diagnostic support that agrees with the target area. It explains why this procedure was reasonable for this patient on this date.
Miss one of those elements and the claim becomes expensive to collect.
That is why your templates need discipline. The right template prompts site, laterality, prior conservative care, functional impact, and objective findings. The wrong template creates a polished denial packet for the payer because every note looks copied, vague, or internally inconsistent.
Weak notes create direct revenue loss
Coding staff cannot bill their way out of poor physician documentation. If the chart says "low back pain" and little else, the biller has no credible support for a procedure that will draw scrutiny. If imaging points one way and the procedure note points another, expect an ADR, a denial, or a refund request later.
This problem gets worse in multi-provider groups. One physician documents diagnosis rationale, failed conservative treatment, and fluoroscopic guidance consistently, so claims move. Another leaves gaps, and the practice burns staff hours chasing records, correcting claims, and filing appeals that should never have existed. That variance is not a clinical style issue. It is a revenue control failure.
Pre-service approval also depends on chart quality. If your team wants fewer last-minute cancellations and fewer post-service denials, tighten the clinical record before the date of service. This guide to what prior authorization means in healthcare operations is a useful reminder that authorization and documentation are part of the same payment process.
A related lesson shows up outside physician claims too. DME Superstore's Medicare claims information highlights the same rule Medicare applies everywhere. Payment follows complete supporting records and correct process, not good intentions.
Standardized documentation protects revenue twice. It improves first-pass payment and cuts the labor cost of fixing denials after the fact.
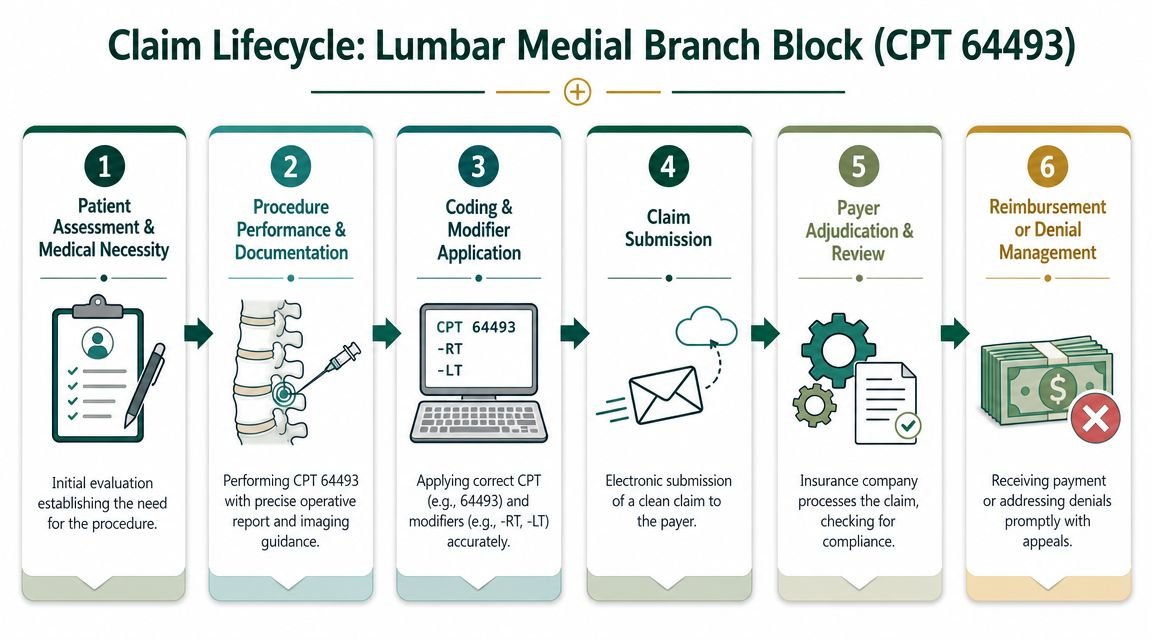
Anatomy of a Perfect High-Value Pain Management Claim
The cleanest way to judge your RCM is to trace one claim from decision to payment. Consider a lumbar medial branch block billed with CPT 64493. When this claim pays smoothly, it's rarely because one person did something heroic. It's because every step matched.
What the strong claim looks like
The visit starts with a documented pain complaint, exam findings, and imaging support that line up with the planned intervention. The physician's record identifies the target area clearly enough that the claim can support 64493 without ambiguity. If side-specific reporting applies, the claim includes the appropriate laterality detail.
The diagnosis linkage also has to make sense. Some practices use broad, nonspecific pain diagnoses too often. For a procedure like this, vague diagnosis reporting can weaken medical necessity and trigger review. The biller's job is not to rescue a weak chart. It's to translate a strong one accurately.
What the bad claim looks like
Now compare that with the claim most owners never see until it denies.
The schedule says medial branch block. The note is thin. Imaging support is missing from the assembled record. The claim goes out with the CPT code, but not enough context. The payer asks for records or denies for lack of necessity support. Staff rework follows. Payment slows. Your A/R ages for a claim that should have been clean the first time.
This is why denial prevention beats denial management. Appeals are necessary, but they're expensive.
For practices that also handle medication access issues alongside interventional claims, patient-facing claim friction can mirror what happens on the medical side. This resource on how to fight prescription claim denials is useful because it shows the same underlying truth. The earlier the documentation and coverage logic are fixed, the less downstream damage you create.
If you want to know whether your current billing operation is protecting or leaking high-value pain claims, compare one month of denied procedures against one month of operative notes and authorization records. That review usually tells the truth fast.
FAQs for the Pain Practice Owner
How do I know if my billing team actually understands pain management CPT codes
Look at denial patterns by procedure family, not just total collections. If epidurals, facet procedures, and injection claims repeatedly require corrections, your team may know basic billing but not specialty-specific pain reimbursement logic.
Should I blame denials on coding or documentation
Usually both interact, but documentation often causes the bigger problem in interventional pain. A correct code with weak medical necessity support still delays or kills payment.
Is chronic pain management worth building into my workflow
Yes, if your clinicians already perform ongoing monthly management work and your team can document cumulative time and required service elements correctly. Otherwise the work stays clinically real but financially invisible.
When should I consider outsourcing pain practice billing
Consider it when denials keep recurring on the same procedures, your physicians are answering repeated chart queries, or your A/R keeps stretching because your current team reacts after denials instead of preventing them. If you want to compare your current process against a specialty-focused model, review pain management billing support for specialty practices and request a free revenue cycle audit to identify where claims are leaking before another month of procedures goes underpaid.
If your pain practice is still treating coding, modifiers, and documentation as separate tasks, you're almost certainly losing revenue in the gaps between them. Happy Billing helps specialty practices tighten that entire chain, from clean claim setup to denial prevention and A/R recovery, so high-value pain claims don't stall for avoidable reasons.