Dental Medical Billing Services: A Practice Owner’s Guide
If you perform medically necessary treatment in a dental setting and still bill everything through dental insurance, you're probably suppressing revenue and lengthening A/R without realizing it. The reason is simple: dental plans and medical plans were built for different purposes, and a practice that doesn't bridge that gap correctly ends up writing off collectible dollars, inviting denials, or both.
The risk isn't theoretical. A 2026 industry report says 80% of medical bills contain at least one error, and 58% of collection accounts stem from healthcare bills according to ClinicMind's medical billing statistics roundup. For a practice owner, that means dental medical billing services aren't an administrative convenience. They're a revenue control function.
What Are Dental Medical Billing Services
Dental medical billing services are a specialized revenue cycle function that determines when a procedure performed in a dental office should go through medical insurance instead of dental insurance, then handles the documentation, coding, claim submission, and follow-up required to get paid.
Medically necessary dental-adjacent care doesn't behave like routine hygiene, fillings, or crown work. Sleep apnea appliances, trauma-related procedures, TMJ-related care, and other functional treatments often live in a reimbursement gray zone. If your team treats them like standard dental claims, you create avoidable write-offs. If your team bills them to medical without the right process, you create denials.
Why owners should care
Practice owners usually spot the problem only after it hits the financials:
- A/R stretches out because the team submits the wrong claim type first
- Denials rise because medical necessity isn't established clearly
- Front-desk estimates miss the mark because benefits were checked in the wrong system
- Providers lose confidence in offering certain services because reimbursement feels unpredictable
That's why this work belongs in the same conversation as collections and claim velocity. If you're tightening the back end, this broader guide to AR management for service firms is useful context because it frames receivables as a systems issue, not a bookkeeping issue.
Practical rule: If a procedure solves a disease, injury, airway issue, pain condition, or functional impairment, you should at least test whether it belongs in the medical billing workflow before defaulting to dental.
What the service actually does
A competent dental medical billing service doesn't just "send claims." It usually handles work such as:
- Eligibility review for medical benefits tied to the planned treatment
- Documentation review to confirm the chart supports medical necessity
- Code selection across CDT, CPT, and ICD-10 where applicable
- Payer-specific submission logic including attachments and narratives
- Denial management when payers push back on diagnosis, coverage, or documentation
- Payment posting and follow-up so balances don't age unnecessarily
If your internal team still treats this as a side task, that's the problem. The operational demands are closer to advanced medical RCM than basic dental claim handling. If you need a refresher on how specialized claim work differs from generic admin support, this breakdown of what medical billers do is a useful reference point.
Understanding the Dental vs Medical Reimbursement Divide
Dental and medical reimbursement are two different countries. They use different languages, different border rules, and different definitions of what deserves payment. Practices lose money when they assume crossing from one to the other is just a matter of changing a claim form.
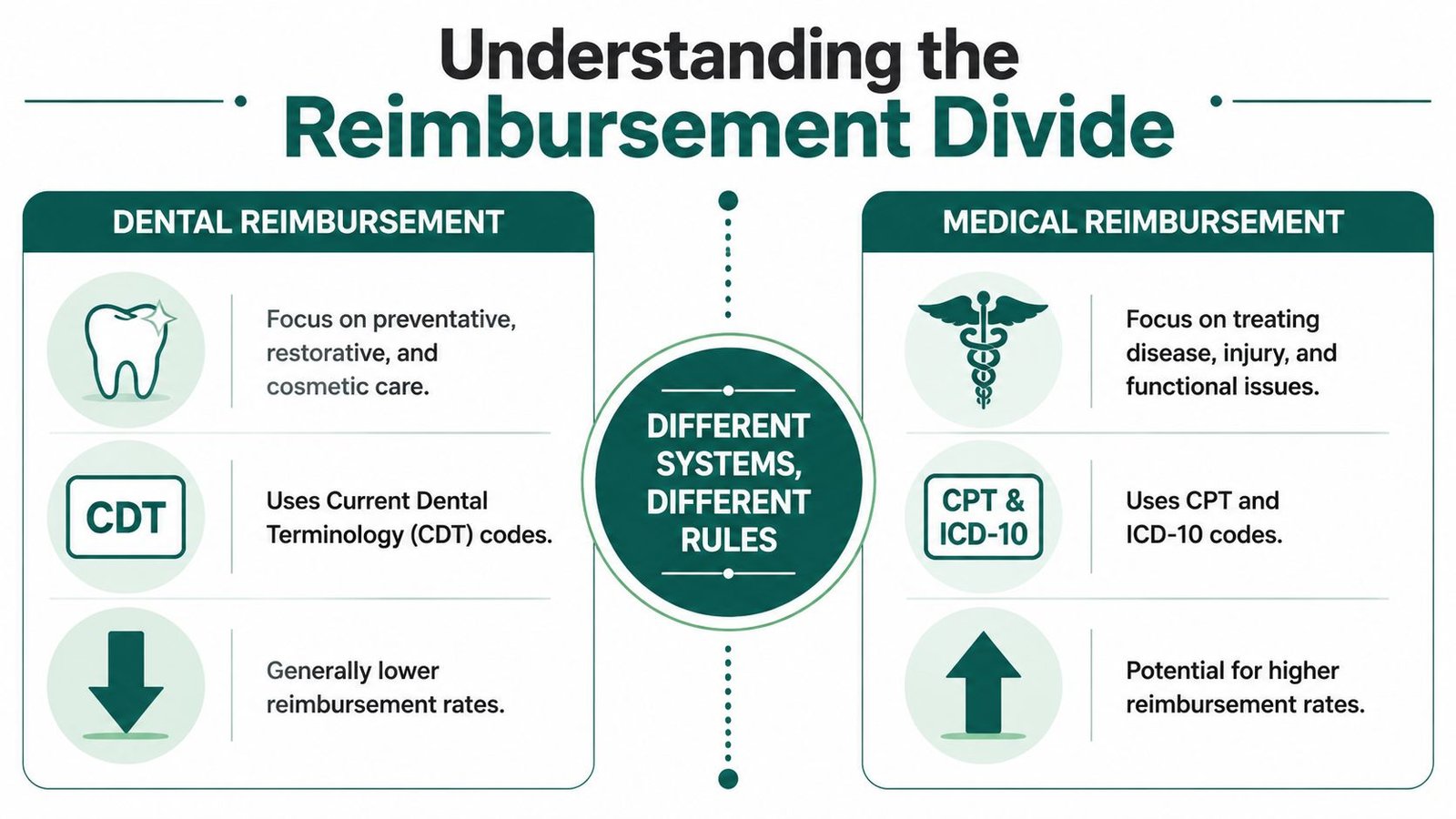
According to CE Computech's overview of dental and medical billing, dental claims typically use CDT codes and are paid through dental plans that often have annual limits of about $1,500 to $2,000, while medical claims use CPT and ICD-10 codes and are generally paid by medical insurers based on medical necessity rather than the same annual maximum structure.
Why that difference changes your economics
A dental plan asks, "Is this a covered dental benefit, and has the patient hit plan limits?"
A medical plan asks, "Is this medically necessary, supported by diagnosis, and documented to payer standards?"
Those are not minor variations. They change how your staff verifies benefits, how the provider documents the visit, and how quickly your claim gets paid or denied.
Here's the practical split:
| System | Core code set | What drives payment | Owner impact |
|---|---|---|---|
| Dental billing | CDT | Plan design, annual limits, frequency rules | Faster for routine dentistry, but limited upside on medically necessary cases |
| Medical billing | CPT and ICD-10 | Medical necessity, diagnosis support, payer policy | More administrative work, but broader reimbursement opportunity for the right cases |
Why cross-coding isn't enough by itself
A lot of practices hear "cross-code it" and think the work is done. It isn't. Translating a dental procedure into a medical claim is only part of the process. The chart, diagnosis specificity, and payer-facing story all have to line up.
That's why the claim often lives or dies before submission. If your chart can't explain why the service addressed disease, dysfunction, pain, trauma, or airway compromise, the payer treats it as dental, even if the procedure feels medically obvious to the clinician.
The claim has to make sense in the medical payer's logic, not just in the operatory.
Owners who want a cleaner understanding of how documentation travels across reimbursement workflows should also understand the role of a superbill in medical billing, especially when diagnosis and procedural support need to be tied together clearly.
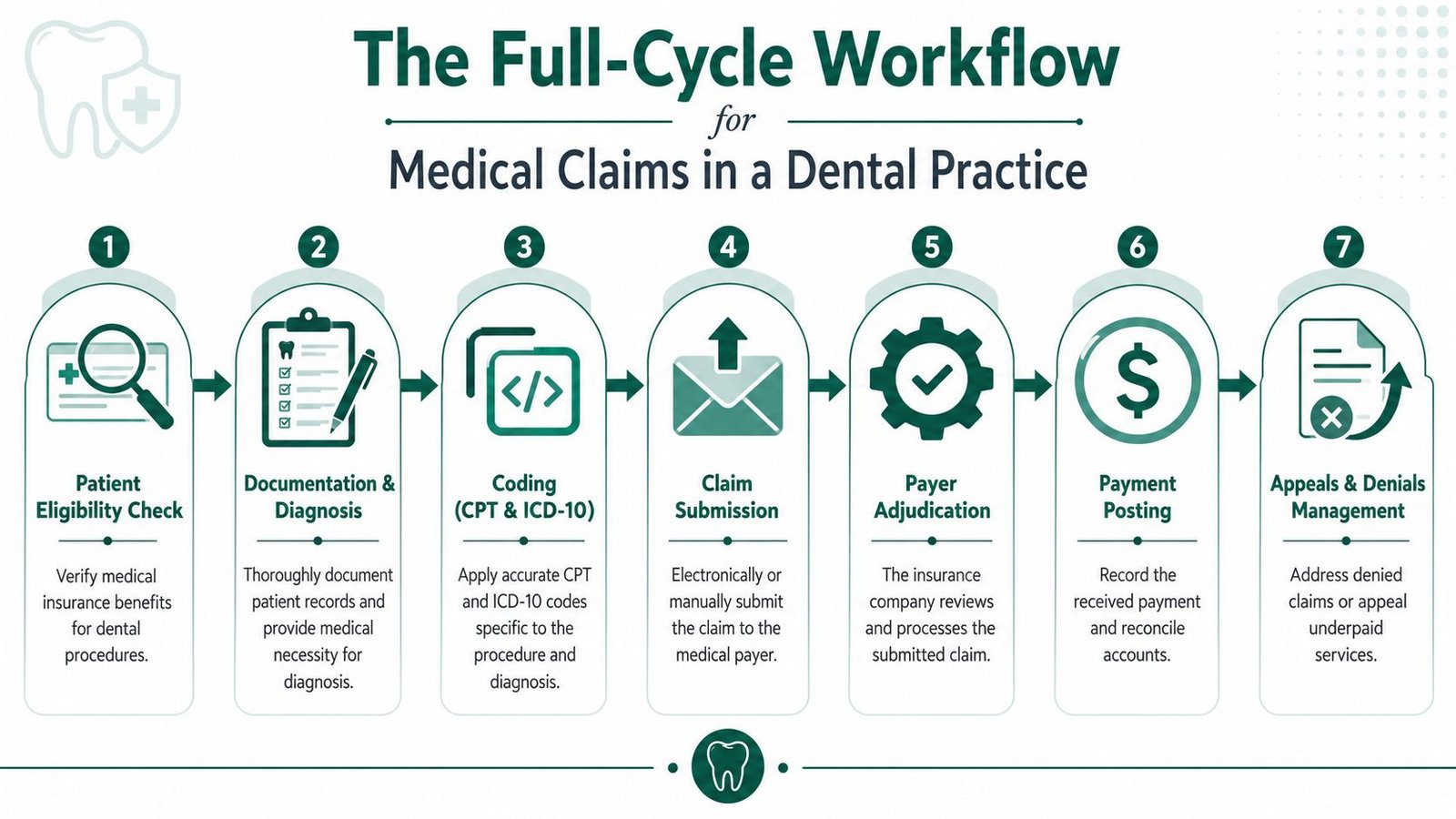
The Full-Cycle Workflow for Medical Claims in a Dental Practice
A medical claim in a dental office succeeds or fails long before payment posts. The owner who treats this as a front-desk task leaves money on the table and creates denial risk that spreads across scheduling, documentation, coding, and follow-up.
The practical question is simple. Which cases justify the extra work of a medical claim, and does your team have the process to collect that reimbursement without creating rework, write-offs, or compliance exposure?
Use this workflow to answer that question before treatment starts.
Start with case selection, not claim submission
Owners lose margin when they send every borderline case through medical billing. They also lose margin when they default everything to dental and miss reimbursable medical cases. The right filter is financial and operational.
A case belongs in the medical lane only if three conditions are true:
- The clinical story supports medical necessity
- The expected reimbursement exceeds the extra labor and documentation cost
- Your team can meet the payer's rules before and after treatment
That framework matters. An emergency trauma case, biopsy-related service, sleep-related appliance workup, or surgery tied to pathology may justify medical billing. A routine restorative procedure with no medical necessity usually does not. Owners need this decision made consistently, not by gut instinct at the front desk.
Step one is benefits and policy review
Eligibility alone is not enough. Your team needs to verify the policy terms that control payment. That includes prior authorization requirements, referral rules, diagnosis limitations, attachment requirements, place-of-service rules, and whether the payer expects the service to process through medical at all.
Miss this step and you create expensive failure. The patient gets treated, the claim gets denied, and your staff spends weeks trying to fix a case that was never positioned correctly.
Give one person ownership here. If three employees touch verification and nobody is accountable for the final answer, errors multiply.
Step two is provider documentation
Medical payers pay for a documented medical problem and a documented reason for treatment. They do not pay because the office completed a procedure that feels obviously necessary to the clinician.
Your record needs to show:
- The diagnosis and why it is medically relevant
- Symptoms, functional impairment, trauma, infection, pathology, or pain
- Exam findings and treatment rationale
- Attachments that match the narrative, such as imaging reports, pathology reports, or referral notes
- Consistency across the chart, claim form, and supporting documents
Weak documentation causes two separate losses. The first is the denial you see now. The second is the recoupment you get later after an audit.
Step three is coding and claim construction
This is the point where many dental offices underperform. They treat coding as a translation exercise instead of a reimbursement decision with compliance consequences.
The claim has to connect the procedure, diagnosis, provider note, and attachments into one payer-ready story. If that chain breaks, the payer classifies the case as dental, investigational, cosmetic, or unsupported. Then payment stops.
A good coder does more than select codes. A good coder checks whether the case should be billed medically at all. That discipline protects ROI. It also prevents your staff from spending forty minutes building a claim that had no realistic path to payment.
Medical coding logic will feel more familiar to teams that already work with specialty RCM models such as orthopedics billing support, where diagnosis specificity and documentation depth directly affect reimbursement.
If the chart, diagnosis, and code set do not tell one clear medical story, the claim is weak before it ever leaves your office.
Step four is submission, tracking, and fast correction
Electronic claim submission is now standard across healthcare administrative workflows, as the Centers for Medicare & Medicaid Services explains in its overview of administrative simplification electronic transactions. Speed helps, but speed does not rescue a bad claim.
Watch these checkpoints closely:
- Was the claim accepted by the clearinghouse and payer
- Did the payer request records or issue a development letter
- Was the request answered within the payer's deadline
- Did payment match the expected allowed amount
- Was any denial appealed with payer-specific support instead of a generic resubmission
This part of the workflow should run on deadlines, not memory.
Step five is payment posting and A/R control
A paid claim can still be underpaid. A denied claim can still be recoverable. An ignored pended claim turns into old A/R fast.
Owners should track where claims stall. Is the problem front-end verification, provider notes, coding quality, missing attachments, or follow-up discipline? If you cannot identify the choke point, you cannot fix the margin leak.
That is why integrated revenue cycle management across the full claim lifecycle matters. Medical billing from a dental practice only works when verification, documentation, coding, submission, posting, and appeals operate as one controlled process.
The payoff is real when you apply this workflow selectively. The wrong cases create admin cost. The right cases create new reimbursement that dental billing alone would never capture.
Common Coding Traps and Payer Denials to Avoid
Most denials in dental medical billing aren't bad luck. They're predictable. The practice either billed a dental service as if medical necessity were obvious, or it submitted a medical claim without the documentation and code coordination the payer requires.
According to DentalBilling.com's review of dental billing companies, successful dental medical billing hinges on correct CDT-to-CPT/ICD-10 coordination, and medical payers require a medically necessary diagnosis plus supporting documentation. Without that, denials increase and post-payment recoupments become more likely.
The biggest traps we see
Here are the mistakes that usually hurt owners the most:
- Routine diagnosis logic on a medical claim. If the diagnosis reads like ordinary dental maintenance, the payer has no reason to process it in the medical lane.
- No proof of medical necessity. A provider may know the case is functional or pathology-driven, but if the chart doesn't say that clearly, the claim is weak.
- Incomplete attachments. Medical payers often need records that a dental team doesn't routinely package well.
- Mismatch between documentation and codes. The narrative says one thing, the diagnosis suggests another, and the procedure code points somewhere else.
- Failure to anticipate payer edits. Some payers are strict about diagnosis specificity, prior review, or documentation sequencing.
Specific examples owners should recognize
An oral appliance case tied to sleep-disordered breathing can look financially attractive until the claim is filed without the clinical support the payer expects. Then reimbursement stalls, staff spends weeks chasing records, and the balance shifts back to the patient or gets written down.
TMJ-related care creates a similar problem. The clinical team may treat it as clearly functional, but many payers scrutinize whether the record supports a medical condition rather than a dental occlusion issue. If the note doesn't establish symptoms, failed conservative measures when relevant, and a medically necessary rationale, pushback is common.
Bone grafting and trauma-related oral surgery also expose the same weakness. The procedure may feel self-explanatory to the surgeon. The payer still wants a claim built in medical language.
Owners should read denial reports less like billing paperwork and more like a map of training failures.
A useful companion resource is this summary of the top denial categories in medical billing. It helps owners connect recurring denials to upstream process issues rather than blaming the payer every time.
What to fix first
If your denial stack is growing, don't start by yelling at the billing team. Audit these three areas first:
- Pre-visit qualification. Did anyone confirm the case met medical billing criteria?
- Provider documentation. Did the note support diagnosis, severity, and necessity?
- Claim assembly. Did coding, narrative, and attachments tell the same story?
Fix those first. Appeals work better when the original workflow was disciplined. They work poorly when the original claim was never defensible.
How to Evaluate a Dental Medical Billing Partner
Most vendors will tell you they can "do dental medical billing." That statement is worthless unless they can show how they protect revenue, control denials, and keep claims moving without turning your staff into a cleanup crew.
One source puts outsourced dental billing around $1,500 to $1,600 per month, but Dental Claim Support's outsourcing overview correctly notes that the price means very little without performance benchmarks. Owners should judge a partner on denial reduction, days in A/R, and clear ROI, not on the monthly fee alone.
The questions that actually matter
When you interview a billing partner, ask questions that expose operating reality:
- What case types do you handle regularly. If your mix includes oral surgery, airway-related treatment, pediatrics, or medically necessary restorative care, general billing experience isn't enough.
- Who owns denials and appeals. If the vendor submits claims but leaves appeals to your staff, that's not full-cycle support.
- How do you report performance. You want plain-English visibility into claim status, denials, aging, and collection progress.
- How do you handle payer-specific rules. A real partner should describe workflow discipline, not vague "we know the industry" language.
- How do you work inside our current systems. If the answer sounds like a software migration pitch, be careful.
Red flags owners should not ignore
We have seen practices sign with vendors that looked affordable and created expensive chaos. Watch for these warning signs:
| Red flag | What it usually means |
|---|---|
| They talk mostly about low fees | They compete on price because they can't prove outcomes |
| Reporting is vague or delayed | You won't know where cash is stuck until A/R ages |
| They avoid specialty examples | They probably lack true dental-medical depth |
| Appeals are excluded or limited | Your team will inherit the hardest work |
| They want you to change systems immediately | Their process may not adapt well to your operation |
A billing partner should reduce management burden. If they create more meetings, more exceptions, and more staff confusion, they aren't solving the right problem.
Before you sign anything, compare their answers against a structured vetting list like these questions to ask a medical billing company before hiring. If your current operation already feels opaque, a practical next step is to get a baseline through a free billing audit so you can measure any vendor against your actual leakage.
Understanding Pricing Models and EHR Integration
Owners often overfocus on vendor price and underfocus on fit. That's backwards. The wrong pricing model distorts incentives, and the wrong integration approach slows your front office, frustrates providers, and creates more rework than the outsourcing relationship is worth.
How pricing models affect behavior
You'll usually encounter three broad approaches.
Percentage of collections aligns the vendor with getting claims paid. That can work well if your case mix is complex and follow-up intensity matters. The risk is that some vendors chase easier claims and underinvest in harder appeals unless expectations are written clearly.
Flat monthly pricing gives cost predictability. It can be useful when claim volume is stable and the scope is clearly defined. The problem is obvious. If your denial workload spikes, a flat-fee vendor may have little financial incentive to spend more time on your account.
Per-claim or hybrid pricing can make sense if you want a tighter link between activity and cost. But owners need to look closely at what's excluded. Eligibility work, documentation review, appeals, and patient balance support often sit outside the advertised fee.
The right question isn't "What's your rate?" The right question is "What work is included, who owns the difficult claims, and how will this affect our collections and A/R?"
Integration should be boring
A strong partner should work inside your existing practice management and billing environment through secure access, established workflows, and disciplined communication. You shouldn't need a disruptive platform migration just to improve claim performance.
That matters because dental medical billing depends on the quality of documentation as much as the claim itself. If your charting process is messy, your billing will stay messy. That's why practices looking to tighten records and narratives often also invest in ways to streamline healthcare documentation before or during an RCM cleanup.
What owners should insist on
Ask for a plain-language implementation plan that answers:
- Who logs into what system
- How claims, notes, and attachments are exchanged
- How your staff escalates urgent payer issues
- What training is needed for schedulers, providers, and front-desk staff
- How reporting reaches leadership
If the integration plan sounds complicated, daily execution will be worse. Billing support should simplify operations, not create an IT project.
Frequently Asked Questions by Practice Owners
Owners ask these questions because the margin impact is real. A medically billable case handled the wrong way can turn a payable claim into write-off work, staff overtime, and patient frustration.
How do I know whether a procedure belongs under medical billing or dental billing
Start with a business test, not a coding test. Will medical necessity be clear in the chart, will the payer likely recognize the diagnosis-treatment link, and will the expected reimbursement justify the extra work for eligibility, records, attachments, and follow-up?
If the answer is weak on any of those points, bill dental first or do not build a medical workflow around that procedure. Practices lose money when they chase medical claims for cases with thin documentation, vague diagnoses, or low reimbursement potential. The training gap is real, as discussed in Dental Economics' article on bridging the gap in medical billing for dentistry. The article is useful because it highlights the same issue owners face every day. medical billing can expand reimbursement, but only when the clinical story and claim support are strong enough to survive payer review.
A simple rule works well. If your provider cannot explain the diagnosis, functional impairment, prior conservative treatment, and reason this procedure is medically necessary before treatment, do not expect a profitable medical claim after treatment.
Should I outsource dental medical billing or build it in-house
Outsource when your practice has enough medically eligible volume to matter, but your team lacks medical claim discipline. Build it in-house only if you already have staff who can handle benefit verification, diagnosis-based documentation review, coding selection, attachment assembly, denial management, and payer follow-up without pulling attention away from front-desk operations.
This is a capacity decision as much as a skill decision.
A busy scheduler or treatment coordinator should not be learning medical billing between phone calls and patient check-ins. That setup creates preventable denials and slow cash.
What should I watch first if claims aren't getting paid
Watch three numbers first. Denial categories, days in A/R, and claims stuck in a records or payer-response status.
Those reports tell you where the breakdown sits. A spike in medical necessity denials points to qualification or documentation. A pile of unsubmitted or pended claims points to operational bottlenecks. Rising A/R with low denial visibility usually means follow-up is weak and no one owns the aging inventory.
Is medical billing always worth it for a dental practice
No. It is worth it when the practice performs enough medically necessary procedures, documents consistently, and can manage the extra administrative load without disrupting core dental collections.
Here is the decision standard I recommend. Estimate how many cases per month are medically supportable, what each claim is likely to collect, how long your team or vendor will spend getting that claim paid, and what denial rate you can realistically control. If that math does not produce a clear return, do not force a medical billing program. If it does, commit to it fully and treat it like a revenue channel, not an experiment.
If your practice performs medically necessary care in a dental setting and you're not sure whether your current workflow is collecting everything it should, Happy Billing can help you find the leakage quickly. Their team works inside your existing systems, audits denials and aging A/R, and gives you a practical path to improve reimbursement without forcing a disruptive overhaul.