How to Read an Explanation of Benefits for Practices
Most practices read an Explanation of Benefits too casually. That’s a mistake, because an EOB is not just a payment notice. It’s a financial audit trail that tells you whether the payer applied your contract correctly, whether the claim adjudicated as billed, and whether any balance can legally move to the patient.
If you want to know how to read an explanation of benefits as a practice manager or owner, the answer is simple: reconcile the claim line by line. Compare what you billed, what the payer allowed, what the payer paid, what they pushed to patient responsibility, and the remark codes explaining why. Anything less leaves money behind.
Your Guide to Reading an Explanation of Benefits
A practice can collect on schedule and still bleed revenue if the EOB is read like mail instead of a reconciliation tool.
For managers and owners, the job is not to confirm that a payer responded. The job is to confirm that the payer adjudicated the claim correctly, applied the contract correctly, and assigned only billable patient responsibility. If any one of those steps is wrong, cash posting becomes write-off posting.
Read the EOB against the original claim, your fee schedule, and the payer’s edit logic. That is how underpayments surface early, before timely filing, reconsideration, or secondary submission deadlines expire. In specialty practices, those misses add up fast. A cardiology line for CPT 93306 may be under-allowed. A same-day E/M with modifier 25 may be bundled without support. An anesthesia claim billed with QK may be priced as if medical direction requirements were not met.
Read the EOB as a revenue control point
Start with the adjudication risk, not the check amount.
Ask these questions first:
- Did the payer allow the line at the contracted rate for the billed CPT or HCPCS code?
- Did the payer process the code set and modifiers submitted such as 25, 59, LT, RT, AA, QK, or QX?
- Was cost share assigned correctly to deductible, copay, coinsurance, or a true non-covered amount?
- Do the adjustment and remark codes support the payer’s action under the policy and contract?
- Can the remaining balance legally move to the patient, or does the practice need to appeal, correct, or write it off under contract?
One fast test works well in audits. If the EOB cannot be tied back line by line to the claim and contract terms, it is not ready to post.
That standard matters because the financial errors are rarely obvious at the claim total level. A payer may apply multiple procedure reduction incorrectly, reprice one side of a bilateral service, deny an add-on code that should have paid with the primary procedure, or shift liability to the patient on a line that should stay with the payer. In orthopedics, that can mean LT or RT was ignored. In gastroenterology, it can mean modifier 59 was not recognized on a distinct procedural service. In anesthesia, it can mean the concurrency or supervision logic was applied incorrectly.
Practice leaders who want cleaner posting and fewer avoidable write-offs should document a single review standard across all specialties. For teams building that process, this guide to RCM for physician practices is a useful operating reference.
Deconstructing the EOBs Key Financial Fields
One bad read of the financial fields can turn a collectible underpayment into a permanent write-off. Practice managers who treat the EOB as a posting document instead of a reconciliation document lose revenue in small line-level amounts that add up fast.
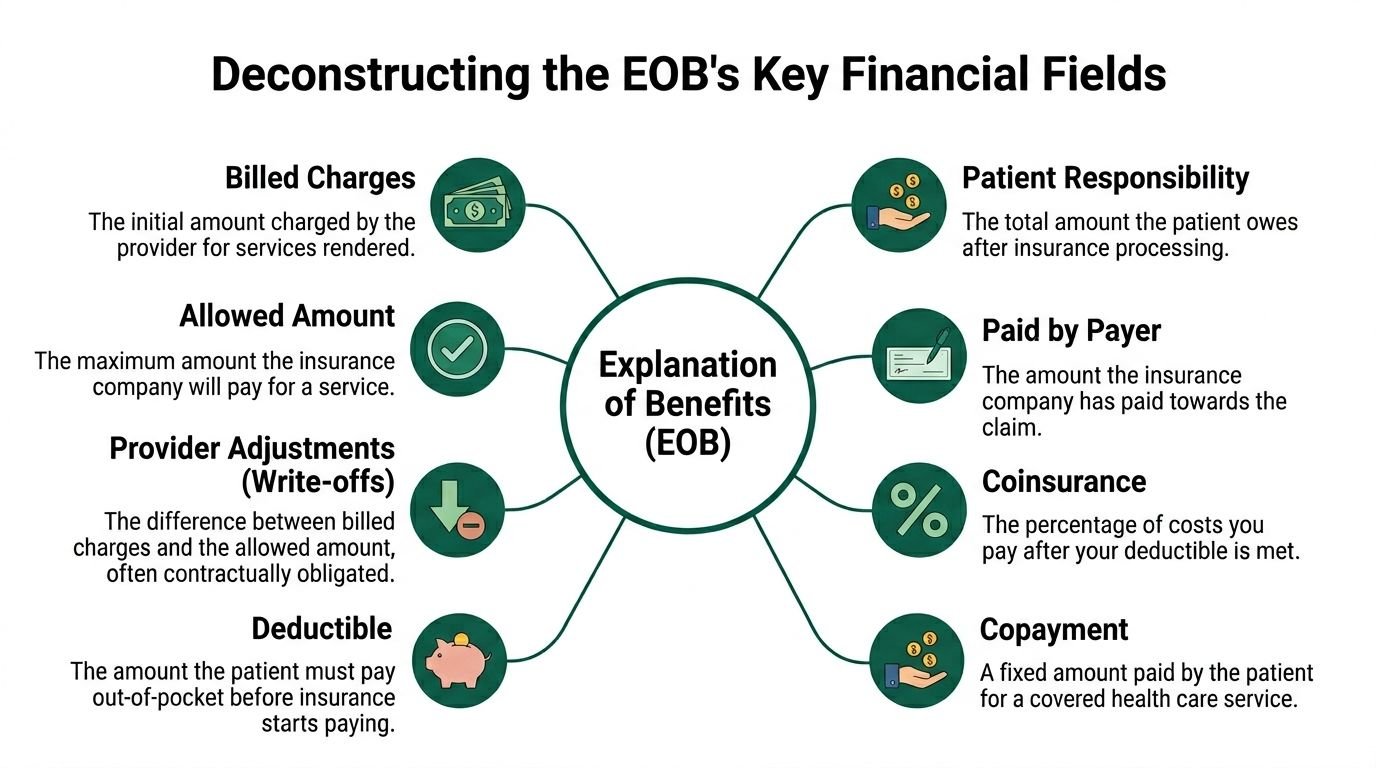
Provider charges and allowed charges
Start with the two numbers that set the rest of the math. The provider charge is what the practice billed. The allowed charge is what the payer says the line is worth under the fee schedule, policy rules, and network status.
For owners and managers, the allowed amount is the field that deserves the most skepticism. If the allowed amount is wrong, every number after it is wrong too. Payment posts short, the contractual adjustment looks larger than it should, and staff may bill the patient off an incorrect adjudication.
A cardiology example makes this clear. If your group billed CPT 93306 and the payer allowed it below the contracted rate, the issue may be a bad fee schedule load, the wrong locality, or processing under the wrong network product. None of those problems fixes itself at posting. They become write-offs unless someone stops the account and works the variance.
Specialty groups should review allowed amounts by CPT, modifier, and payer plan, not just by payer name. A pain practice may be paid one rate for 64483 and a different rate when laterality or multiple levels are involved. An ophthalmology group may see different contract logic on 92014 versus imaging lines billed the same day. A general billing checklist is not enough here. Teams need a line-review process tied to contract terms and payer edits. A practical starting point is this revenue cycle management checklist for medical practices.
Paid by insurer and contractual adjustments
The paid by insurer field answers one narrow question. It shows what the payer sent on that line after applying its pricing logic and the member’s cost share.
That number means very little by itself.
A line can show a payment and still be wrong. I see this often in anesthesia, where a payer pays something on the claim but miscalculates time units or applies the wrong modifier hierarchy for AA, QK, QX, or QZ. The line looks processed. The reimbursement is still short.
The contractual adjustment or discount field needs the same scrutiny. Some adjustments are valid contract write-offs. Others hide pricing errors, duplicate reductions, or bundling that should not have applied. In orthopedics, a payer may reduce a secondary procedure and also ignore a valid modifier that should have protected separate payment. In GI, an add-on code may be denied even though the primary procedure paid and the coding combination was correct.
Review the write-off as a contract question, not a bookkeeping step. The right test is simple. Does the payer’s adjustment match the contract and the code combination billed on that exact date of service?
Patient responsibility and non-covered amounts
The patient responsibility section is where compliance risk and collection risk meet. Deductible, copay, coinsurance, and non-covered amounts are different categories with different posting rules.
If staff collapse them into one patient-balance bucket, two things happen. The practice chases money it may not be allowed to collect, or it fails to bill money that is the patient’s responsibility. Both outcomes hurt the practice.
The highest-risk field is usually non-covered. Some non-covered amounts can transfer to the patient, but only if the payer decision and your documentation support that transfer. If the denial is really a bundling error, medical necessity issue that can be appealed, or an authorization problem caused by payer misprocessing, posting it straight to patient responsibility creates avoidable complaints and weakens your appeal position.
Specialty examples matter here. A dermatology practice billing lesion destruction and a separate biopsy may see one line marked non-covered because the payer ignored modifier 59. A neurology practice may see EMG or nerve conduction testing pushed to patient responsibility under a policy edit that does not fit the diagnosis mix submitted. In both cases, the wrong posting decision turns a payer issue into a patient collection problem.
Adjustment and remark codes
Adjustment codes and remark codes tell your team what action the payer expects next. They are not filler text.
At the line level, these codes separate a contractual write-off from a denial you should fight. They also help your posting team decide whether the balance can move to the patient, should stay with the payer, or needs a corrected claim. If the code narrative is vague, pull the payer policy and the ERA detail before posting.
A practical review standard looks like this:
| EOB field | What to verify | Why it matters |
|---|---|---|
| Billed charge | Matches the amount tied to the submitted CPT or HCPCS line | Confirms staff are reviewing the right service |
| Allowed charge | Matches your contracted rate for that payer, plan, code, and modifier set | Catches underpayments before they become write-offs |
| Payer payment | Matches expected reimbursement after cost share | Identifies short pays hidden inside partially paid claims |
| Contractual adjustment | Fits the contract terms and any reduction rules that actually apply | Prevents overstated write-offs |
| Patient responsibility | Assigned to deductible, copay, coinsurance, or valid non-covered status correctly | Protects collections and reduces patient disputes |
| Adjustment and remark codes | Support the payer’s action and point to the right follow-up path | Tells staff whether to post, appeal, correct, or hold |
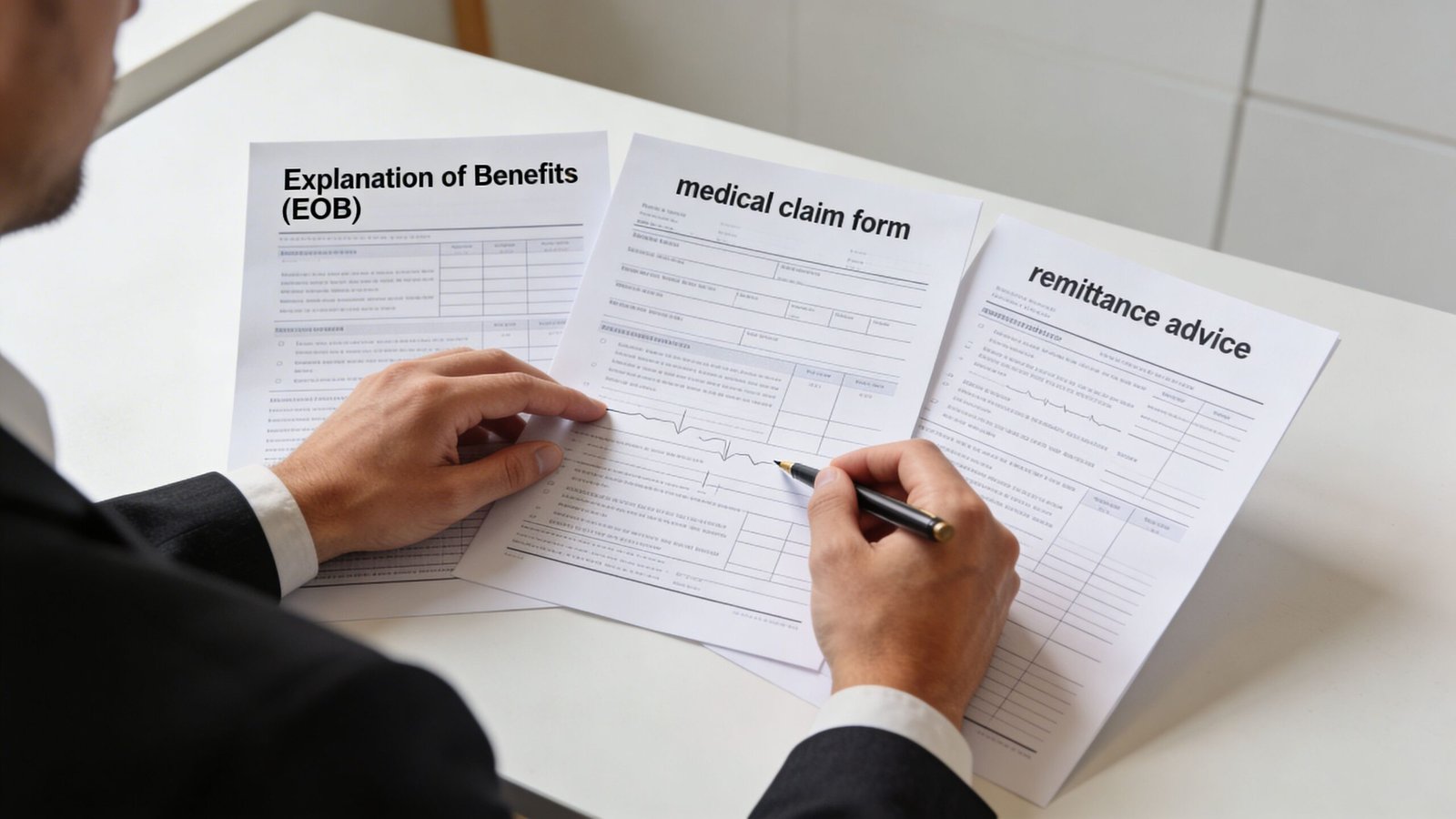
Reconciling the EOB with Your Claim and Remittance
An EOB by itself isn’t enough. You need a three-way match between the original claim, the ERA or 835 remittance, and the EOB image or payer portal record.
That’s how you catch line-level drift. A claim can leave your EHR correctly and come back adjudicated under a different code, with different units, or under a payer edit your team never expected.
Match the original claim first
Start with the claim that left your system. Pull the claim image or submission record and verify:
- CPT and HCPCS codes exactly as submitted
- Diagnosis pointers tied to each line
- Modifier usage such as 25, 59, LT, RT, TC, or 26
- Units
- Date of service
- Rendering provider and place of service
This step matters because staff often investigate the payer before confirming what was transmitted. If your scrubber dropped modifier 59 or the clearinghouse altered a line, the EOB may be correct and your resubmission path will be different.
Compare against the ERA line by line
The ERA is usually more operationally useful than the paper EOB because it drives posting logic. But the EOB still helps your team verify how the payer framed the claim adjudication.
A practical reconciliation sequence:
Confirm the line survived intact
If you billed CPT 93306 for a complete transthoracic echocardiography study, make sure the remittance reflects that same code and not a lower-value echocardiography code.Check units and modifiers
Specialty claims fail here often. A bilateral orthopedic line can lose LT/RT detail. An office E/M service billed with modifier 25 can be denied if the payer sees it as incidental to a procedure.Validate the adjudication category
Was the line paid, denied, bundled, reduced, or applied to deductible?Tie the remittance back to the EOB note language
If the ERA posts a reduction, the EOB remark language should explain it. If it doesn’t, treat that as a research item, not a silent adjustment.Post only after review
If the line is questionable, hold the adjustment category until someone verifies whether it’s contractual, appealable, or patient-billable.
A clean posting workflow doesn’t start with auto-posting. It starts with deciding which claims deserve exception review before the wrong adjustment hits the ledger.
For managers cleaning up posting controls, this revenue cycle management checklist is a good companion process document.
Use specialty examples, not generic posting rules
General rules break down in specialty environments.
In cardiology, a claim containing CPT 93306 alongside additional diagnostic services may trigger payer edits that reduce or reclassify one line. In orthopedics, CPT 29881 can collide with another arthroscopy code under bundling logic. In mental health, CPT 90837 may be denied on medical necessity or authorization grounds that look like patient responsibility until someone reads the remarks carefully.
A short reconciliation matrix keeps teams honest:
| Document | What it tells you | What can go wrong |
|---|---|---|
| Original claim | What your practice actually billed | Missing modifier, incorrect unit, wrong diagnosis pointer |
| ERA or 835 | What the payer posted electronically | Auto-posted reductions without validation |
| EOB or portal view | Why the payer says it processed the claim that way | Misread remarks, missed appeal opportunity |
If all three don’t line up, the account is not ready for final posting.
Decoding Denial Codes and Identifying Actionable Red Flags
Denial codes decide whether money comes back in the door or dies in A/R. If your team posts every unpaid line into a generic denial bucket, you lose the chance to recover underpayments, correct front-end errors, and stop the same payer mistake from repeating next week.
Read denial codes by next action, not by label. A line with patient responsibility, a line that needs a corrected claim, and a line that supports a contract dispute should never live in the same work queue.
Action first, code second
The EOB should tell your staff who owns the next step. Posting, coding, eligibility, authorization, and appeals each have different deadlines and different revenue outcomes.
Use a matrix your team can act on:
| Denial Code (CARC) | What it usually means | What your practice should do next |
|---|---|---|
| PR-1 | Deductible applied | Move to patient responsibility only after confirming active coverage, correct date of service, and correct patient plan |
| CO-45 | Charge exceeds fee schedule or contracted allowable | Post contractual adjustment. Review payer contract terms if the allowed amount looks off. Do not bill the patient |
| CO-97 | Payment included in another service | Check NCCI edits, CPT pairing, modifier use, and documentation support before writing off |
| CO-16 | Missing or invalid claim information | Identify the exact data failure, such as missing auth number, invalid NPI, or incomplete diagnosis pointer, then correct and resubmit or reopen |
| PR with non-covered language | Payer assigned liability to patient | Verify plan exclusion, ABN or financial waiver status where applicable, and whether the payer processed a covered service incorrectly |
One code can hide several different problems. CO-16 might mean a missing authorization on a pain management injection, an invalid taxonomy on a specialist claim, or a diagnosis mismatch that blocked adjudication. The recovery path changes based on the actual defect.
CO-45 and CO-97 are frequent leak points
Managers should audit CO-45 closely in specialties with high contract variance. Cardiology is a common example. If CPT 93306 is consistently allowed below the contracted rate, staff may post the adjustment automatically and never flag a payer underpayment pattern. That is not a denial management issue alone. It is a contract compliance issue.
CO-97 needs the opposite mindset. Teams often treat it as routine bundling and write it off. That is a mistake when the code pair could support a modifier and the chart supports separate work.
Orthopedics shows this well. If CPT 29881 denies as included with 29877, review the operative report before accepting the payer’s position. If the work occurred in separate compartments and the documentation supports a distinct procedure, modifier 59 or the payer-preferred X modifier may support reconsideration. If the modifier was omitted on the original claim, the revenue loss came from your coding workflow. If the modifier was present and the payer ignored it, the issue belongs in appeals or payer escalation.
Separate eligibility failures from coverage denials
Teams lose recoverable revenue when they call every unpaid line a denial.
An eligibility failure usually points to registration, COB, or insurance selection errors. A coverage denial points to medical necessity, authorization, frequency limits, bundling, or plan exclusions. Those categories need different owners, different correction steps, and different reporting.
Use this split:
Eligibility issue
Check effective dates, subscriber ID, payer selection, coordination of benefits, and whether the patient’s plan changed before the date of service.Coverage issue
Review payer policy, diagnosis support, prior authorization, frequency edits, and whether the billed service matches the documented indication.Bundling or modifier issue
Audit the CPT pair, review NCCI or payer-specific edits, and confirm the modifier was both justified in the chart and transmitted on the claim.
Mental health practices see this distinction often with 90837. One payer may deny for missing authorization. Another may process it as not medically necessary based on diagnosis or policy rules. A third may downcode behavior through policy edits that look like a denial problem but are really an underpayment problem. Those should not land in the same bucket.
For teams building tighter workflows, medical billing denial management processes should sit outside basic payment posting and include root-cause tracking by payer, CPT, and denial family.
Red flags that deserve immediate review
Some denial patterns justify same-day review because they signal a repeatable revenue leak:
Repeated CO-97 denials on the same CPT pair
Usually a modifier, documentation, or payer edit issue that will keep hitting future claims until someone fixes the rule.Multiple CO-16 denials from one location or one provider
Usually a front-end or claim-scrubbing defect, such as missing authorization data or invalid provider enrollment details.A single payer under-allowing one service family
Common in echocardiography, ASC procedures, psychotherapy, and anesthesia. This points to fee schedule variance, repricing error, or contract loading issues.“Not covered” language on routine in-network services
Verify whether the service is excluded or whether the payer misprocessed a covered benefit.Modifier-sensitive denials tied to 25, 59, 26, TC, LT, or RT
These lines need chart-level review because a bad modifier habit can depress revenue across an entire specialty.
Strong denial review is not about cleaning up yesterday’s unpaid claims. It is about finding the rule, edit, contract miss, or registration failure that will keep draining cash until someone fixes it.
Posting Patient Responsibility and Finalizing the Account
Posting patient responsibility is where practices either protect margin or create avoidable refunds, complaints, and bad debt.
An EOB balance is not a billable balance. Your team has to separate true patient liability from contractual write-offs, pending appeal amounts, and payer errors before anything hits patient A/R.
Know what can be billed and what cannot
Use the EOB in this order. Confirm the allowed amount. Confirm what the payer applied to deductible, coinsurance, and copay. Then confirm whether any remaining reduction is contractual or tied to a denial reason that still needs review.
The practical rule is straightforward:
- Deductible, copay, and coinsurance can move to patient responsibility if the claim processed correctly under the patient’s plan.
- Contractual adjustments stay off the patient statement.
- Denied amounts under appeal or corrected claim review should stay off the patient statement until the payer decision is final.
CO-45 is the common posting error here. If your charge for CPT 29881 is $1,850 and the payer allows $1,120 under contract, the $730 difference is a contractual adjustment. It does not belong in patient A/R. Posting that amount to the patient creates collection risk and compliance exposure, especially for in-network claims.
Specialties see this mistake in different ways. In behavioral health, a denied 90837 line may look patient-responsible at first glance. It may be a missing authorization, an incorrect POS, or a medical necessity denial that should be appealed. In cardiology, a reduced 93306 payment may reflect a multiple procedure logic issue, a modifier problem, or a contract loading error rather than valid patient liability.
A good posting team uses an exception rule before finalizing the account. If the payer paid materially below the expected allowed amount for that plan and code, stop the account from dropping to statements until someone checks the contract terms and adjudication logic.
Final posting controls that protect cash and compliance
Close the account only after these checks are done:
- Match patient liability to the EOB fields exactly, including deductible, coinsurance, and copay by line when applicable
- Post CO-45 and other contractual reductions to the correct adjustment bucket, not to patient A/R
- Hold CO-16, CO-50, CO-97, PR-204, and other reviewable denial lines until staff decide whether to appeal, correct, or transfer liability based on the payer rules and any signed waiver on file
- Verify secondary crossover status before billing the patient, especially for Medicare supplements and coordination-of-benefits cases
- Document the reason for every transfer to patient responsibility so staff can defend the balance on the phone and reverse it cleanly if the payer reprocesses
One bad posting decision can create three downstream costs. A patient complaint. A refund. A preventable aging balance.
Do not let your statement vendor decide patient liability by default. That decision belongs to billing staff who understand contract terms, denial categories, and specialty-specific coding rules.
Practices that want tighter controls usually improve posting accuracy and underpayment recovery at the same time. This guide on improving insurance reimbursement performance covers the upstream processes that support cleaner final posting.
If your practice works in behavioral health, cardiology, anesthesia, or orthopedics, build close-out rules around the codes and modifiers you bill every day. The teams with the fewest patient balance disputes are usually the ones that review final responsibility at the CPT, modifier, and payer-rule level instead of trusting the EOB summary line.
When to Escalate EOB Issues to Your RCM Partner
Escalate fast when an EOB problem repeats by payer, CPT, modifier, or place of service. A single bad line item costs dollars. A repeated adjudication pattern drains margin for months before anyone catches it.
An internal team can usually fix one underpaid 93306 claim. The threshold changes when the same payer keeps repricing 93306, 93000, or 78452 below contract, or when denials cluster around modifier logic your staff cannot resolve from the EOB alone. At that point, the issue is no longer posting accuracy. It is contract variance analysis, denial trend management, and appeal execution.
The handoff should happen as soon as your staff sees repeat behavior they cannot correct within the payer's timely filing or appeal window.
Escalate in situations like these:
- Recurring underpayments on the same code set or service family. Cardiology practices often see this on diagnostic testing. Orthopedics may see it on injection or fracture-care codes. Behavioral health may see it on recurring reductions to 90837 or telehealth claims with modifier 95.
- Modifier-driven denials that point to payer edit logic, not staff oversight. Examples include anesthesia claims with QK or QX, procedural claims denied after modifier 59 or XS, and bilateral or assistant surgeon issues tied to 50, 80, 81, or AS.
- Bundling patterns that need code-level review. If 20610 is repeatedly denied as incidental to an E/M or imaging service, someone needs to compare NCCI edits, documentation, modifier use, and the payer's reimbursement policy before the write-off posts.
- Medical necessity denials that affect a whole service line. A few CO-50 denials may reflect missing diagnosis linkage. A wave of them usually means your ordering, ABN, auth, or LCD policy controls are breaking upstream.
- Aging exception claims that your team keeps touching without resolution. If staff reopen the same account three times and still cannot decide whether to appeal, rebill, or write off, the account needs senior review.
A good RCM partner should quantify the leak. That means pulling a sample of paid claims, comparing allowed amounts to the contract or fee schedule, isolating denial rates by CARC/RARC and modifier, and telling you whether the root cause sits with registration, coding, prior auth, charge entry, or payer misadjudication.
That distinction matters financially. If the payer is underpaying a contracted rate, the fix is recovery and contract enforcement. If your coding team is missing modifier 25 on separate E/M work or billing 29881 with documentation that supports a different arthroscopy code set, the fix is operational. Owners need both answers before deciding where to spend labor.
Practices considering outside help should review what outsourced revenue cycle management services include before assigning a vendor only payment posting and expecting them to solve contract variance, denials, and appeals after the fact.
Frequently Asked Questions About EOBs
Is an EOB the same as an ERA or 835
No. The EOB explains adjudication in a payer-facing format, while the ERA or 835 is the electronic remittance file used for posting and workflow automation. You need both when investigating underpayments, denial logic, or adjustment classification.
Should my staff bill the patient as soon as the EOB shows a balance
Not automatically. First confirm the balance is true patient responsibility and not a contractual adjustment, payer processing error, or appealable denial. This is especially important on non-covered language, bundled denials, and specialty claims involving modifiers.
What’s the most common EOB reading mistake in private practices
The most expensive mistake is accepting the allowed amount and adjustment at face value without comparing them to the contract and original claim. That’s how underpayments, improper bundling, and bad patient balances slip through.
How quickly should an EOB be reviewed after receipt
The strongest process is immediate review, especially for exception claims. CMS notes that practices with sub-35-day A/R cycles commonly audit EOBs within 24-48 hours of receipt, which helps them correct issues before secondary claims or appeal deadlines are missed.
Happy Billing helps physician practices turn EOB review into a real revenue control process. If your team is dealing with underpayments, denial patterns, modifier-heavy specialty claims, or aging A/R, Happy Billing provides full-cycle RCM support built for practices that need tighter reconciliation, faster follow-up, and cleaner collections.