Maximize Out of Network Reimbursement in 2026
Out of network reimbursement can be a meaningful revenue opportunity, but only if you manage it like a financial strategy instead of a billing afterthought. The risk is larger than many owners realize. In a major analysis of large employer health plans, almost 18% of inpatient admissions included at least one claim from an out-of-network provider according to KFF Health System Tracker, which means this issue touches routine care and can directly inflate denials, slow cash flow, and lengthen A/R.
A practice that handles out of network claims casually usually pays for it in three places. The first hit is underpayment because the team never verified the plan's reimbursement logic. The second is rework because the claim went out with weak documentation. The third is aged receivables because nobody owns the appeal path once the payer issues a low allowed amount or denial.
Owners who understand the mechanics can protect margin. Owners who don't often confuse a paid claim with a properly paid claim.
What Is Out-of-Network Reimbursement
Out-of-network reimbursement can either protect margin or drain it. The difference usually comes down to whether the owner treats OON billing as a series of revenue decisions, or leaves it to staff to sort out claim by claim.
Out-of-network reimbursement is the amount a health plan pays when your practice has no participating contract with that payer for the service billed. That definition is straightforward. The business impact is not. Payment terms are less predictable, patient responsibility is harder to estimate, and underpayments require active follow-up if you expect to collect what the case is worth.
The key issue for an owner is control. In a contracted relationship, the fee schedule sets the frame for expected payment. In an OON relationship, the payer often applies its own reimbursement method, then leaves the practice to decide whether to accept the amount, bill the patient when allowed, appeal, or pursue a higher recovery through other channels. Each choice affects cash flow, staff time, and A/R days.
That is why OON reimbursement belongs in the same conversation as pricing, intake, documentation, and collections.
Why owners should care
Practices rarely lose money on OON claims because the service should never have been billed. They lose money because the financial ground rules were weak before the visit, the chart did not support the level of service, or nobody recognized that the payer's payment method made the case worth fighting.
A $3,000 underpayment is not just a posting issue. It is a decision point. The practice can write it off, assign staff to appeal it, shift the balance to patient collections if plan rules allow, or send the account to a specialist who handles OON disputes every day. Owners who make those choices intentionally usually keep OON A/R under control. Owners who do not often end up with old balances that consume staff time and never convert to cash.
Newer administrators may need a basic explanation of in-network vs. out-of-network care. Owners need a more practical view. Network status changes how you estimate, how you document, how you pursue payment, and how much effort a claim deserves after the first remittance.
If your team needs broader context, this overview of revenue cycle management fundamentals is useful. OON performance usually reflects the discipline of the larger revenue cycle.
Owner's lens: Out-of-network reimbursement is a payment strategy issue first, and a billing task second.
Where practices lose margin
Margin usually slips in a few predictable places:
- Pre-service financial clearance is incomplete. Staff verify active coverage but do not confirm whether the specific provider, location, or service is outside the plan network.
- The practice accepts the first payment without analysis. Low allowed amounts get posted and closed even when the payer used a weak or questionable reimbursement basis.
- Documentation does not support the fight. Records may support medical necessity clinically, but not in the format needed for an appeal, reconsideration, or independent review.
- High-value claims get the same follow-up as low-value claims. A $400 shortfall and a $12,000 shortfall should not get the same workflow.
- Nobody owns the escalation path. Once a payer issues a denial or low payment, the account sits in aging because responsibility is split across front desk, billing, and management.
The owner question is simple. Which claims are worth internal effort, which claims need a formal payment dispute, and which claims should be handed off to a partner with the staff and payer expertise to pursue them efficiently?
That is what out-of-network reimbursement really is in practice. It is not just what the payer sends. It is the amount your business can recover after you decide how hard to push, how well to document, and how long to keep the account in-house.
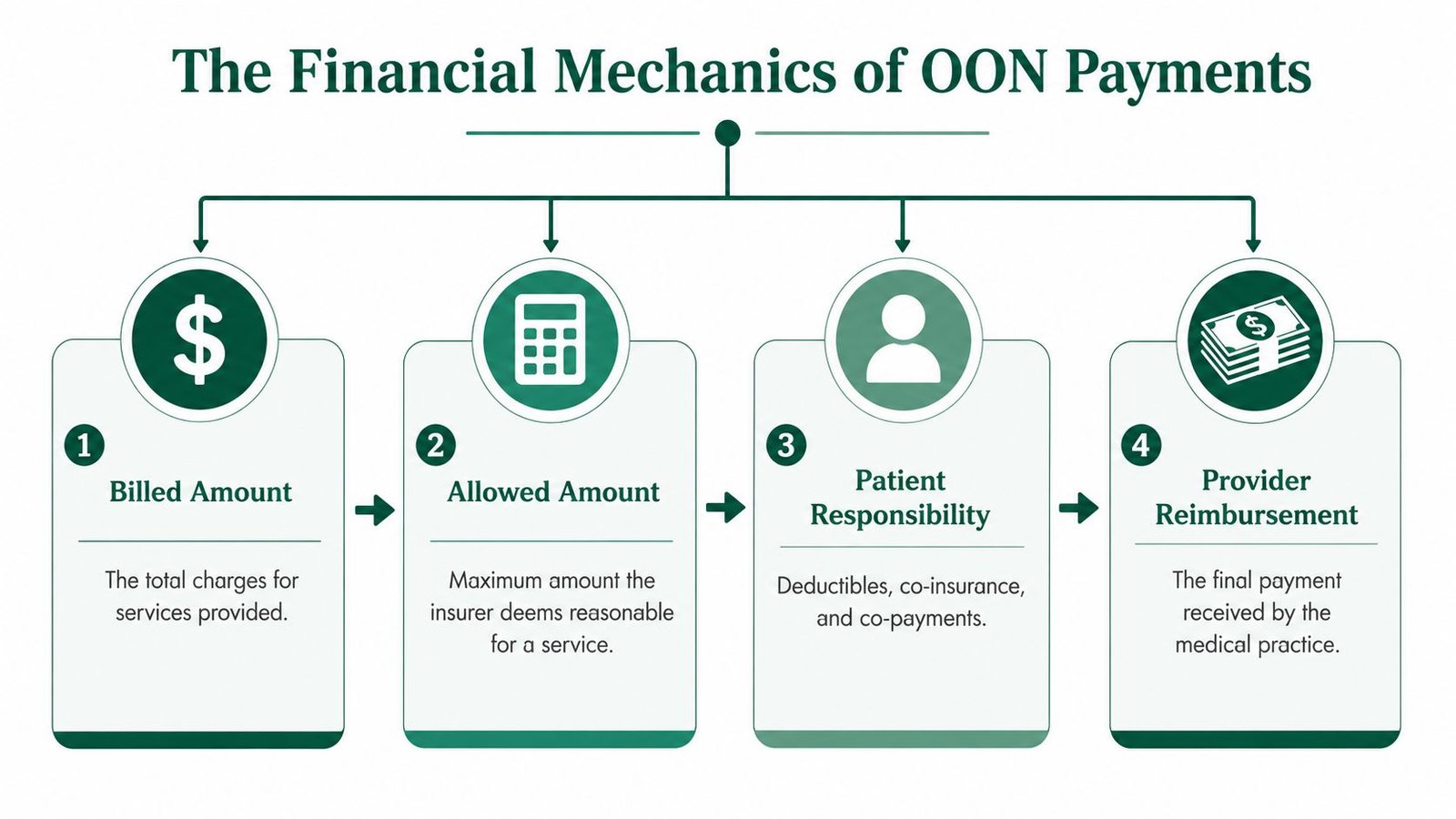
The Financial Mechanics of OON Payments
The core financial issue in out of network reimbursement is the gap between your billed amount and the payer's allowed amount. Owners often focus on charge entry because that's the visible number. The payer doesn't. The payer starts from its own benchmark, then applies plan terms, then calculates what the practice and patient may each receive or owe.
Billed amount is not the economic reality
Think of your billed charge like a sticker price. It matters, but it does not control what the plan will recognize. Many owners find this out only after a high-value claim comes back paid at a fraction of expectations.
FAIR Health explains that many plans calculate out-of-network reimbursement using a percentage of usual, customary, and reasonable (UCR) charges for the geographic area, while others use a percentage of the Medicare fee schedule. That means the exact same CPT code can generate very different payment outcomes depending on the plan.
How the math usually works
A practical way to think about it is this sequence:
| Step | What happens | Why the owner should care |
|---|---|---|
| Charge entry | The practice bills its full fee | Sets the opening position, but not final reimbursement |
| Allowed amount determination | The payer applies UCR or a Medicare-based formula | This is where most revenue compression happens |
| Patient cost share | Deductible, coinsurance, or copay is applied under the plan rules | Bad estimates create collection problems and complaints |
| Net payer payment | The payer issues payment based on its allowed amount | This determines whether appeal work is worth the labor |
Here's a non-numeric example using common coding logic. A specialty encounter might include an office or facility E/M service, a procedure code, and an add-on supply or imaging-related component if payer rules allow it. Your practice may bill each line at your standard fee schedule. The plan may then reduce one line under a Medicare-based benchmark, deny another for bundling, and apply patient cost sharing to the remaining allowed amount. The final payment can be directionally far below what your billing team expected, even when the claim was technically processed.
That is why owners need line-level visibility, not just claim-level visibility.
A paid OON claim can still be the wrong payment if the payer used the wrong benchmark, applied the wrong reduction logic, or ignored documentation that supported separate reimbursement.
When we review EOBs, we look first for the payer's methodology. If the remittance doesn't clearly explain the basis for the allowed amount, the practice is already at a disadvantage. This guide to reading an explanation of benefits is helpful for administrators who need to train managers to spot underpayments before they drift into write-offs.
Why code-level detail matters
Owners don't need to become coders, but they do need to know where money is commonly won or lost.
- E/M selection: If the record supports a higher-level service but the claim goes out conservatively, you've reduced your own ceiling before the payer even starts.
- Modifier use: Modifiers such as 25, 59, 76, or RT/LT can materially affect whether separately reportable services survive payer edits, depending on the scenario and payer policy.
- Anesthesia and time-based billing: Missing units, concurrency support, or required modifiers can turn a collectible claim into a manual-review file.
Navigating the No Surprises Act and Legal Landscape
The No Surprises Act changed more than patient billing. It changed workflow, documentation standards, dispute strategy, and the amount of internal attention an out-of-network claim can demand before you see cash.
For owners, the immediate operational issue is that legal protection from balance billing does not automatically create smooth reimbursement. The claim still has to be submitted correctly, the payer still makes an initial payment decision, and any disagreement still enters a formal process with deadlines and documentation expectations.
Where the law helps and where operations still fail
The legal framework matters most in emergency services, certain out-of-network services at in-network facilities, and other protected settings. In those situations, owners need to know when a patient balance is legally off the table, when notice-and-consent rules may apply, and when a reimbursement dispute belongs in a statutory process rather than a routine appeal queue.
One of the most useful real-world examples comes from state guidance. New York has clarified that if a health plan gives inaccurate network-status information, it may have to reimburse the provider for out-of-network services accordingly, as described in New York's guidance on state and federal surprise billing rules. For owners, that means call logs, portal screenshots, and verification notes can become revenue-critical evidence.
What QPA and IDR mean for A/R
Owners hear QPA and IDR often, but many practices still treat them as legal jargon. They are operational terms.
- QPA: The qualifying payment amount influences disputes in protected claims.
- IDR: Independent Dispute Resolution is the formal process for challenging the payment amount in eligible cases.
- Timing pressure: These processes aren't passive. If your team misses the clean claim or response timeline, the practice's advantage lessens.
The hidden cost is administrative drag. If your staff can't identify which claims are NSA-protected, which are state-law governed, and which require a different appeal path, receivables age while everyone argues about classification.
Compliance rule: If your team cannot prove what the payer said about network status, you may lose a winnable reimbursement position before the financial dispute even starts.
Practical owner controls
A workable legal-risk framework looks like this:
- Centralize verification evidence: Save payer portal outputs, reference numbers, rep names, and date-stamped notes.
- Flag protected claims early: Don't let front-end staff treat NSA-related encounters like standard OON self-pay matters.
- Separate notice-and-consent cases: Non-ancillary services require stricter handling. Don't let generic intake forms carry legal weight they don't have.
- Escalate mixed state-federal cases quickly: If your market has state-specific surprise billing rules, generic national workflows won't be enough.
Building a Leak-Proof OON Billing Workflow
Most OON revenue problems start before the claim is filed. They begin at scheduling, insurance verification, intake, documentation, and handoff. If those steps are weak, your billing team spends its time repairing avoidable damage.
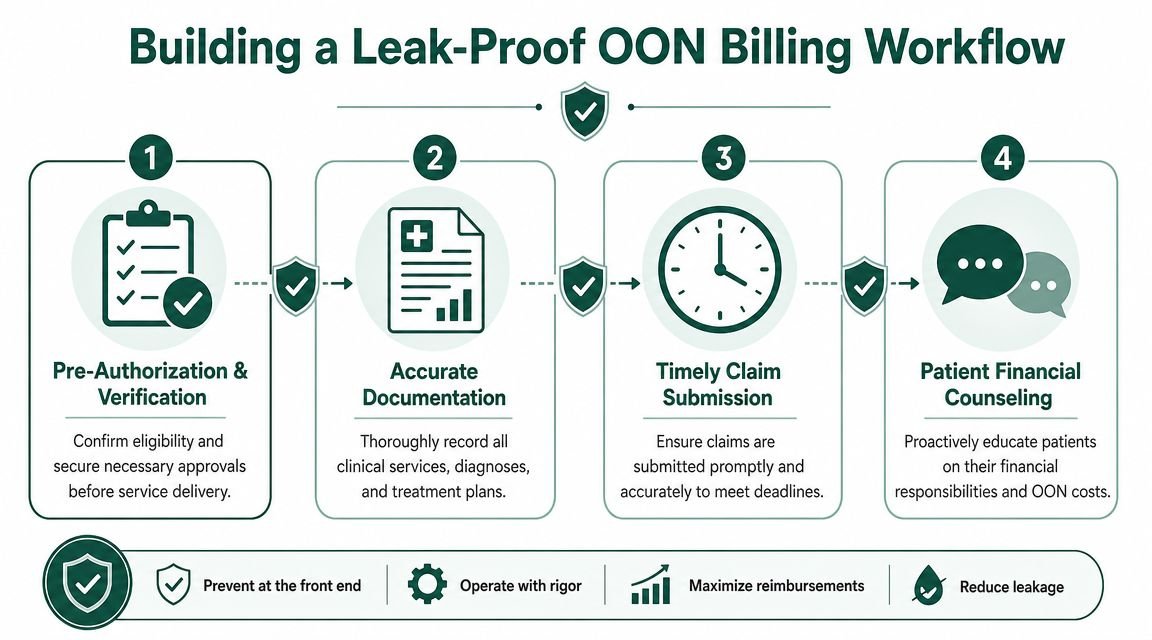
A strong workflow does not mean adding bureaucracy. It means deciding, before service, whether the claim is viable, what evidence will support it, and who owns each handoff.
Start with front-end verification that goes beyond eligibility
Eligibility alone is too shallow for out of network reimbursement. The team needs to verify whether OON benefits exist, whether preauthorization is required, how the payer determines reimbursement, and whether any referrals or special submissions are needed.
For high-value claims, that conversation should be documented with the same seriousness you would use for a prior authorization. Owners should require staff to capture the payer's stated OON methodology, call reference number, and any network-status representations made during the verification call.
This is especially important in hospital-based and procedure-heavy specialties. In anesthesiology billing, for example, one missed detail about rendering provider status, place of service, or modifier support can affect payment far downstream.
Documentation is the shortest path to faster cash
One industry source notes that incomplete or inaccurate OON submissions can delay review for as long as 90 days, and may require added evidence of medical necessity on appeal, according to PRG's guidance on handling out-of-network claims. That's why the superbill or claim package should be treated as a reimbursement instrument, not just a receipt.
For owners, that means requiring documentation that is complete enough to support first-pass adjudication:
- Diagnosis specificity: The diagnosis must match the service rendered and the payer's coverage logic.
- Procedure detail: CPT coding should reflect the actual work. If a modifier changes payment eligibility, it must be supported in the note.
- Rendering provider information: NPI, credentials, location, and service date accuracy are basic, but missing one of them can trigger avoidable review.
- Proof of medical necessity when relevant: Particularly important in behavioral health, pain management, imaging, and procedure-based care.
Weak OON documentation doesn't just create denials. It turns collectible money into labor-intensive money.
A simple operating model that works
The practices that protect OON revenue usually assign ownership in this sequence:
- Scheduling team confirms whether the patient may trigger an OON workflow.
- Verification staff determine plan rules, pre-service requirements, and payer methodology.
- Clinical team documents with downstream reimbursement in mind, not just compliance.
- Billing team submits a clean claim with all required data and supporting detail.
- Follow-up team reviews the EOB for allowed amount logic, not just payment receipt.
Owners who want to tighten these handoffs should review revenue cycle workflow improvements. Most OON write-offs are really workflow failures disguised as payer behavior.
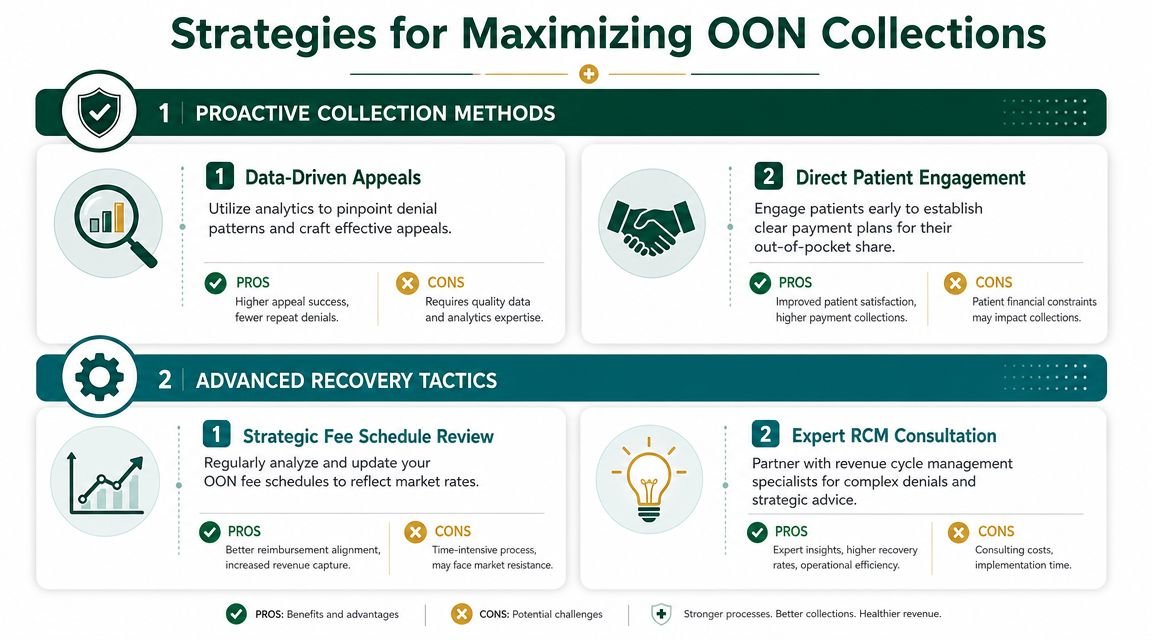
Strategies for Maximizing OON Collections
Once an OON claim is denied or underpaid, the practice needs a hierarchy of response. Not every claim deserves the same effort. Some need a correction. Some need a policy-based appeal. Some need negotiation. A few may justify more aggressive recovery steps, but that should be the end of the ladder, not the beginning.
Start with payment logic, not emotion
Historically, out-of-network physicians charged 637% of Medicare, while in-network rates averaged 266% of Medicare, according to the Yale surprise billing study. That pricing spread helps explain why payers scrutinize OON claims so aggressively. If your appeal only says the payment was unfair, it will usually go nowhere.
A better appeal asks a narrower question. Did the payer apply its own methodology correctly? Did it ignore documentation? Did it process the service under the wrong place of service, specialty designation, or reimbursement rule?
Build appeals in this order
Here is the collection ladder I recommend to owners:
- Correct obvious claim defects first: Fix missing modifiers, wrong rendering provider data, or unsupported units before you argue value.
- Challenge the adjudication basis: Ask for the payer's pricing rationale, policy citation, or benchmark basis when the allowed amount appears inconsistent.
- Use contract-style evidence when available: Prior authorizations, gap approvals, network-status misstatements, or written payer representations can matter more than generalized fairness arguments.
- Escalate selectively: Reserve labor-intensive appeals for claims with meaningful net recoverable value.
This is also where single-case agreements or gap exceptions can outperform retrospective appeals. If your physicians deliver hard-to-source specialty care, securing case-specific payment terms before treatment can remove a lot of downstream uncertainty.
Don't let staff “work the denial” without defining the reimbursement theory. Activity is not the same as recovery.
Treat patient balance strategies carefully
Balance billing is now much riskier in protected settings and can create legal exposure even where it may appear permissible. Owners should assume that aggressive patient-balance tactics will backfire if the team has not first confirmed whether surprise billing rules, notice-and-consent restrictions, or state law limitations apply.
If you do reach the collections phase on a legally collectible balance, the practice still needs a disciplined policy. For administrators managing older receivables or legal escalation questions, these Connecticut debt collection insights can help frame the difference between collectible debt and practically recoverable debt.
The bigger strategic move is usually upstream. Set realistic patient expectations early, collect what is clearly owed, and keep the payer dispute on the payer side whenever the law supports that approach.
For owners evaluating whether their current team is maximizing reimbursement or just posting what comes in, this overview of maximizing insurance reimbursements is a useful benchmark.
When to Partner with a Revenue Cycle Expert
Some OON problems can be fixed internally. Others become too technical, too slow, or too expensive for a small team to manage well. The decision point usually arrives when leadership realizes the practice is spending physician-grade time on payer behavior that should be handled by specialized revenue staff.
Red flags that usually justify outside help
We've seen practices write off significant recoverable OON revenue because no one internally had the time or expertise to pursue it correctly. The warning signs are usually obvious once you look for them:
- OON claims keep aging: Staff say they are “in follow-up,” but the same balances remain unresolved month after month.
- Appeals are generic: The team resubmits records without addressing the payer's pricing basis, legal classification, or policy error.
- Verification notes are weak: Nobody can prove what the payer represented before service.
- Specialty complexity is rising: Your practice is billing procedures, modifiers, units, or facility-based services that need tighter reimbursement control.
- Leadership lacks visibility: You can't quickly separate true denials, underpayments, NSA disputes, and patient-balance issues.
What a specialist does differently
A strong RCM partner doesn't just push claims faster. They build a tighter operational loop between front-end verification, claim construction, denial segmentation, and payer escalation. That matters in OON billing because underpayments often look superficially “final” unless someone knows what to challenge.
The best partners also know when not to fight. Some balances don't merit prolonged labor. Others require immediate escalation because delay weakens your position.
If your current team is struggling with those decisions, review what outsourced revenue cycle management should include. For OON reimbursement, the value is not clerical support. It is strategic recovery discipline.
Frequently Asked Questions From Practice Owners
Should we avoid out-of-network patients altogether
Usually, no. The better question is whether your practice can predict and manage the reimbursement path before care is delivered. Some OON encounters are commercially attractive when verification, documentation, and follow-up are strong. Others are operationally toxic because the plan rules are opaque or your team lacks the bandwidth to pursue them.
A blanket ban can push away clinically appropriate cases and referral opportunities. A selective acceptance policy is smarter. Approve OON encounters that fit your documentation strength, specialty's strengths, and collections process.
How should I think about state law versus federal surprise billing rules
Assume you need claim-level analysis, not broad assumptions. Some encounters fall squarely under federal protections. Others interact with state rules in ways that change reimbursement rights, notice requirements, or dispute options. If your staff treats every OON claim the same, they will miss collectible revenue on some claims and create compliance exposure on others.
This is why owners need cleaner internal categorization. Protected claim, standard OON commercial claim, state-regulated claim, and patient-pay balance should not live in one generic work queue.
My biller says they are appealing OON claims, but A/R keeps aging. What should I ask
Ask for specifics, not reassurance.
Request a report that shows:
- The denial or underpayment reason
- The payer's stated reimbursement methodology
- The exact appeal argument used
- What evidence was attached
- The current age and next deadline
If they can't provide that, the practice is probably doing activity-based follow-up rather than results-based follow-up. For a broader financial perspective on how these controls fit into overall practice operations, these RCM insights from Bookkeeping and Accounting of Florida Inc. are a useful companion read.
What's the first change a practice owner should make this quarter
Tighten pre-service verification for every encounter that may bill out of network. That means documenting network-status representations, benefit limitations, preauthorization requirements, and the payer's reimbursement methodology before the visit or procedure. If your team gets that step wrong, every downstream process becomes more expensive.
A close second is auditing EOBs for underpayment logic instead of just posting receipts. Many practices don't have a collections problem. They have an underpayment recognition problem.
If out of network reimbursement is driving denials, stale A/R, or unexplained write-offs, Happy Billing can help you identify exactly where revenue is leaking. A practical starting point is a free billing audit that shows whether the problem sits in verification, claim construction, payer follow-up, or appeal strategy.