Claim Denial Management: The Practice Owner’s Guide

If your practice is collecting slower, writing off more, or watching A/R age without a clear reason, claim denial management is usually where the money is leaking. It's the system for preventing denials before claims go out, fixing the ones that still hit, and turning denial patterns into operational changes that protect revenue.
Most owners don't have a denial problem. They have a workflow problem that shows up as denials. When registration misses coverage details, when authorization tracking lives in sticky notes, or when documentation doesn't support the CPT billed, payment slows down and staff time gets burned reworking claims instead of collecting clean ones.
What Is Claim Denial Management and Why It Is Costing You
Claim denial management is the process of identifying why a payer refused or reduced payment, correcting what can be fixed, appealing what should be challenged, and changing upstream workflows so the same denial doesn't keep repeating.
That sounds administrative. It isn't. It's a direct profitability issue.

In hospital revenue cycle operations, the average cost to rework a single denied claim is $25 to $118, and 50% to 65% of denied claims are never appealed, according to Advantum Health's denial management analysis. Even if your practice is smaller than a hospital system, the lesson is the same. Every denial creates two losses at once. You lose time, and you delay or abandon cash you already earned.
Denials are not a back-office nuisance
Owners often focus on the visible symptoms first: rising write-offs, unexplained patient balance growth, or providers asking why a paid procedure still sits in A/R. Denials sit underneath all of that. They push revenue out, increase labor, and hide process failures across scheduling, front desk intake, authorizations, coding, and follow-up.
A useful way to think about it is this. A denial is not one event. It is a chain of avoidable work:
- The original failure: bad eligibility data, missing authorization, wrong modifier, unsupported diagnosis, duplicate submission, or filing error
- The rework cost: staff has to research the ERA or EOB, gather documents, correct the claim, call the payer, or draft an appeal
- The cash delay: payment moves deeper into A/R, often past the point where collections stay efficient
- The final leak: some claims never get touched again, especially low-dollar claims or denials that no one owns
Practical rule: If your team only sees denials as billing cleanup, you'll keep paying to fix the same mistake multiple times.
Where practice owners usually misread the problem
A practice can have a billing team that “works denials” all day and still perform poorly. That's because effort isn't the same as control. Strong claim denial management connects front-end prevention, payer-specific follow-up, and reporting that ties denials back to the exact workflow that caused them.
If you want the broader financial context, revenue cycle management in medical practices then stops being a back-office concept and becomes an operating system for cash flow.
For owners, the bottom-line question isn't whether denials happen. They will. The key question is whether your practice has a system that prevents the avoidable ones and works the recoverable ones before they become write-offs.
The Most Common Denials and Their Hidden Root Causes
Most denial reports are misleading because they describe the symptom, not the disease. “Patient not eligible” sounds like an insurance issue. It's often a scheduling issue. “Authorization required” sounds like a payer obstacle. It's often a tracking failure inside the practice.
Experian Health's 2025 survey found that 54% of providers said denials are increasing, 41% reported that at least one in ten claims is denied, and the top causes were missing or inaccurate data, authorization problems, and incomplete patient information, as reported in Experian Health's claims denial review. That matters because those are operational failures first.
Denial symptoms vs root causes
| Denial Reason (The Symptom) | Likely Root Cause (The Disease) | Where to Look |
|---|---|---|
| Patient not eligible | Coverage not verified at scheduling and again before date of service | Front desk, scheduling scripts, eligibility workflow |
| Authorization required | No centralized authorization log, expired auth, wrong service linked to auth | Referral team, pre-visit review, payer portal tracking |
| Missing information | Demographics, policy numbers, referring provider data, or accident details entered inconsistently | Registration, intake forms, data entry QA |
| Duplicate claim | Staff resubmitted before confirming claim status or posting lag made claim appear unpaid | Charge entry, claim status workflow, payment posting lag |
| Medical necessity denial | Documentation does not support diagnosis-to-procedure relationship | Provider documentation, coding review, payer policy checks |
| Modifier-related denial | Modifier used incorrectly, omitted, or applied without payer-specific logic | Coding edits, specialty billing rules, claim scrubber setup |
| Timely filing denial | Claims held in charge lag, credentialing delays, or unresolved front-end edits | Charge capture, enrollment status, held-claim work queues |
| Bundling denial | Procedure combination billed without proper modifier support or documentation | Coding review, NCCI edit awareness, operative note detail |
What the denial reason usually hides
A denial category by itself rarely tells you where to act. We've seen practices spend months coaching billers on appeals when the underlying failure sat at check-in. If patient demographics are captured inconsistently, no amount of downstream denial work will stabilize collections.
Take common procedural examples. Modifier 25 on an E/M with a same-day procedure can be legitimate, but if the note doesn't clearly support a separately identifiable service, you create avoidable payer friction. Modifier 59 can unblock distinct procedural services, but using it casually invites review and delay. For surgery and pain cases, global-period confusion and modifier 24 or 79 misuse can turn valid claims into preventable denials.
Denials should be grouped by who created the defect, not just by CARC text on the remittance.
That's why denial reporting has to move beyond denial code tallies. A useful owner-level dashboard asks better questions:
- Which payer is denying which service line most often
- Which provider or location generates repeat documentation-related denials
- Which front-end staff workflows correlate with eligibility or authorization issues
- Which modifiers trigger disproportionate rework
If you want a more tactical list of recurring denial categories, the most common medical billing denials are worth reviewing. But the significant gain comes when you stop asking, “What denial code did we get?” and start asking, “Which process inside the practice made this denial predictable?”
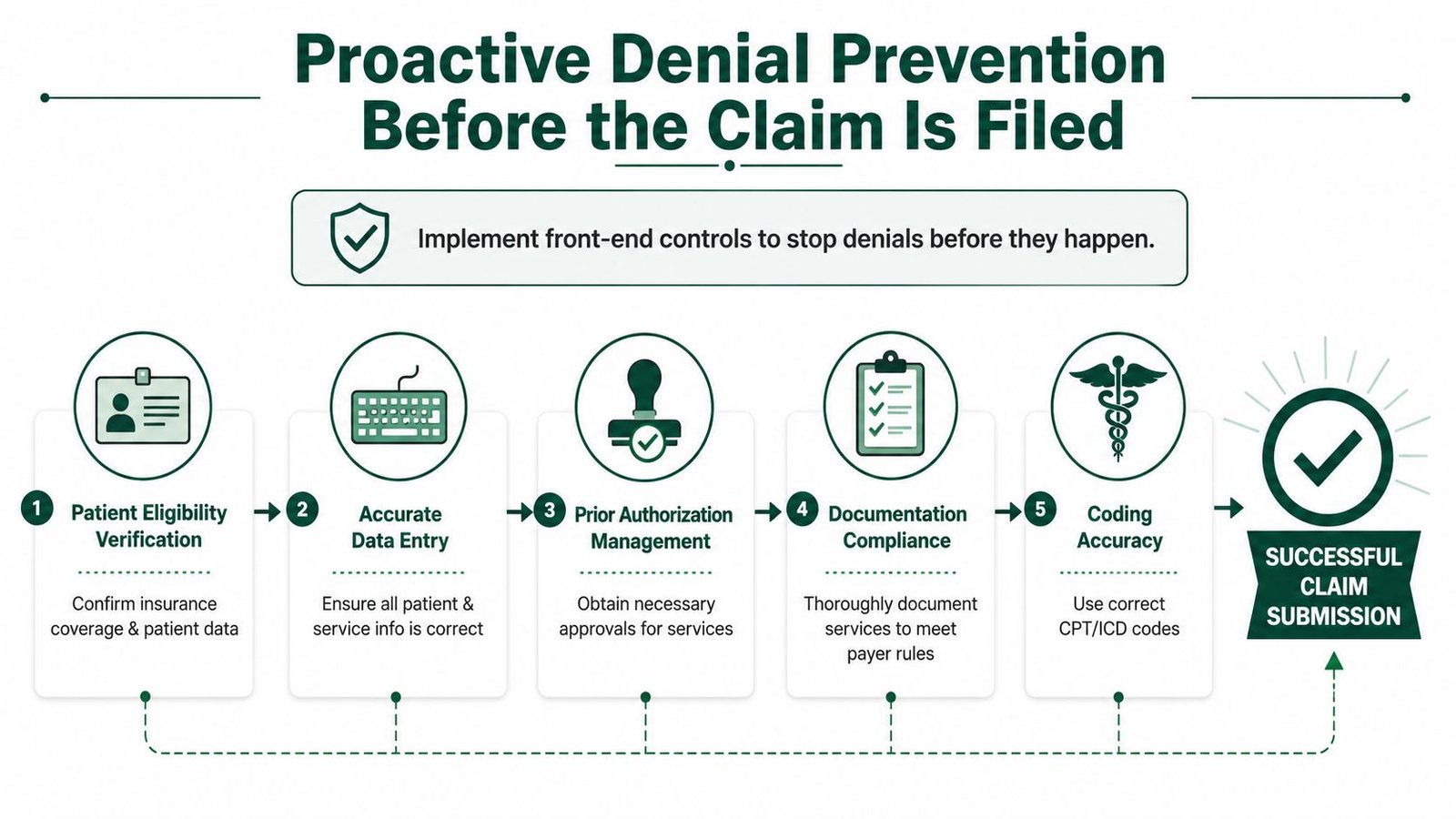
Proactive Denial Prevention Before the Claim Is Filed
Monday morning starts with a full schedule, a clean front desk, and providers seeing patients on time. Thirty days later, the cash is short because the actual failure happened before the visit closed. Eligibility was checked once instead of twice. The authorization covered fewer units than the procedure performed. The note supported the care, but not in the way that payer expects to see it. That is where denial prevention has the highest financial return.
Practices usually lose more money from preventable front-end defects than from difficult appeal cases. We see the same pattern across audits. Owners focus on rework after the ERA posts, while the larger margin gain sits upstream in scheduling, intake, authorizations, and pre-bill review. If the goal is fewer denials with less labor, start where bad claims are created.
Tighten high-risk intake points first
Front-end prevention is not about adding more clicks to every visit. It is about controlling the few fields that create the most downstream loss.
For most practices, those fields are insurance status, subscriber data, referral details, and ordering provider information. If any of those are wrong, the claim can fail before coding quality even matters. A useful benchmark is your practice's clean claim standard in medical billing, because it forces the team to define what must be correct before a claim leaves the building.
Three controls usually produce the fastest return:
- Run eligibility twice. Verify at scheduling, then verify again near the date of service.
- Use one demographic script. Names, DOB, member ID, group number, and subscriber relationship should be captured the same way every time.
- Validate referral and ordering data before the visit. Imaging, cardiology, therapy, and specialist claims often fail over missing or mismatched provider information.
A pediatric practice and an orthopedic group will not have the same intake risk. Pediatrics often sees coverage shifts and coordination-of-benefits issues. Orthopedics gets hit harder by referral, imaging order, and procedure authorization defects. The control point should match the specialty's actual loss pattern.
Treat authorizations like a revenue control process
Authorization work breaks down when ownership is vague. One person starts it, another follows up, a third schedules the case, and nobody confirms whether the approved CPTs, units, and date range still match the final plan.
That creates expensive denials on high-value encounters.
Use one source of truth for the auth number, approved services, units, servicing provider, and validity dates. Then require a final check whenever the plan of care changes. Pain management, GI, cardiology, and outpatient surgery are common problem areas because small service changes can push the billed claim outside the approved scope.
This is also an area where automation helps if it is tied to a disciplined process. Tools and AI employees can assist with status checks, follow-up tasks, and missing-data flags. They do not fix weak ownership. If the practice has not defined who updates auth details and who signs off before billing, the denial still happens.
Put a pre-bill stop on claims that predictably cause rework
Every claim does not need manual review. The high-ROI move is to intercept the claims your payers repeatedly challenge.
Common examples include:
- E/M visits billed with modifier 25
- Distinct procedure claims using modifier 59
- Post-op and related surgical claims involving modifier 24, 57, 58, 78, or 79
- High-cost diagnostic or interventional services where diagnosis support must clearly match the procedure billed
Those claims deserve a short pre-bill review for documentation support, coding logic, and payer-specific edits. Family medicine may need tighter review of same-day E/M and procedure combinations. Interventional pain often needs closer review of laterality, units, and authorization alignment. General surgery usually needs stronger controls around global periods and related follow-up services.
A good prevention workflow interrupts risky claims before submission and leaves routine claims alone. That trade-off matters. If every encounter goes through a heavy review queue, staff cost rises and charge lag gets worse. If no risky claims are screened, denial volume rises and cash slows down. The right model is selective friction where the dollars justify it.
Building a Disciplined Denial Remediation Workflow
Even the strongest front-end process won't eliminate every denial. Payers change edits, policies shift, and some claims require payer-specific defense. What matters is whether your team works denied claims with discipline or just reacts to whatever appears oldest in A/R.
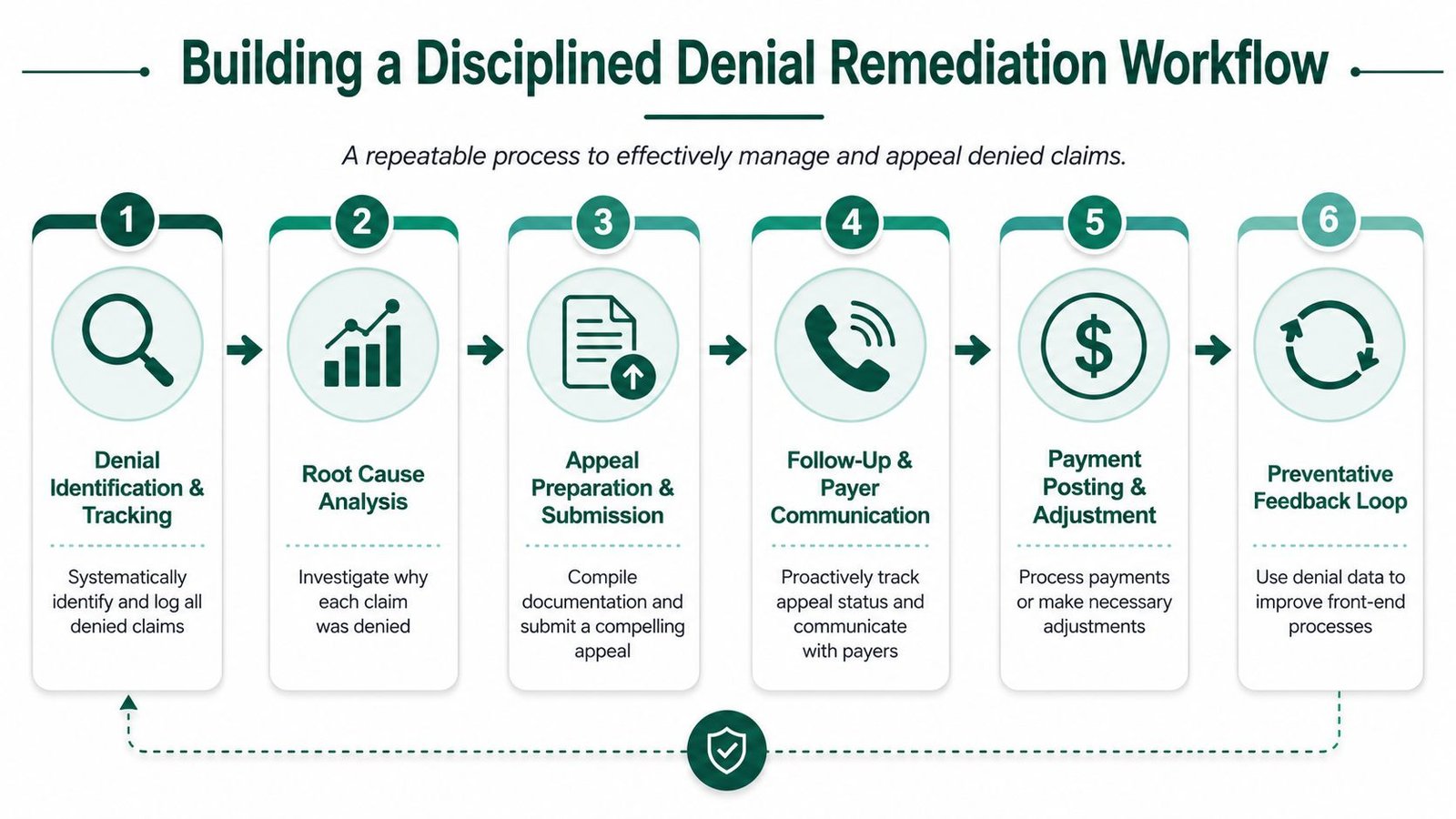
Stage one, triage by value and winnability
The biggest mistake we see is treating all denials equally. A low-balance claim with weak documentation should not consume the same staff time as a high-value claim with a clear correction path.
Start with three filters:
- Dollar value: Higher-value claims deserve faster review.
- Appeal deadline: Claims near filing limits move up.
- Correctability: Some denials need a simple corrected claim. Others require records, provider input, or policy support.
If the team's work queue is sorted only by oldest date, you'll often recover less money with more labor.
Stage two, research the real denial path
Once a claim is triaged, the next question is simple. Is this a correction, a reconsideration, or a formal appeal?
That distinction matters. A duplicate denial may require status verification and internal cleanup. A modifier denial may require coding correction and resubmission. A medical necessity denial may require chart support and payer policy comparison.
For practices evaluating automation support, the most useful tools aren't the ones that promise magic. They're the ones that reduce repetitive status checking, deadline tracking, and documentation routing. That's why some groups are exploring workflow support such as AI employees to handle repetitive admin work while experienced staff focus on payer judgment calls.
Stage three, act fast and document everything
A denial workflow fails when staff keep the next step in their heads. Every denied claim should show owner, due date, denial reason, current status, and required documents.
Good remediation usually looks like this:
- Corrected claims: Fix the error, validate the correction, and resubmit with proof the issue was addressed
- Appeals: Attach the exact records that answer the denial, not the entire chart dump
- Payer calls: Log representative name, date, reference number, and next action
- Provider tasks: Ask for a specific addendum or clarification, not a vague “please review”
Stage four, feed denials back into operations
A denial resolved without process change is wasted learning. If multiple claims deny for authorization mismatch, the auth workflow needs redesign. If a payer repeatedly rejects modifier 25 on specific visit types, someone should review note structure, charge review, and payer policy alignment.
For owners who need a tactical framework for the appeal side, how to appeal a denied insurance claim is useful. But the bigger operational point is this. Denial remediation should produce fewer future denials, not just more reopened claims.
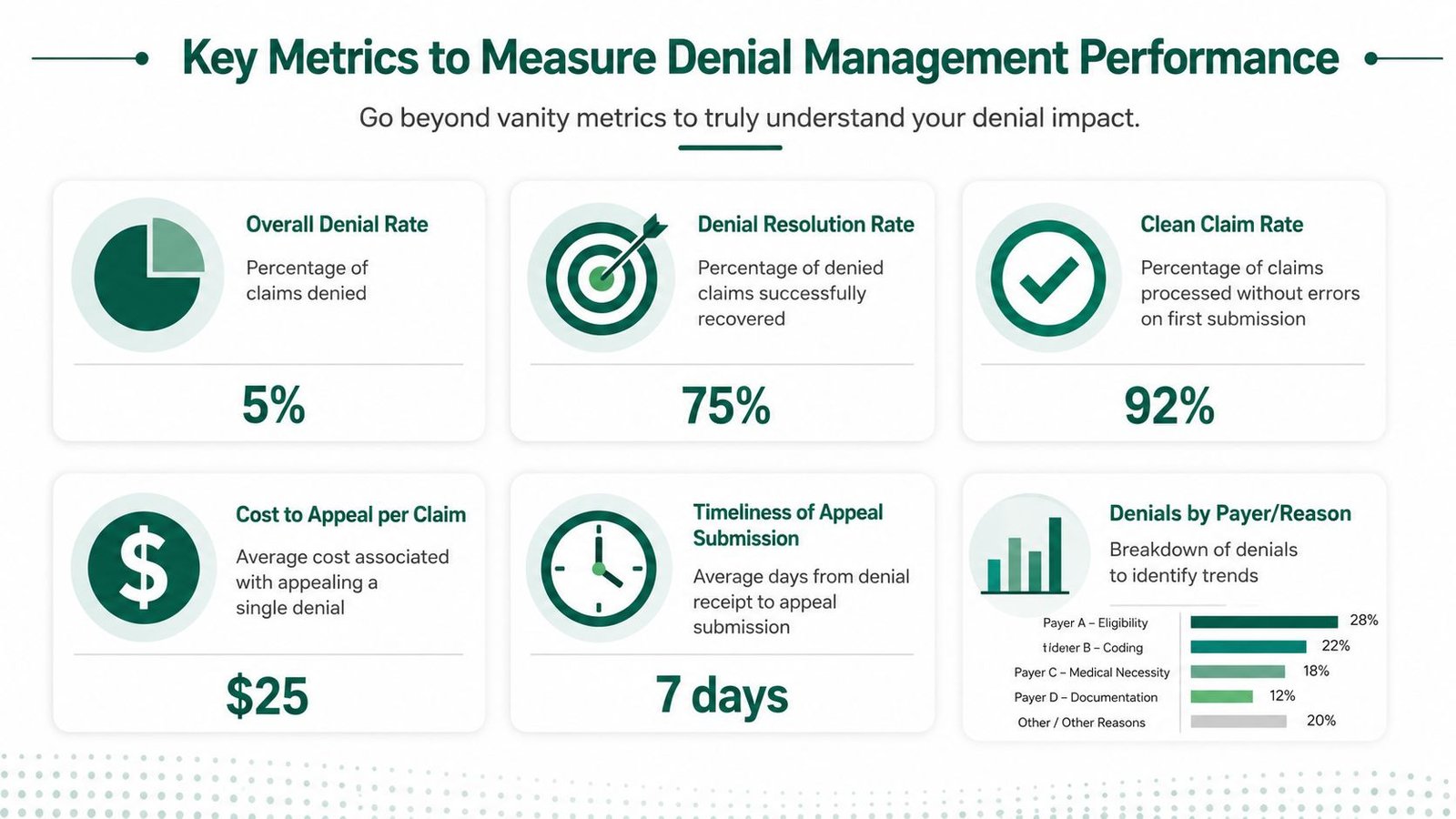
Key Metrics to Measure Denial Management Performance
A low denial rate can still hide a weak revenue cycle. Teams can suppress reported denials by writing claims off too early, underbilling conservatively, or avoiding hard-to-defend services. None of that helps the owner.
HFMA recommends tracking initial denial rate, appeal rate, and win/loss ratio together, because looking at a single metric by itself can mislead decision-makers, as explained in HFMA's guidance on denial measurement.
Stop using denial rate as a vanity metric
Owners should care about denial rate, but not in isolation. A practice with a moderate denial rate and excellent recovery discipline can outperform a practice with a superficially lower denial rate and poor follow-up.
The more useful dashboard includes:
- Initial denial rate: How many claims fail the first pass
- Appeal rate: Whether your team is pursuing recoverable claims
- Appeal win/loss ratio: Whether the appeals being worked are strong
- Days in A/R: Whether denials are slowing total cash conversion
- Clean claim rate: Whether the front end is producing payable claims
- Net collection performance: Whether expected reimbursement is coming in
Metrics should answer management questions
Each metric should tell you where to intervene.
If initial denials rise but appeal wins stay healthy, prevention is weak but remediation may be fine. If denials are stable but A/R worsens, follow-up speed or payment posting may be the issue. If appeal activity is low, the team may be abandoning recoverable revenue.
This is similar to support operations. Looking at one surface metric rarely tells the whole story. Some of the best thinking on balanced KPI design comes from outside healthcare too, such as Halo AI's customer support insights, which show why single-metric management usually creates blind spots.
What owners want is not more reporting. They want a dashboard that tells them who is losing money, where, and whether the fix belongs at the front desk, in coding, or in follow-up.
If you're holding an in-house team or outsourced partner accountable, medical billing KPIs worth tracking should be tied to cash outcomes, not just activity counts.
Specialty-Specific Denial Challenges and Solutions
Generic denial advice breaks down fast in specialty care. The denial may arrive in billing, but the cause often starts with the clinical workflow, documentation pattern, or payer rule that is unique to that specialty.
For specialties such as behavioral health and imaging, denial causes often originate upstream from the claim itself. Payer rule volatility and missing prior authorizations can create large batches of avoidable denials, which makes front-end workflow design more important than back-end appeals, as discussed in CGM's denial management focus areas.
Anesthesiology
In anesthesia, owners often underestimate how much denial exposure sits in unit reporting, modifiers, and concurrency logic. CPT 00140 is a good example of a code where payment depends on more than just charge entry. If time documentation is inconsistent, if physical status modifiers are missing where supported, or if concurrency is reported incorrectly, payers may reduce or deny payment without the issue looking dramatic on the surface.
The fix is rarely “train billing harder.” It's tighter anesthesia record capture, charge review against the anesthesia log, and payer-specific checks before submission. Practices dealing with those issues should review a specialty-specific workflow such as anesthesiology billing support.
Cardiology
Cardiology groups face a different pattern. A claim for CPT 93458 may be billed correctly from a coding standpoint, but still deny when the documentation doesn't clearly support medical necessity or when related imaging and interventional details aren't aligned with payer expectations.
We've seen this happen when the procedure note is clinically sound but not structured for reimbursement defense. The owner experiences it as longer A/R and heavier appeal volume. The key is coordinated review between provider documentation, coding edits, and payer policy interpretation. For that environment, cardiology billing services are more relevant than generic multispecialty advice.
Mental health and behavioral health
Behavioral health clinics often lose money before the claim is even built. Session limits, authorization expirations, and payer-specific visit rules can invalidate an entire run of claims when the schedule keeps moving but the authorization record doesn't.
The billing team then inherits a denial stack that looks like a payer issue. It's not. It's an authorization operations issue. In that setting, mental health billing services should be built around auth tracking and benefit control, not just claims follow-up.
The owner's takeaway is straightforward. Denials are specialty-specific leaks. If your billing model treats anesthesia, cardiology, and behavioral health as basically the same, you're probably losing money in ways the aging report won't explain clearly.
FAQs on Claim Denial Management
Should we handle claim denial management in-house or outsource it
The right answer depends on control, speed, and cost to collect.
Keep denial work in-house when your team owns the full chain. Scheduling captures clean insurance data, authorizations are current, coding is specialty-aware, and a manager reviews denial trends closely enough to change upstream workflows. In that setup, in-house management can protect margin because the people fixing the problem sit close to the people creating it.
Outsource when denials keep repeating, appeal queues age out, staff turnover keeps resetting performance, or the owner is acting as the unofficial denial manager. We usually find that outsourcing pays off when the practice does not have the volume, leadership depth, or payer expertise to run a disciplined process internally.
What is a good denial rate for a medical practice
A denial rate only matters in context. Specialty, payer mix, visit type, and documentation burden all change the baseline.
We put more weight on avoidable denial dollars than on the headline percentage alone. A practice with a modest denial rate can still be losing substantial cash if high-value claims are getting denied for authorization, medical necessity, or modifier issues. A practice with a higher denial rate may be in better shape if denials are low-dollar, corrected quickly, and rarely hit final write-off.
Track trend, dollar exposure, overturn rate, and time to resolution together. That shows whether denial management is protecting cash or just generating activity.
Is AI actually useful in claim denial management
Yes, if it is assigned the right work.
AI is useful for queue routing, pattern detection, status follow-up, and identifying recurring edits by payer or CPT. It can reduce manual sorting and help teams focus on claims with the highest recovery value first.
It does not replace specialty judgment. It will not fix weak documentation, poor front-desk intake, or a bad appeal argument. The best financial result comes from pairing automation with experienced billers, coders, and managers who know which denials should be corrected, appealed, or written off quickly.
What should I do first if denials are hurting cash flow right now
Start with denied dollars, not denial counts.
Pull a recent set of denied claims and rank them by payer, denial reason, service line, and total dollars at risk. Then trace each category back to the point of failure. We often see the biggest losses tied to a small number of operational breakdowns such as expired authorizations, specialty-specific coding errors, missing documentation support, or weak follow-up discipline.
The question to answer first is simple: where is the practice losing money?
If your practice needs that answer, Happy Billing can help identify the denial patterns and workflow failures draining cash. Their team focuses on independent practices that need practical fixes, faster collections, and tighter front-end controls without rebuilding the entire operation.