Medical Billing Costs: A Practice Owner’s 2026 Guide
A cardiology group once told me their billing was “only” a small percentage of collections, so they assumed costs were under control. What they were really paying for was slower cash, preventable denials, and staff time spent chasing claims instead of fixing the front end.
That's the short answer to the question of medical billing costs. Billing doesn't just cost what your vendor invoices. It costs what your practice loses when claims go out wrong, get paid late, get underpaid, or sit in A/R too long. If you own the practice, that difference shows up in revenue, denial pressure, and how much working capital you have available every month.
What Medical Billing Really Costs Your Practice
Most owners start with the visible fee. That's understandable, but it's incomplete.
The cost of billing is the combination of service fees, revenue leakage, and administrative drag. A lower fee can still be expensive if the billing team misses eligibility issues, lets denials age, or fails to pursue underpayments. A higher fee can be cheaper if it protects collections and keeps cash moving.

The fee is only the first layer
Most content about medical billing costs stays focused on price models. The bigger question is what billing costs after denials, underpayments, and A/R drag. The AAMC points to a deeper reimbursement problem, noting that Medicare covered less than 84% of average hospital costs in FY2020, which underscores that the financial problem is not just the fee for billing, but the gap between cost and reimbursement in the first place, as explained in this AAMC analysis of reimbursement and billing pressure.
That matters to independent practices because the billing department sits right at the point where revenue is either protected or lost. If your team submits office visits but doesn't catch modifier issues on procedures, or posts payments without checking payer logic, the practice absorbs the shortfall.
Practical rule: If you only track billing cost as a percentage fee, you're measuring the least important part of the problem.
What owners should actually watch
A useful billing review starts with three questions:
- How much cash are we giving up to preventable denials because insurance verification, authorization, or documentation breaks before the claim ever goes out?
- How long does money sit in A/R before someone works it, appeals it, or writes it off?
- Who is doing the rework when claims bounce for missing modifiers, invalid diagnosis pairing, or payer-specific edits?
In orthopedics, the difference between a clean claim and a delayed one often comes down to details like global periods and whether modifier 58 is supported for a staged procedure. In anesthesiology, mistakes around modifier reporting can hit reimbursement hard. In behavioral health, recurring authorization lapses can choke off cash flow even when documentation is otherwise sound.
If you want a clearer operating definition, think in terms of your full revenue cycle management process, not just claim submission. Billing cost belongs to the entire chain from scheduling through final payment.
How Medical Billing Companies Structure Their Fees
You'll usually see three models in the market. Each one can work. Each one can also hide problems if you judge it only by the headline price.
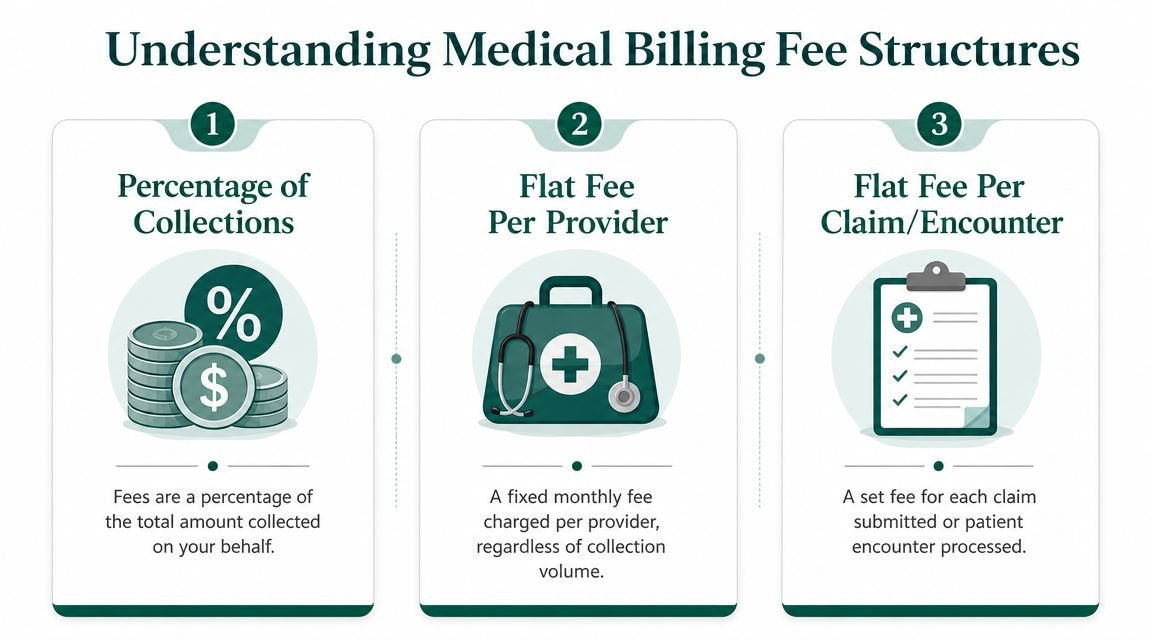
Percentage of collections
This is the most common structure. Outsourced billing services commonly charge 4% to 10% of collected revenue, with many market benchmarks clustering around the mid-range. One-time setup fees often add $500 to $1,500, and a practice collecting $1 million annually could spend about $40,000 to $100,000 per year in percentage-based fees alone, according to this 2025 medical billing pricing overview.
Think of this model like a sales commission. If collections rise, the vendor fee rises too. That can be fair if the company is actively improving payment outcomes, cleaning up denials, and protecting net revenue. It's less attractive if the vendor mostly pushes claims out and lets your staff handle the hard follow-up.
This model usually fits practices that want alignment around collections and don't want to build a larger fixed internal billing function.
Per-claim pricing
Per-claim pricing works more like transaction processing. The practice pays for each claim submitted or encounter processed. This can look efficient for high-volume, lower-complexity environments where claim workflow is relatively standardized.
The risk is that a cheap per-claim number may not include the expensive part of billing. If appeals, underpayment review, coding validation, and aging A/R work sit outside the base scope, your actual cost-to-collect can climb fast.
A primary care office with stable payer rules may tolerate that model better than a specialty group dealing with prior auth friction, procedural modifiers, and medical necessity edits.
Flat monthly fee
Flat-fee pricing behaves more like a subscription. It gives owners predictability, especially when volume is stable. But predictability only matters if the contract clearly defines what the practice is getting.
When I review flat-fee proposals, I look for what isn't written just as closely as what is. Does the fee include old A/R recovery, credentialing support, patient statements, claim edits, and denial appeals? Or does the practice sign a “fixed” agreement and discover a menu of extra charges after go-live?
A billing contract should tell you who owns denials, underpayments, and old balances. If it doesn't, the missing line items usually become your problem.
The model matters less than the scope
Owners often spend too much time comparing fee formats and not enough time comparing operational coverage. That's where decisions go wrong.
Use this quick frame when you compare proposals:
| Fee model | Best use case | Main risk |
|---|---|---|
| Percentage of collections | Practices that want incentives tied to cash actually collected | Fee rises with improved collections |
| Per-claim | High-volume, simpler workflows | Rework and appeals may be outside scope |
| Flat monthly fee | Stable practices that want budget predictability | Add-ons can erase predictability |
If you're weighing offers side by side, this medical billing outsourcing cost comparison is the right way to structure the analysis. Compare service scope first, then fee model, then contract terms.
Uncovering the Hidden Drivers of Your Billing Costs
Billing gets expensive when complexity meets inconsistency. That can happen inside the billing office, at the front desk, in provider documentation, or in the payer mix.
A 2026 industry analysis reported that claims adjudication costs providers $25.7 billion annually, and nearly 80% of medical bills contain at least one error, showing how mistakes and processing complexity drive rework across the revenue cycle, as summarized in these medical billing statistics on administrative burden.
Specialty complexity changes the cost-to-collect
Not all claims cost the same to bill.
Orthopedics is a good example. A straightforward office visit isn't managed the same way as a surgical claim tied to a global period, multiple procedure rules, or staged treatment where modifier 58 needs proper support. Pain management has similar friction when documentation, imaging support, and payer edits don't line up. Cardiology adds another layer with procedures, diagnostic testing, and medical necessity review.
Behavioral health looks simpler on paper, but recurring authorization management for codes like 90837 can create a steady stream of avoidable denials when no one owns the renewal workflow. Anesthesiology has its own exposure around unit capture, modifier logic, and concurrency reporting.
Front-end mistakes create back-end expense
The cheapest denial to fix is the one that never happens.
Practices often blame billing for problems that start much earlier:
- Eligibility failures because staff didn't verify active coverage before the visit
- Authorization gaps on recurring services or high-cost procedures
- Demographic errors that trigger basic payer rejections
- Incomplete documentation that leaves coders and billers guessing
- Payer-specific rule misses on modifiers, bundling, or medical necessity
Owners usually feel these failures as labor cost first. Staff spend time on calls, resubmissions, and appeals. Then the practice feels them as cash flow drag.
If you're trying to manage broader practice compliance and staffing exposure alongside RCM issues, tools outside billing can help frame the financial picture. For example, an ACA Penalty Estimator can be useful when benefit decisions and employer obligations are also affecting operating costs.
Hidden charges that show up after signing
A billing proposal can look clean and still become expensive in practice. Watch for charges tied to work that every serious RCM partner should define clearly before the contract is signed.
Common pressure points include:
- Legacy A/R cleanup that isn't included in onboarding
- Patient statement or payment posting fees billed separately
- Technology access charges for dashboards or reporting
- Coding review outside a narrow scope when documentation problems appear
- Appeals and denial work treated as extra labor instead of core service
The right response isn't just negotiating the percentage. It's tightening ownership. A disciplined denial management workflow lowers effective billing cost because it reduces rework, protects staff time, and gets money off the aging report faster.
The Break-Even Point for Outsourcing Your Billing
The outsourcing decision becomes clear when you stop asking, “What percentage do they charge?” and start asking, “What does my current process cost after salaries, software, supervision, and leakage?”
Industry benchmarks often place in-house billing at 7% to 10% of net collections when salaries, benefits, software, and overhead are fully loaded. Outsourced RCM is often priced between 4% and 9% of net collections, and it becomes cost-competitive when it controls denial rates and staffing inefficiencies better than the internal team, according to this breakdown of in-house versus outsourced billing economics.
Build the calculation the right way
For a practice owner, the break-even analysis should include five buckets:
Staff cost
Include billers, supervisors, and the management time the administrator or physician spends untangling billing issues.Technology cost
Practice management tools, clearinghouse access, reporting layers, and any outside coding support belong here.Instability cost
Staff turnover, training time, PTO gaps, and the slowdown that hits when one experienced biller leaves.Rework cost
Claims that need correction, appeals, rebilling, secondary follow-up, and patient-balance chasing.Cash flow cost
The operational strain created when money sits in A/R and the practice funds payroll and supplies while waiting for payment.
A practical example for a cardiology group
Take a $2 million cardiology practice. Cardiology billing isn't simple. Office visits may be straightforward, but diagnostic testing, procedures, modifier logic, and payer edits raise the stakes. If the current in-house team looks inexpensive on payroll but collections lag and old A/R keeps growing, the “savings” aren't real.
Here's a sample decision framework:
| Metric | In-House Team | Outsourced Partner (Happy Billing) | Financial Impact |
|---|---|---|---|
| Fully loaded billing cost as share of collections | Often sits in the in-house benchmark range | Often sits in the outsourced benchmark range | Compare actual cost-to-collect, not payroll alone |
| Denial follow-up ownership | Often fragmented across staff | Usually centralized under one service scope | Faster accountability reduces revenue leakage |
| Staffing continuity | Vulnerable to turnover and PTO | More stable service coverage | Less interruption to claim flow |
| A/R velocity | Can slow when follow-up is inconsistent | Improves when aging work is structured | Faster cash supports operations |
| Specialty workflow support | Depends on internal expertise | Depends on specialty competency | Better payer handling protects net collections |
The break-even point is reached when the outsourced partner does at least one of these things better than your internal team: reduces preventable denials, accelerates payment timing, tightens follow-up discipline, or removes staffing instability.
If outsourcing lowers your administrative burden but doesn't improve cash conversion, it may be convenient, but it isn't a strong financial move.
What usually tips the scale
In my experience, owners reach the right answer faster when they review operations, not just invoices.
Outsourcing tends to make financial sense when:
- Your best biller is carrying the department and there's no backup when that person is out.
- Physicians are answering billing questions weekly because documentation, coding, and payer edits aren't coordinated.
- Old A/R keeps aging even though new claims are going out.
- Specialty rules are getting more demanding than your current team can comfortably manage.
- Leadership can't get clean reporting on denials, underpayments, and payer behavior.
If you're comparing internal cost against external options, this in-house vs outsourced medical billing guide gives you the right lens. Measure control, depth, and recovery performance, not just headline pricing.
Actionable Strategies to Lower Billing Expenses Now
You don't need to change vendors tomorrow to reduce medical billing costs. Most practices can cut waste by tightening a few operational weak points first.
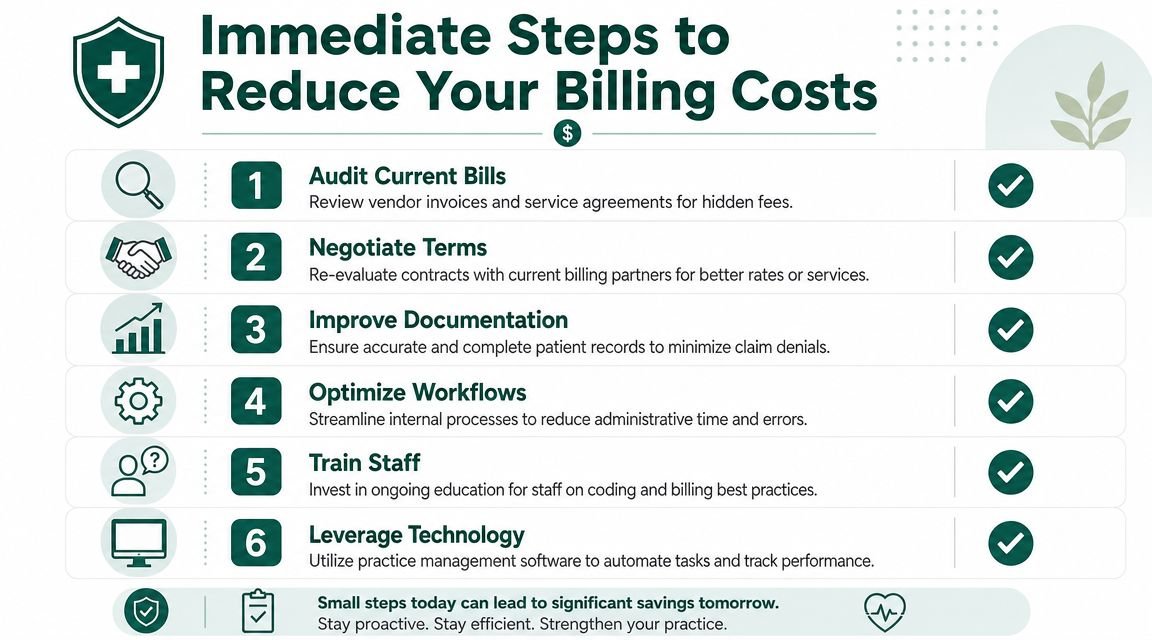
Focus on the denials that matter most
Don't review denials as one giant category. Split them by root cause and by financial importance. If one payer keeps rejecting claims for authorization defects while another keeps downcoding procedural work, those need different fixes.
Start with:
- Eligibility and registration denials
- Authorization denials
- Coding and modifier denials
- Timely filing misses
- Medical necessity edits
Then ask a simple owner-level question: which denial group is taking the most money off the table or tying up the most staff time?
Tighten front-desk controls
A weak front end raises billing expense later. The claim may still go out, but your team pays for the miss through rework.
Require a documented pre-visit process for:
- Insurance verification before the appointment date
- Authorization ownership for recurring and high-risk services
- Referral tracking when payer rules require it
- Demographic confirmation at every encounter
That work sounds basic because it is. It also has the highest impact in the revenue cycle.
Audit your payer payments, not just your claim submissions
Many practices check whether claims were paid, but not whether they were paid correctly. That leaves underpayments sitting unnoticed in posted balances.
For specialties with procedure-heavy billing, owners should sample high-value claims and ask whether the payer applied the expected contract logic, modifier handling, and bundling rules. In orthopedics and pain management, that often means reviewing post-op and procedural scenarios carefully. In behavioral health, it often means checking that authorized units and visit limits were applied correctly.
A broader guide to optimizing cash flow can also help leadership connect A/R discipline to day-to-day operating flexibility, especially when reimbursement timing is starting to affect payroll planning or vendor payments.
Strong billing teams don't just submit claims. They challenge avoidable write-offs and pursue payment variance.
Clean up contract scope and reporting expectations
If you outsource, get specific. Ask for reporting that shows denial categories, aging ownership, underpayment follow-up, and unresolved old A/R. If you bill in-house, require the same visibility internally.
Make your next review meeting answer these questions:
- Who owns appeals by payer?
- Who works old balances and how often?
- Which CPT codes are drawing repeated edits?
- Which modifiers create the most rework?
- Where does the handoff fail between front desk, clinical team, and billing?
That discipline is the backbone of good revenue cycle management best practices. It lowers cost by reducing waste, not by cutting corners.
Evaluating a Billing Partner for Your Specialty
A billing company can be competent in general medicine and still be the wrong fit for your specialty. Owners should test specialty depth early, because that's where hidden cost either gets prevented or multiplied.
The wrong partner usually doesn't fail on the basics. They fail on nuance. They submit the claim, but they don't understand where your specialty loses money.
Ask specialty-specific questions
Use pointed questions that expose whether the team understands your revenue risk.
For anesthesiology, ask how they audit time units, modifier use, and medical direction reporting. For behavioral health, ask how they manage recurring authorizations for 90837 and how they prevent treatment from continuing after authorization expiration. For orthopedics, ask how they handle global periods, post-op claim separation, and support for modifier 58 when a staged procedure is appropriate. For cardiology, ask how they review diagnostic and procedural claims for payer edits before submission.
If the answers stay generic, the cost will show up later in rework.
Scope matters as much as the fee
Published pricing ranges for per-claim models often fall around $3 to $12 per claim, and flat-fee arrangements commonly run from about $500 to more than $2,500 per month, but the economic result depends on what is included. If denial management, appeals, and coding validation are bundled, the fee may reduce hidden labor. If not, add-on charges can destroy predictability, as outlined in this medical billing pricing and scope overview.
That's why owners should ask for a service map, not just a rate sheet.
Use a checklist like this:
Claim edits and coding support
Do they catch payer-specific issues before submission, or only after rejection?Denial and appeal ownership
Are appeals included, or billed separately?Old A/R recovery
Who works balances that are already aging before transition?Provider communication
How do they resolve documentation questions without slowing down the physician?Reporting depth
Can they show payer trends, denial categories, and underpayment follow-up in a way leadership can use?
Match the partner to your clinical model
A multispecialty group shouldn't evaluate a billing partner the same way a single-specialty surgical practice does. Complexity sits in different places.
If your practice has specialty-driven friction, review providers with demonstrated fit for your field, not just a polished sales process. The specialty billing pages here are a good benchmark for what specialty-specific RCM questions should look like in anesthesiology, cardiology, orthopedics, behavioral health, and other high-variation practices.
Answering Your Top Questions on Billing Costs
Is a lower billing percentage always better
No. A lower fee can be more expensive if denials rise, underpayments go unworked, or A/R slows down. Owners should judge billing cost by net cash performance and operational burden, not by percentage alone.
When should I outsource instead of keeping billing in-house
Outsourcing becomes attractive when staffing instability, specialty complexity, or weak follow-up is costing the practice more than the perceived control of keeping billing internal. If physicians or administrators are spending too much time fixing revenue cycle problems, the in-house model is already costing more than it appears.
Which specialties usually need the most scrutiny
Procedure-heavy and authorization-heavy specialties need the closest review. Orthopedics, anesthesiology, cardiology, pain management, and behavioral health all have billing risk that isn't visible from claim volume alone. Modifier handling, global periods, unit logic, and payer-specific authorization workflows can change financial outcomes quickly.
What should I ask a billing company before signing
Ask who owns denials, appeals, underpayments, and old A/R. Ask how they report performance by payer and CPT category. Ask how they handle specialty-specific claim scenarios that affect your practice's biggest revenue lines. If they can't answer concretely, don't expect strong execution later.
If you want an expert second look at what billing is really costing your practice, Happy Billing can help you pressure-test the numbers. A good next step is to request a complimentary billing audit so you can see where fees, denials, and A/R drag are affecting collections.