Medical Bill Review Services: A Practice Owner’s Guide
If you're asking whether medical bill review services are worth it, the answer is yes. About 80% of medical bills in the United States contain at least one error, according to ClinicMind's medical billing statistics summary. For an independent practice owner, that isn't an abstract compliance issue. It's a direct threat to revenue, denial rate, and days in A/R.
We see this constantly in specialty practices. A missed modifier, unsupported unit count, weak documentation match, or payer rule mismatch doesn't just create a bad claim. It slows cash, increases rework, and forces your staff to spend time appealing preventable denials instead of collecting clean revenue. If you want a practical baseline on the broader revenue cycle context, review this guide on what revenue cycle management actually covers.
What Are Medical Bill Review Services?
Medical bill review services are a structured audit process that checks claims, charges, documentation, payer rules, and payment logic before money is lost. In plain terms, they exist to catch billing defects before those defects turn into denials, underpayments, refund demands, or patient disputes.
A lot of owners confuse bill review with denial management. That's a mistake. Denial management is reactive. Medical bill review is preventive. One tries to recover money after the claim breaks. The other stops the break from happening in the first place.
What the service actually reviews
A serious bill review function looks at more than whether a CPT code exists on the claim. It checks whether the claim is internally consistent and financially defensible.
That usually includes:
- Charge accuracy: Are the CPT and HCPCS lines supported by the encounter, op note, anesthesia record, cath lab report, or therapy note?
- Modifier logic: Is modifier use defensible under payer policy, or are you creating an avoidable edit?
- Documentation alignment: Does the record support the level billed, the units billed, and the medical necessity implied by the code set?
- Pricing integrity: Are contract terms, fee schedules, and allowed amounts being applied correctly?
- Duplicate and conflicting charges: Are you billing the same work twice, or splitting services in a way the payer will bundle back down?
Why practice owners should care
When physicians hear “bill review,” they often think of an administrative layer added on top of billing. I think of it differently. It's a margin protection system.
If your group is seeing rising denials, aging A/R, or unexplained write-offs, bill review is often where the leak becomes visible. The fix usually isn't hiring one more biller to work denials faster. The fix is to stop feeding bad claims into the system.
Practical rule: If your team is touching the same claim twice, your process is already too expensive.
For practices comparing internal controls with outside tools, it's also worth seeing how newer platforms are approaching intake and review. One useful example is Matil's solution for medical bills, which shows how medical bill analysis is becoming more structured and repeatable.
The Medical Bill Review Workflow Explained
A good review workflow works like a multi-point inspection. You don't want one person glancing at the claim and hoping the clearinghouse catches the rest. You want layered controls that stop errors at different points before submission and before payment posting.
The three-part defense
The strongest medical bill review services combine data integrity checks, automated repricing logic, and expert clinical or coding review, which Rising Medical Solutions describes as the most effective design for catching inappropriate charges, duplicate billing, and documentation mismatches before payment decisions are made.
That matters because no single control catches everything.
Data integrity checks catch basic but costly defects. Wrong patient demographics. Missing authorization numbers. Invalid provider identifiers. Date mismatches. Incomplete rendering or billing provider setup. These are boring errors, but they kill claims every day.
Automated repricing and rule logic checks whether the charge structure fits payer rules, contract terms, and edit logic. During this process, bundling conflicts, duplicate line items, incompatible modifiers, and frequency issues surface before the payer does it for you.
Expert review handles what software won't interpret correctly on its own. Medical necessity questions. Specialty-specific unit logic. Complex modifier combinations. Operative and procedural documentation that technically supports one code set but financially performs better under another valid structure.
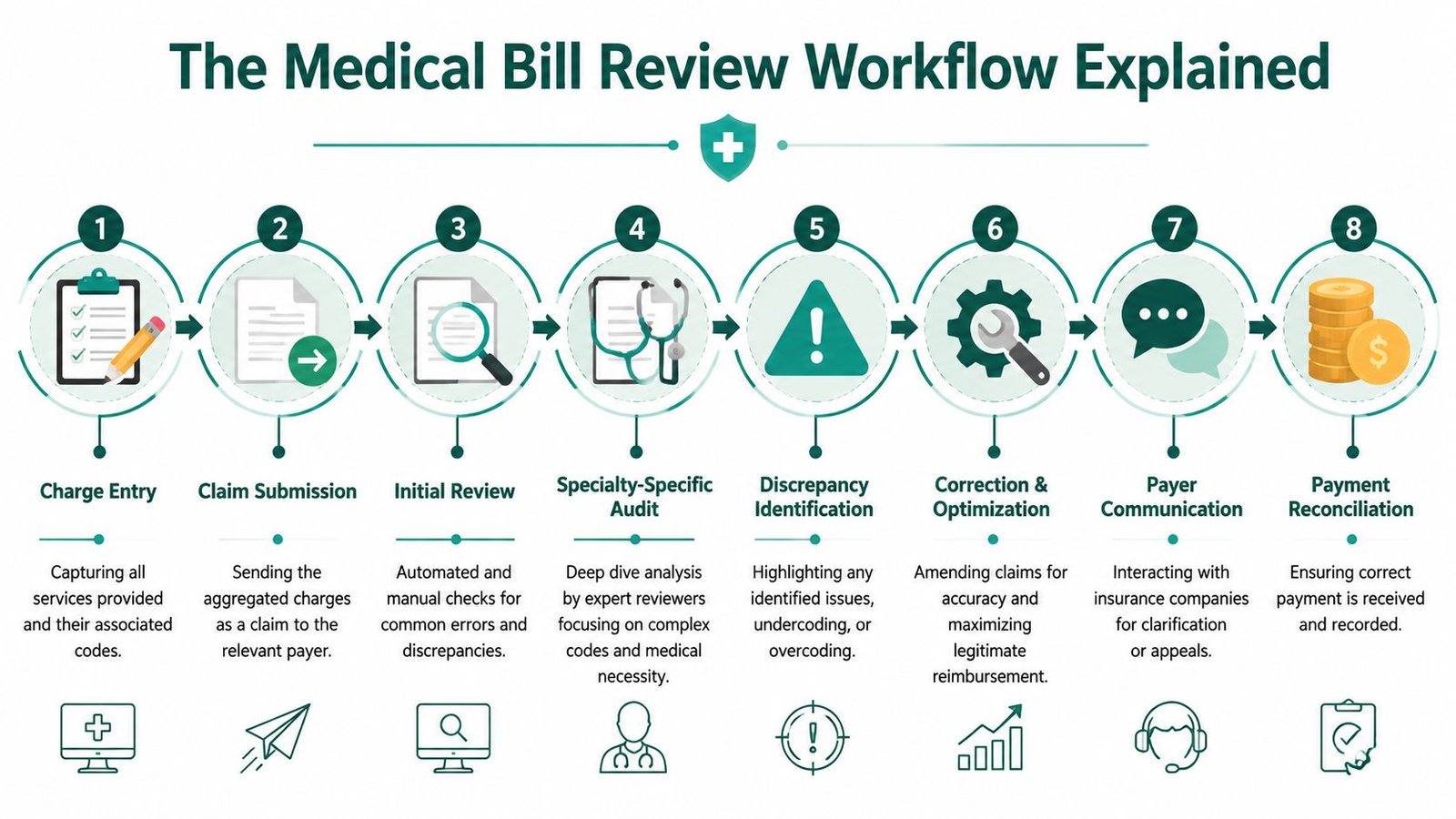
The workflow in practice
Here's what a real process should look like inside a practice or outsourced RCM operation:
- Charge capture enters the system: The service starts with what the provider documented, not with what someone guessed should be billed.
- Front-end edits run immediately: Eligibility, demographics, provider setup, place of service, and authorization details are validated.
- Code and modifier review follows: CPT, ICD-10-CM, HCPCS, and modifier combinations are checked against the chart and payer edits.
- Specialty review kicks in on high-risk claims: Anesthesiology time units, cardiology procedure combinations, or behavioral health documentation risk get a second look.
- Claim is corrected before submission: That reduces first-pass failure and cuts rework.
- Payer responses are reconciled: ERA, EOB, and posted payments are matched back to expected reimbursement logic.
- Variance review closes the loop: Underpayments, silent bundling, and payer processing errors are flagged instead of written off.
A superficial scrubber checks syntax. A real review process checks whether the claim will survive contact with the payer and get paid correctly.
If you want a clearer view of what belongs to billers versus auditors versus a full RCM partner, this explanation of what medical billers do day to day is useful context.
Key Benefits and Performance Metrics
Medical bill review shouldn't be judged by whether it “helps the billing team.” It should be judged by whether it improves the financial numbers you review every month. If it doesn't reduce preventable denials, tighten payment velocity, and protect collections, it's overhead.
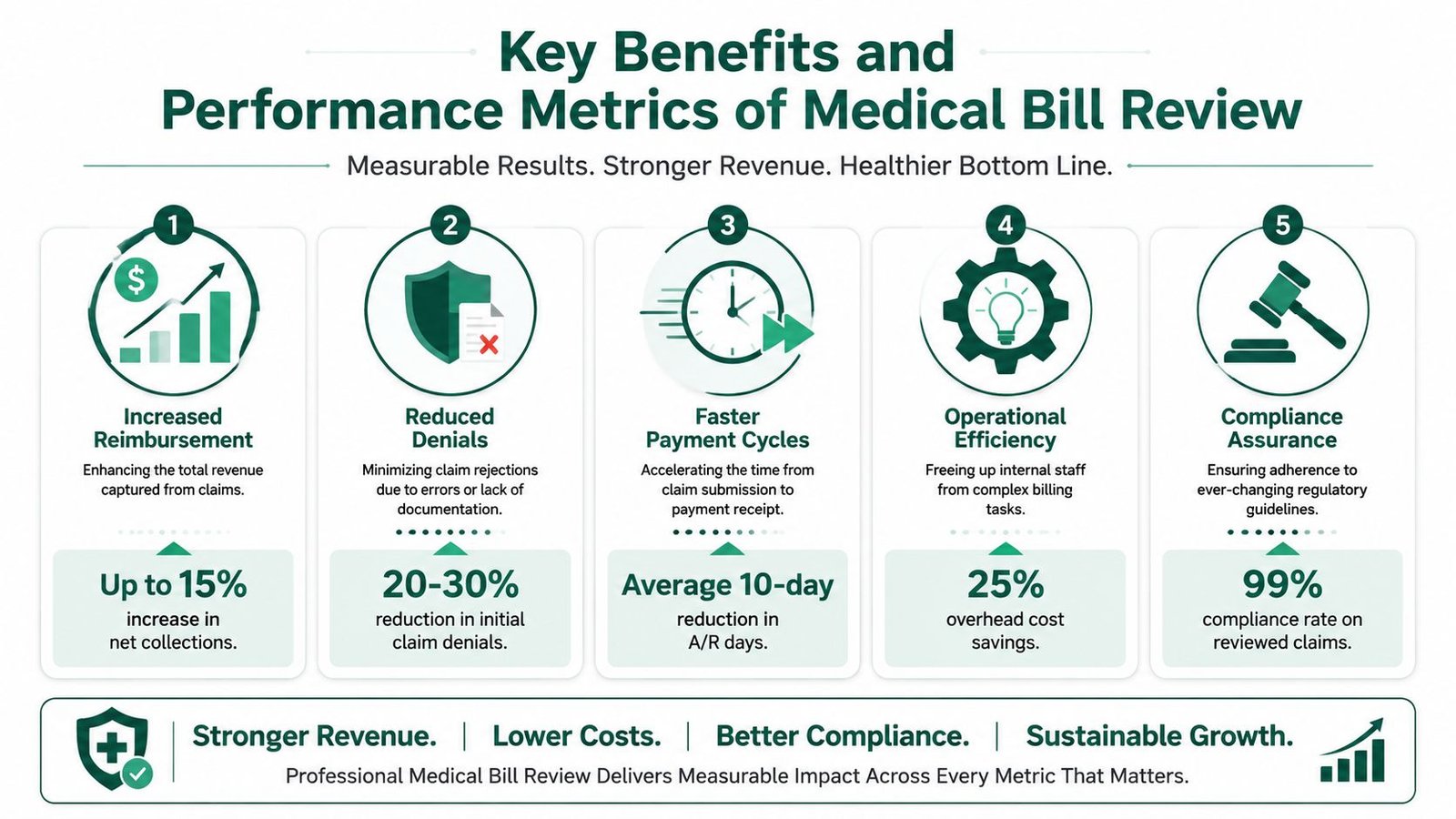
The metrics that actually matter
I focus on four outcomes.
| Metric | What bill review changes | Why owners should care |
|---|---|---|
| First-pass claim quality | Fewer preventable defects leave your system | Staff spend less time reworking claims |
| Denial rate | Front-end errors get caught before payer rejection | Denials stop draining cash and labor |
| Days in A/R | Clean claims move faster than corrected claims | Cash arrives with less lag |
| Net collections | Underbilling, missed modifiers, and unsupported charges get addressed | You keep more of the revenue already earned |
The article brief mentions common target thresholds owners watch, and those are useful operating benchmarks. But the right way to use bill review is not to chase vanity percentages. It's to identify where your practice leaks money and remove the root cause.
Where the financial lift comes from
Most gains come from ordinary failures that nobody owns until cash drops.
- Missed revenue capture: Charges that should have been billed differently, or not written off after weak first submission.
- Preventable denials: Bad modifier pairing, incorrect place of service, poor diagnosis support, late filing exposure, or mismatched provider enrollment.
- Payment variance: The payer paid something. Your team posted it. Nobody checked whether the allowed amount was correct.
- Labor waste: Skilled staff spend time fixing claims that should have gone out clean the first time.
For administrators trying to build cleaner internal workflows, some principles from automated invoice processing also apply here. Standardized intake, exception handling, and reconciliation discipline matter just as much in healthcare revenue as they do in AP operations.
Owner takeaway: The real ROI isn't just more collected dollars. It's fewer touches per claim, fewer aging balances, and fewer avoidable write-offs.
If you're measuring billing performance at the practice level, keep a close eye on the medical billing KPIs worth tracking every month. A bill review program without KPI accountability becomes a reporting exercise instead of a revenue strategy.
Why Specialty-Specific Review Is Non-Negotiable
Generic bill review is fine for generic risk. High-stakes specialties don't have generic risk.
In anesthesiology, cardiology, orthopedics, pain management, and behavioral health, a reviewer has to understand more than line-item coding. They need to understand how the specialty produces documentation, how payers interpret it, and where financial exposure hides.
Zurich notes that the deeper value of bill review in complex settings is clinical review, provider credential validation, and contract alignment. It also reports average savings of 63% off annual billed charges in workers' compensation settings when these deeper checks are applied in complex claims, which you can read on Zurich's medical bill review overview. That figure comes from a payer environment, not a physician practice benchmark, but the lesson is still clear. Complexity creates leakage, and shallow review misses it.
Anesthesiology and unit-based revenue risk
Anesthesia billing fails when the reviewer doesn't understand time units, base units, concurrency, and direction modifiers. If modifier QK, QX, QY, or AA is applied incorrectly, your reimbursement logic changes. If start and stop times don't reconcile to the anesthesia record, you create either underbilling or audit risk.
A generic reviewer may see a paid claim and move on. A specialty reviewer asks whether the claim was billed under the correct medical direction structure, whether the provider credential was aligned to payer enrollment, and whether the units billed match the actual record.
Cardiology and bundling exposure
Cardiology groups deal with expensive procedures, imaging, and payer scrutiny. Claims involving CPT 93458 or related cath and imaging combinations can trigger bundling edits fast if the documentation and code pairing aren't airtight. Modifier misuse and diagnosis support problems can turn a technically performed service into a delayed or reduced payment.
That's why a cardiology practice shouldn't settle for a generalist vendor. The vendor has to understand interventional coding logic, supervision requirements, documentation thresholds, and payer-specific edits. If you want a deeper look at the operational side, review this guide on cardiology revenue cycle management.
Behavioral health and note-to-code mismatch
Mental health practices often lose money through documentation mismatch rather than dramatic coding errors. The service length, therapy modality, add-on logic, and E/M support all have to line up. If the note says one thing and the billed structure implies another, denials follow.
Specialty review isn't optional when the specialty itself determines how revenue is calculated.
For a broader view of billing models across anesthesiology, cardiology, and more, compare vendors by specialty depth, not by who promises the lowest fee.
Evaluating a Medical Bill Review Vendor
A weak vendor choice shows up fast in cash flow. In high-acuity specialties, one vendor that misses anesthesia time discrepancies, cath lab bundling edits, or implant underpayments can push more claims into rework, increase aged A/R, and leave six figures sitting with payers instead of in your bank account.
Evaluate vendors by financial control, not sales polish. I want to know how they reduce denial volume, how they recover underpayments, how they handle specialty-specific coding risk, and how they report performance in a way an owner can use.
Vendor evaluation checklist
| Criteria | What to Ask | Why It Matters |
|---|---|---|
| Specialty expertise | Which specialties do you actively review, and which claim types trigger senior review? | An anesthesiology or cardiology group needs auditors who understand time units, modifier logic, NCCI edits, device-intensive procedures, and payer-specific reimbursement rules |
| EHR workflow | Can you work inside our current EHR and PM system without forcing a platform change? | A forced system change creates charge lag, retraining, and posting errors. That raises A/R days before the contract has even settled in |
| Review depth | Do you stop at claim scrubbing, or do you compare the chart, payer policy, contract terms, and posted payment? | Scrubbers catch format issues. They do not catch underpaid high-dollar claims or documentation gaps tied to denials |
| Reporting | Can you show denial categories, first-pass resolution rate, underpayment trends, and A/R aging by payer and provider? | Owners need operating data tied to cash. Activity logs do not tell you where revenue is leaking |
| Escalation model | Who reviews high-risk claims? Certified coders, specialty auditors, or general billing staff? | Complex claims need judgment from people who know the specialty, not a generic queue team |
| Compliance controls | How do you handle HIPAA, audit trails, access logs, role-based access, and breach response? | Bill review touches PHI, payment data, and documentation. Review their controls against practical benchmarks like CloudOrbis HIPAA guidance |
| Pricing model | Is the fee based on collections, claim volume, a fixed scope, or a hybrid? | A bad fee model rewards claim volume and follow-up volume instead of cleaner claims and faster cash |
| Payer management | Who owns underpayments, appeal support, documentation requests, and edit resolution? | Split ownership creates delays, duplicated work, and write-offs that no one claims responsibility for |
Ask for proof. A real vendor should be able to show specialty-level examples, redacted if needed, of claims they corrected before submission and underpayments they identified after posting.
Red flags I'd treat seriously
- They lead with migration. A vendor who wants you on their platform before they understand your denial patterns is optimizing their workflow, not your revenue.
- They speak in generic billing language. If they cannot explain anesthesia concurrency risk, cardiology bundling exposure, or specialty-specific modifier use, they will miss the claims that matter most.
- They report tasks instead of outcomes. You need trends in denials, net collection rate, payment variance, and aged A/R by payer. Ticket counts and touch counts do not improve cash.
- They separate review from correction. If one team finds the issue and another unrelated team is supposed to fix it, errors sit in limbo and A/R keeps aging.
- They avoid contract variance discussions. If they never compare expected reimbursement to actual payment, underpayments stay hidden.
One direct question exposes weak vendors fast. Ask which payer edits they catch before claim submission for your specialty, and ask what percentage of those edits are resolved before the claim leaves the door. Vague answers usually mean the front-end review process is thin.
For owner-level due diligence, use this checklist of questions to ask a medical billing company before hiring.
Common Pitfalls and How to Avoid Them
The biggest mistake practice owners make is assuming outsourcing automatically fixes billing. It doesn't. Outsourcing a weak process just gives the weak process a new address.
Pitfall one, buying on price
Cheap billing is expensive when claims go out wrong. A low-fee vendor that lacks specialty depth can lead to increased rework, write-offs, and payer friction. You won't feel it on the contract. You'll feel it in slower collections and more A/R over aging thresholds.
Avoid this by tying vendor evaluation to outcomes. Ask how they prevent denials before submission, how they review underpayments after posting, and who audits high-risk claims.
Pitfall two, ignoring system fit
If the vendor can't work cleanly inside your EHR and practice management setup, your staff becomes the integration layer. That's where charges get delayed, documentation gets lost, and accountability gets fuzzy.
This is also where security gets overlooked. Before you hand over PHI, compare their controls against practical standards like this CloudOrbis HIPAA guidance. You don't need marketing language. You need clear answers on access control, audit logs, encryption, and breach response discipline.
Pitfall three, treating bill review as only a coding function
Owners often think bill review starts and ends with CPT and modifier accuracy. That's incomplete. The hard cases involve payer policy, payment variance, contract terms, and compliance exposure.
The No Surprises Act changed the operating environment for out-of-network billing disputes. Pennsylvania's consumer guidance explains that the law blocks many surprise out-of-network bills and adds review pathways, but it doesn't apply universally to Medicare, Medicaid, VA, or TRICARE, and plan-specific rules still matter, as outlined in Pennsylvania's No Surprises Act review guidance. For a practice owner, the implication is straightforward. If your review service still acts like every issue is just a repricing problem, it is behind.
Pitfall four, fixing symptoms instead of root causes
If the same denial reason keeps showing up, the issue isn't your appeals team. It's your process upstream. That could mean scheduling errors, authorization failures, weak charge capture, poor note structure, or incomplete provider enrollment.
Use denial categories to trace the leak back to source:
- Authorization failures: Usually a front-desk or referral workflow defect
- Modifier denials: Often a coding logic or specialty knowledge gap
- Medical necessity denials: Usually documentation and diagnosis support
- Underpayments: Often contract loading, posting, or variance review weakness
The best medical bill review services don't just catch errors. They tell you why your organization keeps producing them.
Frequently Asked Questions for Practice Owners
How do I know if my practice needs medical bill review services or a full billing replacement
Start with the leak size and where it starts.
If your anesthesiology group keeps losing revenue to modifier errors, missed concurrency details, or payer underpayments on clean claims, bill review is usually the right fix. If your cardiology practice has broken scheduling, weak eligibility checks, incomplete charge capture, stale credentialing, and no usable reporting, you need broader RCM support. Bill review fixes claim-level failure points. It does not rebuild a damaged revenue cycle.
A simple rule works. If the same denial codes, payment variances, or aging buckets keep recurring, add review. If revenue is breaking across intake, coding, posting, follow-up, and reporting, replace the process, not just the checkpoint.
Will outsourcing bill review make us lose control of the billing process
You keep control when the vendor gives you operating visibility.
Require monthly reporting on denial rate by payer, first-pass resolution, underpayment recovery, aging by bucket, and root-cause trends by specialty. For high-risk specialties, that reporting should also show where revenue is slipping on procedure-heavy claims, modifier usage, medical necessity edits, and documentation gaps. If a vendor cannot show you what hit A/R over 30, 60, and 90 days, they are not managing performance. They are asking for trust without proof.
Which specialties benefit most from medical bill review services
High-stakes specialties get the biggest financial return because the claims are harder to code correctly and more expensive to get wrong.
Anesthesiology, cardiology, orthopedics, pain management, emergency medicine, and behavioral health all sit in that category. In anesthesiology, one time-unit discrepancy or concurrency issue can cut reimbursement fast. In cardiology, missed modifiers, device-related coding errors, or documentation gaps around medical necessity can turn a high-value procedure into a denial or underpayment. Review matters more when each claim carries more revenue and more payer scrutiny.
Should my practice expect bill review to reduce denials immediately
You should expect early gains on obvious defects. Eligibility misses, missing modifiers, claim edit failures, and basic documentation gaps can improve within the first reporting cycle.
The bigger payoff takes longer. Specialty-specific denial patterns, payer behavior, and physician documentation habits do not change in a week. Judge results by cleaner claims, lower preventable denials, fewer underpayments, and shorter A/R over the next few months.
If your practice is carrying avoidable denials, underpayments, or aging that keeps drifting past target, Happy Billing is worth a hard look. Their model fits specialty groups that cannot afford coding sloppiness or slow payer follow-up. If you want a clear view of where cash is leaking before you make a larger RCM decision, request a free billing audit.