CMS Anesthesia Billing Guidelines for Practice Owners
CMS anesthesia billing guidelines are not built on a simple fee schedule. CMS pays anesthesia claims through a formula using base units, time units, and modifiers, and errors inside that formula are one of the fastest ways anesthesia practices lose revenue.
If your group is seeing avoidable denials, unexplained payment variance, or aging A/R, the problem often starts with those three inputs. A claim can look complete and still underpay if the wrong anesthesia code is chosen, the time record is incomplete, or the modifier doesn't match the clinical service. For owners and administrators, that means CMS anesthesia billing guidelines are not just a compliance issue. They are a cash flow issue.
Why Anesthesia Billing Guidelines Matter More in 2026
The reimbursement environment got tighter, not easier. The CY 2026 Physician Fee Schedule Final Rule set the anesthesia conversion factor at $20.4976 for most physicians, a 0.88% increase over 2025, but the same CMS-linked analysis projected an overall 1% revenue decline for anesthesia because CMS also finalized a 2.5% efficiency adjustment that reduces RVUs for non-time-based services. That same analysis noted a 7% payment reduction for facility services and a 4% increase for non-facility services, which changes the economics of where care is delivered and how efficiently claims have to move through the revenue cycle (analysis of the 2026 CMS final rule for anesthesia).

That matters because anesthesia practices don't have much room for operational leakage. A small payment shift at the fee schedule level becomes more painful when your own workflows are already giving away units, delaying claims, or triggering rework.
What owners should watch first
Three pressure points show up quickly in audits:
- Time capture drift: Start and stop times aren't consistently documented, so billed time doesn't fully reflect care delivered.
- Modifier mismatch: The record supports one level of anesthesia service, but the submitted modifier tells Medicare something else.
- Bundling errors: The practice bills anesthesia separately in scenarios where Medicare treats it as part of the primary procedure.
Practical rule: When reimbursement gets tighter, billing accuracy stops being a back-office metric. It becomes margin protection.
The operational response isn't complicated, but it has to be disciplined. Owners should review denial categories, compare clinical time records to billed units, and look for recurring write-offs tied to anesthesia-specific edits. If your team needs a framework for that review, these revenue cycle management best practices for physician groups are a good place to start.
The hidden risk in a "mostly clean" process
Many practices assume their billing is fine because claims are going out. That standard is too low. In anesthesia, a process can be "working" while still producing underpayments, extra touches, and delayed collections.
The 2026 environment makes that expensive. If CMS policy is already compressing revenue, your billing operation can't also be leaking it.
The Core Anesthesia Billing Formula Explained
CMS anesthesia payment is built differently from most physician reimbursement. For anesthesia CPT codes 00100 to 01999, Medicare uses a model based on base units, time units, and modifier-based adjustments, then applies the relevant conversion and geographic factors to calculate the allowed amount. CMS also states that anesthesia for those codes must not be unbundled into component services, and Medicare generally doesn't pay separately when the same physician furnishes both the anesthesia and the medical or surgical procedure (CMS anesthesia payment framework summarized here).
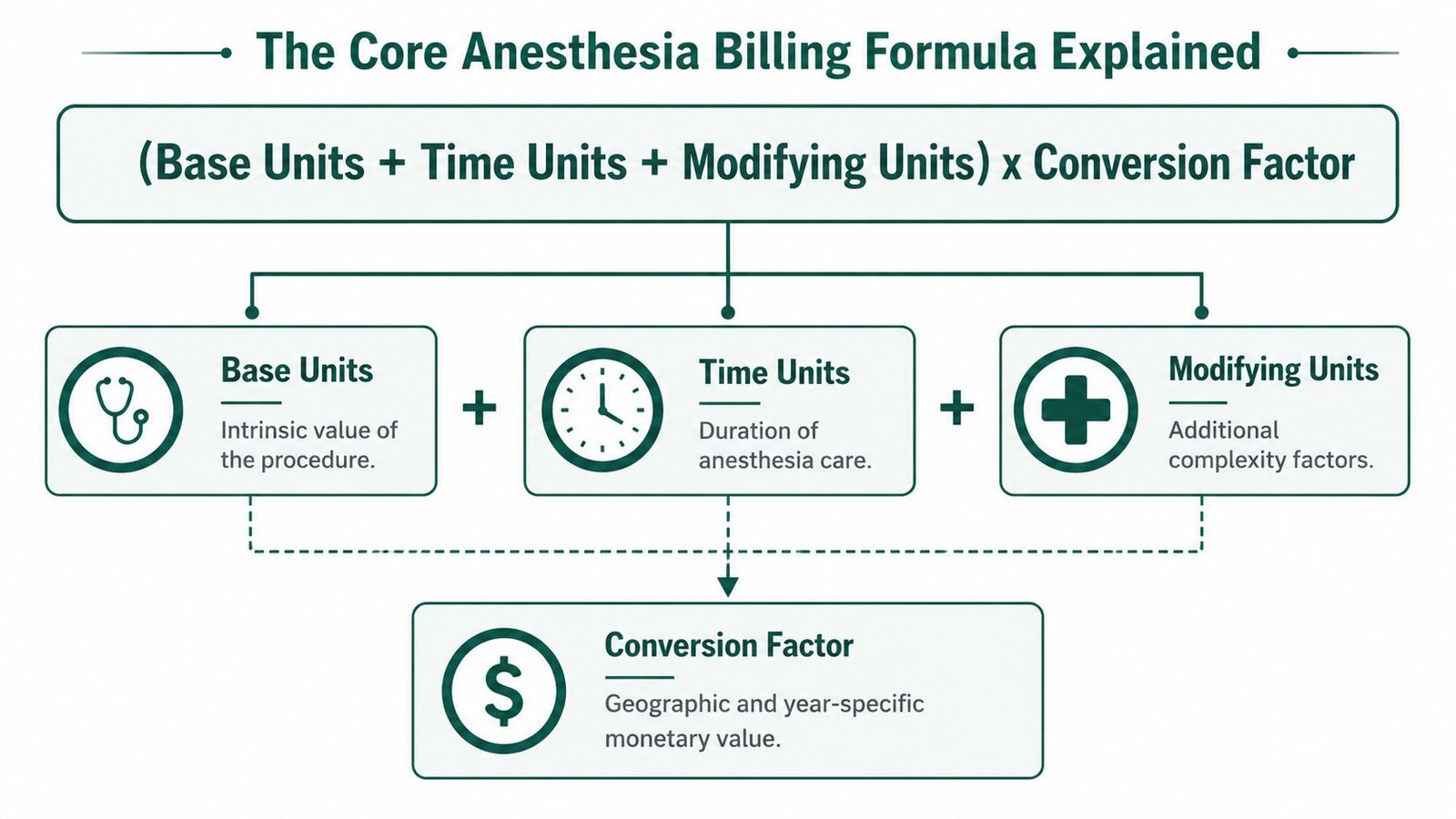
That formula sounds technical. Financially, it's simpler than it looks. Each part is a revenue lever, and each part can fail.
Base units determine the starting value
The anesthesia CPT code establishes the claim's starting point. If the wrong anesthesia code is selected from the 00100 to 01999 range, the claim starts from the wrong valuation before time and modifiers are even considered.
For owners, this is why code selection cannot be treated as clerical cleanup. The code has to reflect the actual anesthetic service tied to the encounter. In radiology, CMS also notes that only one anesthesia code is generally reported for a radiological encounter even when multiple imaging procedures occur in the same session. If your team reports anesthesia more than once for a single anesthetic episode in that setting, you've created compliance risk and invited payment reversal.
Time units are where small misses become real money
Time documentation is not a side note in anesthesia billing. It is part of the payment formula. Medicare uses documented anesthesia time to derive payable units, which means incomplete or inconsistent start and stop times can reduce reimbursement or trigger denials.
Owners usually feel this problem in two ways:
| Revenue leak | What it does to the practice |
|---|---|
| Incomplete time record | Lowers billed units or sends the claim to manual review |
| Inconsistent time across records | Creates denials, rework, and slower collections |
| Late documentation finalization | Delays claim submission and extends A/R |
When we audit anesthesia claims, the most expensive mistakes are often the least dramatic. Missing minutes, wrong code selection, and preventable bundling errors create steady leakage.
Modifier-based adjustments finish the story
Modifiers tell Medicare how the service was delivered. If the modifier doesn't match the documentation, the claim can be paid incorrectly, denied, or reprocessed later.
This is why a practice owner should care about billing logic, not just billing volume. More cases don't automatically mean more revenue if the claims don't capture the full service correctly. A useful benchmark for reviewing that logic is to compare your current workflow against broader RCM strategies for physician practices, then isolate the anesthesia-specific failure points.
How Key Modifiers Impact Your Bottom Line
Modifiers are where anesthesia claims often move from payable to problematic. A clean anesthesia record can still produce the wrong payment if the modifier logic is weak, and owners usually don't see that until denials pile up or payer recoupments start appearing.
Two categories deserve close executive attention: modifiers that describe the anesthesia service itself, and modifiers that affect how Medicare interprets the claim in the context of coverage and payment rules.
The QS modifier is not optional when CMS requires it
For Medicare claims involving monitored anesthesia care, CMS policy requires the QS modifier when MAC is provided for procedures commonly associated with MAC. CMS also states that Medicare anesthesia billing uses the date anesthesia time begins, with units reflecting the total anesthesia time in minutes. If the modifier and time documentation don't align with the actual service, the claim can reject or be reprocessed at a lower payment level (CMS MAC billing guidance).
For a practice owner, the takeaway is direct. MAC documentation has to support MAC billing. If your record describes one service and your claim submits another, you don't just risk a denial. You create extra touches, delayed cash, and payer scrutiny on similar future claims.
Modifier errors create two kinds of financial damage
The first kind is immediate. The claim doesn't pay correctly.
The second kind is slower and usually more expensive. The payer starts treating your anesthesia claims as higher-risk, which means more requests, more rework, and longer collection cycles.
A practical way to think about modifier controls:
- Clinical match: The modifier has to reflect what the record supports.
- Timing match: The time record has to be complete enough to support the billed anesthesia episode.
- Scenario match: Radiology and MAC encounters need special attention because CMS applies specific billing limitations and expectations.
A modifier is a payment instruction, not just a claim detail. If it's wrong, the rest of the claim can be right and you still won't like the result.
What works and what doesn't
What works is a simple pre-bill checkpoint where the claim cannot move forward unless the anesthesia type, minutes, and modifier are consistent.
What doesn't work is relying on downstream denial management to catch errors after submission. That approach turns a preventable front-end issue into an A/R problem.
If your internal team doesn't have a modifier review protocol, start with a tighter workflow around the anesthesia-specific scenarios that trigger the most rework. This anesthesia modifier reference for practice operations can help frame the review around payment impact rather than coding theory.
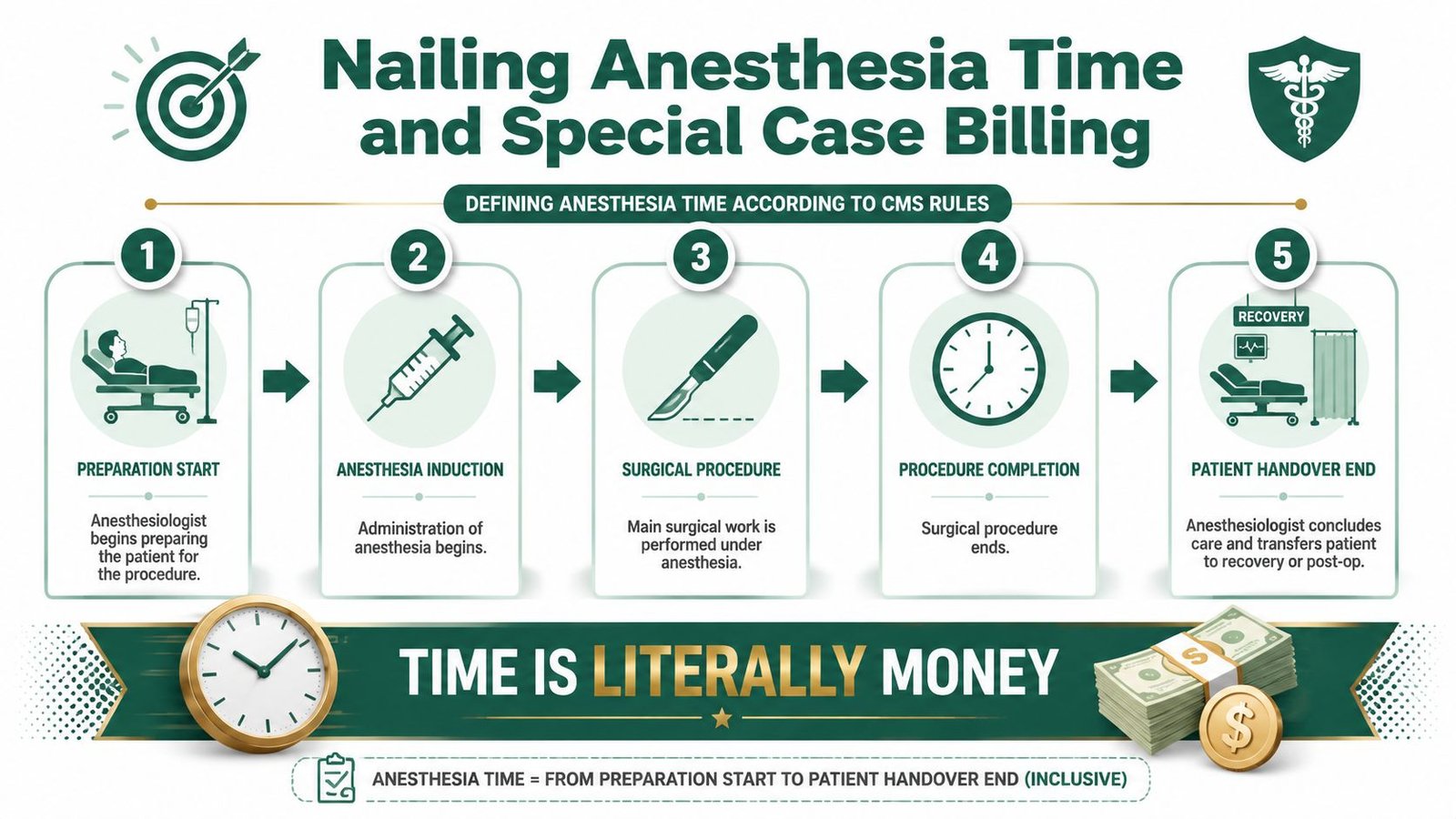
Nailing Anesthesia Time and Special Case Billing
In anesthesia, time is one of the few parts of the claim that directly moves payment and compliance risk at the same time. Medicare billing units reflect total anesthesia time in minutes from the start of care, so if your record is vague, inconsistent, or finalized late, you are putting both reimbursement and collectability at risk.
The practical problem isn't only underbilling. It's operational drag. Claims with questionable time records often sit longer, require staff intervention, and age into avoidable A/R.
Minute-accurate records protect revenue
The safest workflow is also the most efficient one. Capture anesthesia start and stop times clearly in the clinical record, reconcile them before claim creation, and hold any claim where the timeline is incomplete.
Owners should ask for routine reporting on these points:
- Missing timestamps: Claims held because the record lacks a clear beginning or end to the anesthesia episode.
- Cross-record mismatch: Cases where the anesthesia record and related encounter documents don't line up.
- Late finalization: Records signed after the expected billing window, which slows claim release.
A surprisingly large share of denial work starts here. Not because the service wasn't provided, but because the file didn't prove it cleanly enough for payment.
MAC cases are high-risk when workflows are loose
CMS is clear that QS is required for certain Medicare MAC claims, and that minute-based time reporting drives units. That creates a narrow lane for clean billing. The record must support MAC, the modifier must reflect MAC, and the minutes must cover the full anesthesia encounter.
When one of those pieces is off, practices usually see one of three outcomes:
| Failure point | Likely financial effect |
|---|---|
| QS missing when required | Claim rejection or avoidable follow-up |
| Time not fully documented | Lower payment or payer reprocessing |
| Documentation suggests a different anesthesia service | Medical necessity or payment edits |
Special scenarios need claim discipline
CMS also allows only one anesthesia code for radiology encounters even when multiple imaging procedures occur during the same session. That matters operationally because some internal workflows accidentally mirror procedural billing logic and duplicate anesthesia reporting across the encounter. Medicare doesn't want the anesthetic episode reported that way.
Clean anesthesia billing is usually boring. One code where CMS expects one code. One accurate time record. One modifier set that matches the chart.
The owners who improve cash flow fastest are usually the ones who stop treating time capture as a documentation issue and start treating it as a revenue control.
Preventing Common Denials with Bulletproof Documentation
A denied anesthesia claim usually isn't born in billing. It starts in the chart, then passes through charge capture, then reaches the payer carrying the same unresolved defect. By the time the denial appears, your practice has already spent money on the case, spent staff time on the claim, and delayed payment for work already performed.
That is why the best denial strategy in anesthesia is documentation design. For practices struggling with denials in anesthesiology billing, the record has to support the exact claim CMS expects to see.

The five documentation failures that hurt revenue most
These are the patterns we see most often when auditing anesthesia revenue cycle performance.
Time is present, but not defensible
A start time and stop time may exist, but they don't appear reliable when compared against the rest of the encounter. If the timeline doesn't read cleanly, the payer has a reason to deny, pend, or reprocess.
Prevention tip: Build a pre-bill edit that compares the anesthesia time record against the rest of the encounter documentation before the claim leaves your system.
The anesthesia code doesn't fit the encounter
CMS payment for anesthesia hinges on choosing the correct code within 00100 to 01999. If the claim starts with the wrong anesthesia code, everything that follows is built on a weak foundation.
Prevention tip: Review anesthesia code assignment as a revenue control, not just a coding task. High-dollar denial prevention often starts with the first field on the claim.
The modifier doesn't match the service
MAC encounters are especially vulnerable here. If the record supports monitored anesthesia care but the modifier logic doesn't reflect the Medicare requirement, payment becomes unstable.
Prevention tip: Require claim review when the anesthesia type documented in the record and the modifier selected on the claim are not an exact match.
A short checklist owners can actually use
Ask your team whether every Medicare anesthesia claim can answer yes to these questions before submission:
- Is the anesthesia CPT code in the correct 00100 to 01999 range and supported by the encounter?
- Are the anesthesia start and stop times complete, legible, and internally consistent?
- Does the modifier set match the service documented in the chart?
- Is the claim free of separate anesthesia billing in a scenario Medicare treats as bundled?
- For radiology, is the anesthetic episode reported once rather than duplicated across multiple imaging procedures?
That last point gets missed more than owners expect. CMS states that, in general, only one anesthesia code is reported for radiological procedures even when multiple imaging procedures occur in the same encounter. A workflow that duplicates the anesthesia claim line across the session may look productive internally, but it creates external repayment risk.
Strong documentation doesn't just win appeals. It prevents the appeal from being necessary.
What bulletproof documentation looks like in practice
The record should make the claim obvious. A payer reviewer should be able to see what service was delivered, how long it lasted, and why the billed modifier makes sense without hunting through conflicting notes.
That usually requires tighter coordination between clinicians, charge entry, and claim QA. In many practices, each team assumes the next team will catch problems. That handoff mentality is exactly what extends A/R.
A better model is a closed loop:
- Clinician documents the anesthesia episode clearly.
- Charge capture mirrors that documentation without improvising.
- Pre-bill review checks time, code, and modifier alignment.
- Claims with discrepancies are corrected before submission, not after denial.
Documentation standards that reduce rework
The most effective documentation improvements are usually simple.
- Use one authoritative time source: Don't let multiple timestamps compete without resolution.
- Standardize MAC documentation: If your group bills MAC to Medicare, make sure the clinical record consistently supports the required claim logic.
- Flag bundled scenarios early: If Medicare generally bundles the anesthesia service into the primary procedure when the same physician furnishes both services, your billing system should not wait until denial to recognize that issue.
- Treat radiology anesthesia separately in workflow design: The one-code expectation should be built into your claim edits.
Owners don't need to micromanage each chart. They do need visibility into whether those controls exist and whether they're being enforced.
The A/R connection most groups miss
Denials are obvious. Slow pays caused by weak documentation are quieter. The claim gets touched more times, sits in a work queue longer, or gets paid only after repeated follow-up. Those cases may not show up as clean denial statistics, but they still lengthen A/R and increase collection cost.
This is why documentation quality should be reviewed alongside operational KPIs. If your team is focused only on charge lag or payment posting speed, you're measuring the downstream effects without addressing the upstream cause. Stronger medical billing denial management processes help, but they work best when paired with documentation controls that prevent the denial in the first place.
If these issues sound familiar, a targeted review of your workflow usually surfaces the leakage quickly. Practices that want an outside view of missed units, modifier errors, and preventable denials can request a no-cost billing audit to identify where revenue is slipping before another quarter closes.
Anesthesia Billing FAQs for Practice Owners
Practice owners usually don't need another coding lecture. They need to know where to focus first, what to monitor, and when internal fixes stop being enough.
A good operating rule is this: if the same anesthesia denial pattern shows up repeatedly, the problem is not staff effort. It is process design.
For leaders comparing internal cleanup to outside support, these anesthesia medical billing service considerations can help frame the decision around control, speed, and financial impact.
What should I audit first if my anesthesia revenue feels low?
Start with the claims most likely to hide leakage rather than the claims already denied. Review whether billed minutes match the final anesthesia record, whether MAC cases carry the expected modifier logic, and whether any radiology encounters are being reported with duplicate anesthesia coding. If you find recurring mismatches, you've identified a front-end process problem, not a one-off claim issue.
How do I know whether to fix billing in-house or outsource it?
Look at repeatability. If your current team can identify the root cause of denials, correct workflow defects, and keep those problems from returning, an internal rebuild may work. If the same issues keep cycling through A/R, outside review often becomes the faster path because it exposes the gaps between documentation, charge capture, and claim submission.
Which CMS rule creates the most financial risk?
For many practices, it's not one rule. It's the interaction of three. The anesthesia claim has to use the correct anesthesia code, the time record has to be complete, and the modifier has to match the service. When any one of those breaks, payment can drop, denial risk rises, and staff spend more time fixing avoidable errors.
How should I judge whether my anesthesia billing operation is healthy?
Don't judge it only by whether claims are going out. Judge it by whether claims are going out right the first time, whether your team can explain payment variance quickly, and whether documentation defects are being caught before submission rather than after denial.
If your anesthesia practice is losing revenue to time capture gaps, modifier errors, or Medicare-specific billing defects, Happy Billing can help you pinpoint the leak. We combine specialty-specific anesthesia billing expertise with hands-on revenue cycle review, and we can show you where your current process is slowing cash or creating preventable denials.