Medical Bill Negotiation Services: Maximize Practice Revenue

If your practice has balances sitting in A/R that your team has already touched three times, medical bill negotiation services can be a smart revenue recovery tool. Used correctly, they help turn disputed payer balances, aged self-pay accounts, and stalled underpayments into cash without defaulting every difficult account to write-off or collections.
For an independent practice owner, this is not a patient advocacy topic. It is an RCM decision. If denials are climbing, payer variance is showing up in remits, or old balances are dragging out your cash cycle, negotiation affects net collections, denial recovery, and A/R days directly. We've seen practices treat negotiation as a last resort when it should often sit inside a broader escalation strategy for unresolved accounts.
What Are Medical Bill Negotiation Services
A practice owner usually encounters this need in a familiar moment. The monthly aging report lands on your desk. A block of balances looks too old to trust, too large to ignore, and too labor-intensive for your front office to keep chasing. At that point, medical bill negotiation services become less about “asking for discounts” and more about recovering revenue that ordinary follow-up no longer moves.
In practice, these services sit between standard billing operations and hard collections. They review accounts that have stalled, identify whether the obstacle is a payer issue, a pricing issue, a documentation issue, or a patient-balance issue, and then pursue a structured resolution.
What they do differently
A negotiation partner is not the same as a traditional collections vendor.
Collections agencies usually work after the relationship has already deteriorated. Negotiation services work earlier and more strategically. They look for recoverable value in accounts that internal staff may have already categorized as difficult, especially when the account still has room for repricing, correction, appeal, or a managed settlement.
That matters because every unresolved balance has a revenue-cycle cost. It ties up staff time, distorts forecasting, and normalizes preventable write-offs.
A strong overview of the broader workflow sits in this healthcare revenue cycle management guide, but negotiation belongs in a narrower category. It is an escalation function for accounts where standard claim submission and routine statements have already failed.
Where negotiation fits inside practice finance
For a practice, the most useful way to define medical bill negotiation services is this:
- Payer-facing recovery: Challenging underpayments, incorrect bundling, contractual misapplication, or closed claims that still have a valid reopening path.
- Patient-balance resolution: Auditing balances for errors, validating responsibility, and restructuring payment in a way that preserves both recovery and goodwill.
- Aged A/R salvage: Pulling cash out of accounts your internal team no longer has time or ability to move.
Practical rule: If an account is old because nobody knows what to do next, it is a negotiation candidate. If an account is old because the underlying balance is wrong, it is an audit candidate first.
That distinction matters. A practice that sends the wrong account to the wrong vendor loses twice. First in missed recovery. Then in damaged patient experience or avoidable contractual write-off.
If you're sorting through that line between valid balance and flawed balance, this overview of medical bill review services is the right companion process to understand before assigning accounts out.
How Medical Bill Negotiation Works for Practices
Most practice owners hear “negotiation” and think someone calls a payer or patient and asks for a reduction. That's not how effective recovery works. The advantage comes from evidence.
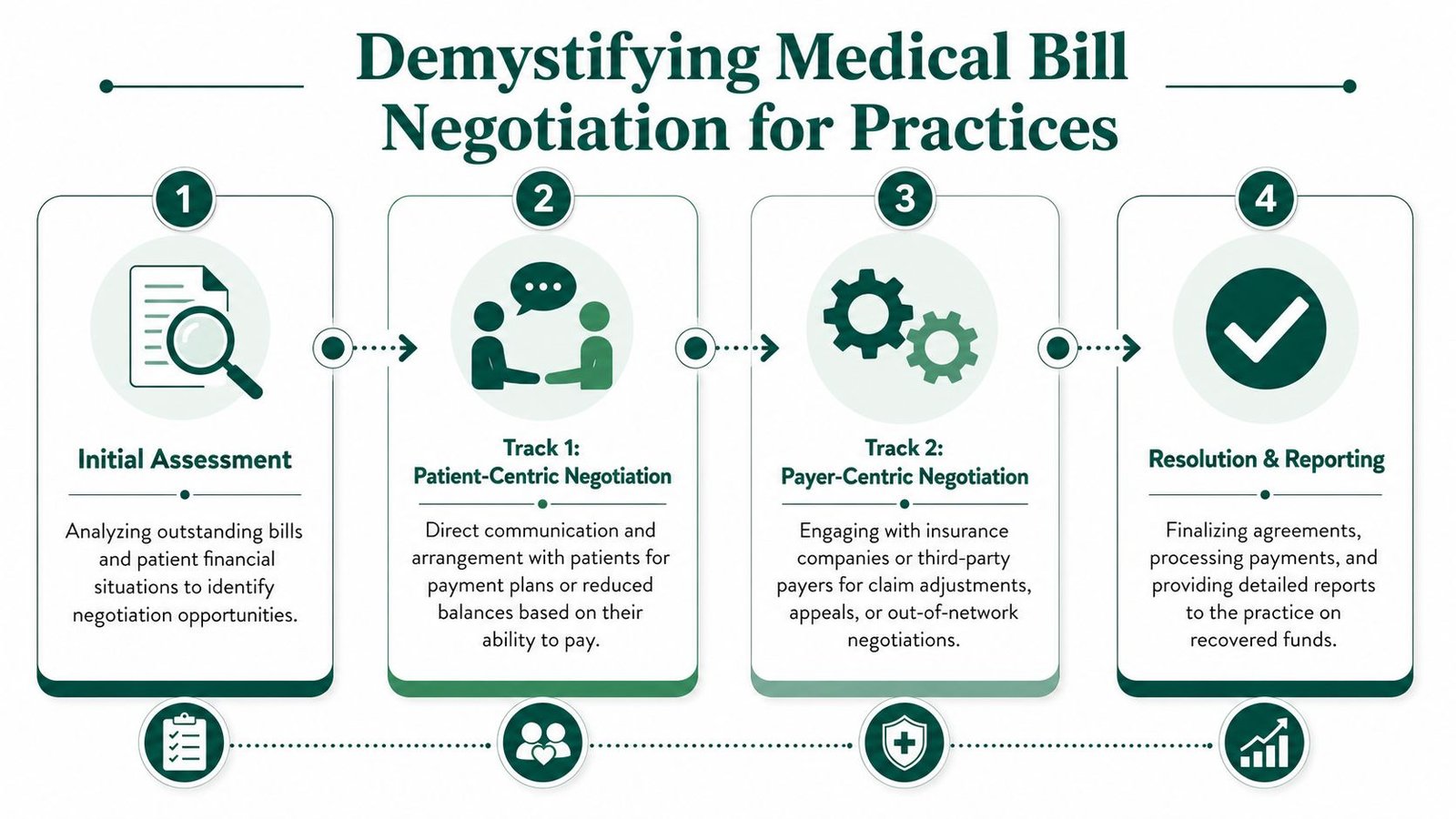
Track one for patient balances
On the patient side, negotiation usually starts with an account-level review. The negotiator checks whether the balance is collectible as billed. That can include matching the patient statement to the EOB, verifying whether the deductible and coinsurance were applied correctly, and reviewing whether the account reflects an itemized and internally consistent charge set.
Consumer-facing disclosures describe the core method clearly. Independent services often create savings by combining itemized-bill auditing, coding-error detection, and fair-market-rate benchmarking, then using those findings to seek repricing or discounts. Those disclosures report reductions of 25% to 50% in many cases (Altumed).
For a practice, the financial lesson is not “give discounts.” It is this: when the balance contains inconsistencies, inflated charge presentation, duplicate line items, or coding-level issues, the account becomes harder to defend at full value. A negotiation service uses that weakness to close the account instead of letting it age into bad debt.
Track two for payer disputes
Payer-side negotiation is more technical and usually more valuable for a physician group.
A service reviews remits, contract terms, appeal history, and denial patterns to determine whether the payer paid below contract, bundled incorrectly, or forced a write-off that should never have been taken. The point is not to ask for courtesy. The point is to enforce terms.
Common examples include:
- Modifier 25 disputes: A payer improperly bundles a significant, separately identifiable E/M service such as CPT 99214 with a minor procedure. If documentation supports the modifier, every wrongly bundled encounter lowers revenue.
- Modifier 59 or NCCI-related issues: A payer applies edits too broadly and suppresses payment for a distinct procedural service.
- Professional component underpayment: Imaging or diagnostic interpretations billed with modifier 26 are paid incorrectly or denied due to payer logic rather than actual contract language.
- Global period leakage: In orthopedic or pain management settings, post-op services are denied or folded into the global package beyond what the payer policy or procedure rules support.
When a payer says “inclusive,” your next question should be “inclusive under which contract term, edit set, or policy language?”
That is where many internal teams get stuck. They know payment feels wrong, but they do not have the time to build a reusable dispute package claim by claim.
A specialized partner should also feed those patterns back into your denial workflow. If a payer repeatedly mishandles a modifier, your team should stop treating that as isolated noise and start treating it as a recoverable payment pattern. That's where a disciplined denial management service becomes complementary, not redundant.
What creates leverage
Negotiation succeeds when the other side has a reason to move. In practice, that advantage usually comes from one of four places:
A defensible error
Duplicate charges, wrong CPT-level assignment, unsupported patient balance transfer, or a remit that doesn't match contract logic.A contract mismatch
The payer's payment doesn't line up with fee schedule terms, modifier rules, or payment policy.A practical settlement path
The account is valid, but a structured payment or reduced settlement produces more cash now than prolonged nonpayment.Escalation discipline
The account is documented well enough to survive supervisor review, appeal review, or contract escalation.
Practices lose money when they confuse these categories. Each one needs a different playbook.
Strategic Use Cases for Your Medical Practice
The best use of negotiation services is selective. Not every balance deserves outside intervention. The right accounts are the ones where delay, complexity, or payer resistance has already made your internal cost of follow-up too high.
Underpayment and denial recovery
The highest-value use case is often payer underpayment, especially in specialties where modifiers, diagnostic components, or multiple-procedure logic affect reimbursement. A cardiology group, for example, may notice repeated issues around CPT 93306, or around claims where the professional and technical components are being handled inconsistently. The issue is rarely one claim. It is usually a payment behavior.
That's where negotiation beats routine posting review. A specialist can group affected claims, tie the variance back to contract logic, and reopen the conversation with a payer in a way that your day-to-day billing staff may not have the bandwidth to sustain.
Aged A/R that your team has already exhausted
There is a specific kind of aged A/R that still holds value. It is not the dead account. It is the account that stalled because ownership got fuzzy. Nobody knew whether it needed appeal, adjustment, rebilling, documentation support, or a patient-payment reset.
That segment is where negotiation services can outperform both front-desk collections and generic follow-up vendors.
A useful operational reference is this 2026 accounts receivable guide, especially if you're deciding which aging buckets should stay in-house and which ones need outside recovery muscle. The key is segmentation. You should not outsource all old balances. You should isolate the ones where specialist intervention has a realistic path to recovery.
Self-pay and high-deductible balances
Here, many practices either get too aggressive or too passive.
If your staff presses full balance collection on every high-deductible account without checking the underlying bill quality, you create friction and collect less. If they back off too quickly, the account drifts.
Hospital-bill negotiation advice often misses a critical point. The primary constraint is frequently the payer-side math. Hospitals and providers may already be limited by charity-care rules, prompt-pay structures, or insurer-specific allowed amounts, which means negotiation is only one option in a broader decision tree (PeopleKeep).
For practices, the lesson is simple. Some balances should be negotiated. Others should be disputed. Others should be corrected before anyone discusses payment.
The wrong question is “Can we negotiate this account?” The right question is “What is the fastest defensible path to cash on this account?”
Three signals that an account belongs in a negotiation queue
| Scenario | What it usually means for the practice | Better response |
|---|---|---|
| Repeated payer variance on the same code or modifier | Systemic revenue leakage | Contract-based negotiation and escalation |
| Patient balances with objections tied to bill detail | Collectability problem caused by bill credibility | Audit first, then structured resolution |
| Old balances with multiple touches and no next step | Internal workflow exhaustion | Assign to a specialized recovery track |
That framework is what keeps negotiation from becoming random account chasing.
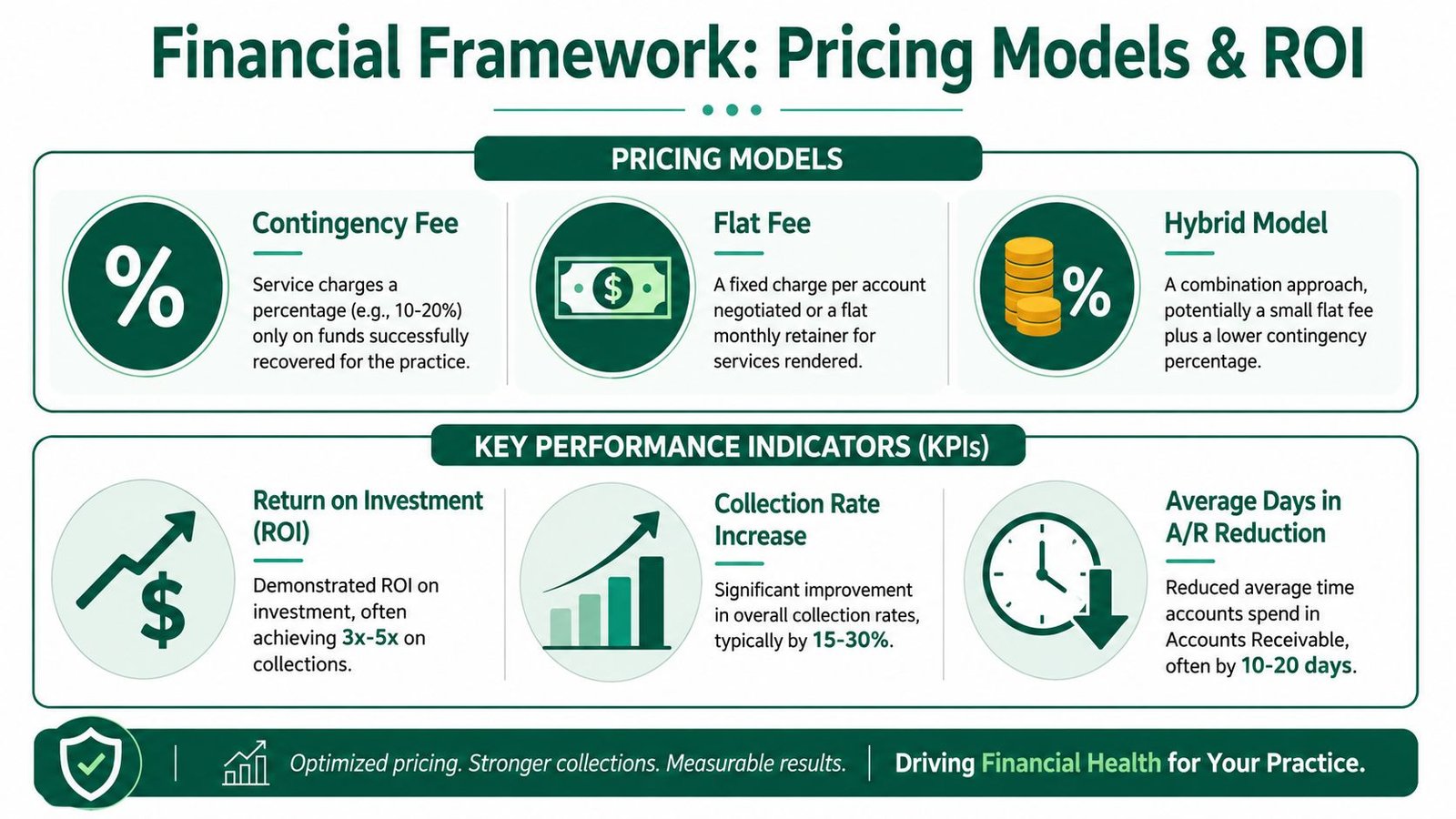
Pricing Models ROI and Key Performance Indicators
If you're evaluating medical bill negotiation services, the pricing model matters almost as much as the recovery skill. A poor fee structure can produce busy reports and weak net value.
Why contingency pricing gets attention
The most practice-friendly structure is usually a contingency model tied to actual savings or recovery. That works because it aligns the vendor's incentives with the account outcome.
One public example uses a fee of 25% of savings, capped at $1,000, with no upfront fee and no charge if there is no reduction. In the example provided, a $3,500 bill reduced to $2,500 produces a $250 fee (CareRoute Bill Defense).
For a practice owner, the takeaway is operational. When the fee is contingent, the service has to identify a real financial opportunity before it gets paid. That lowers adoption friction and helps you test difficult account classes without committing fixed overhead first.
The pricing structures you'll actually see
You'll typically encounter three models:
Contingency fee
Best for aged A/R, underpayment recovery, and disputed balances where outcome is uncertain.Flat fee per account or monthly retainer
Better when volume is predictable and the scope is narrow, such as structured self-pay balance review.Hybrid arrangement
Useful when the partner is doing both recovery and root-cause analysis that feeds back into front-end billing operations.
The wrong model for most independent practices is a vague “consulting” agreement with no clear tie to recoveries, account categories, or reporting standards.
The KPIs that matter
If you outsource negotiation and only track recovered dollars, you're missing the wider impact. The better scorecard includes:
Net recovery by account class
Separate payer underpayments, patient balances, and aged A/R recovery. These categories perform differently.Days in A/R
A good negotiation process should help reduce old unresolved balances, rather than reshuffling them between work queues.Write-off reversal quality
Watch whether recovered accounts came from premature contractual adjustments, avoidable bad debt classification, or denied claims that should have remained active.Denial feedback loop
If the service keeps recovering the same modifier-related issue, your internal claim edits need to change.
Owner's test: If the vendor cannot show you which account types moved, why they moved, and what your team should fix upstream, the service is recovering cash but not improving the revenue cycle.
To benchmark that performance internally, keep your negotiation work tied to the broader set of medical billing KPIs to track. Otherwise, recoveries can look strong while denial prevention stays weak.
How to Evaluate and Choose a Negotiation Partner
A negotiation partner should understand your specialty, your payer mix, and the exact points where money leaks out of your workflow. If they cannot talk credibly about your procedure patterns and modifier exposure, they are not a fit.

Specialty knowledge is not optional
An anesthesiology group needs a partner who understands time units, base units, concurrency, and payer handling of anesthesia modifiers. A behavioral health group needs someone who understands authorization failure patterns and coverage limits. An orthopedic practice needs fluency in global periods, post-op billing boundaries, and modifier use around procedures and E/M services.
If a vendor says they handle every specialty exactly the same way, that's a warning sign. They probably recover only the easiest accounts.
For orthopedic groups especially, knowledge of global package rules directly affects what gets appealed, adjusted, or defended. If that's your area, review a specialty-specific workflow like this one for orthopedic billing support before choosing a generalist.
Questions that reveal real capability
Use the sales conversation to force specificity. Ask things like:
- Which denial categories do you recover most often for practices like mine
- How do you handle CPT 99214 with modifier 25 when a payer bundles it into a same-day procedure
- What is your process for identifying professional component underpayments on modifier 26 claims
- How do you report payer-specific trends versus one-off account fixes
- What access do you require in the EHR or PM system, and can you work read-only
A serious vendor will answer in operational terms. A weak one will default to generic promises about “maximizing reimbursements.”
Red flags worth taking seriously
| Red flag | Why it matters |
|---|---|
| Ambiguous fee language | You won't know what counts as recovery or savings |
| No specialty examples | They may not understand your highest-risk revenue scenarios |
| Reporting limited to total dollars | You cannot measure process quality or root causes |
| No clear HIPAA and access controls | The revenue upside is not worth compliance exposure |
| One-size-fits-all workflow | Complex payer behavior will slip through the cracks |
Before hiring anyone, it's smart to pressure-test your own internal blind spots first. A structured checklist like these questions to ask a medical billing company before hiring helps you separate actual negotiation capability from polished sales language.
Implementation Steps and a Case Example
The cleanest implementations are narrow at the start. Don't hand over your full A/R universe on day one. Start with a defined account set and clear rules.

A practical rollout sequence
Segment the A/R
Pull accounts by payer, age, balance type, denial reason, and specialty-specific coding exposure. Separate underpayments from patient balances and both from true bad debt.Set access rules
Give the vendor only the system access required to review and work accounts. Read-only access is often enough for the review phase. Internal permissioning matters as much as the BAAs you sign.Define settlement authority
Decide which patient balances can be adjusted, which payer disputes require your approval, and which accounts should never be settled without provider review.Build a reporting cadence
Weekly or biweekly reporting works best at launch. You want visibility into account movement, root causes, and any payer pattern emerging early.
A lot of practices overlook the compliance side of onboarding. Staff who interact with outside vendors should understand the same privacy and handling rules applied internally. This overview of HIPAA training requirements is a useful refresher when you tighten vendor workflows.
What a realistic case example looks like
A credible case example does not need dramatic storytelling. It needs a recognizable operational problem.
Take an independent cardiology group that keeps seeing imaging-related claims paid inconsistently when the professional component is billed with modifier 26. Internal staff appeal some claims individually, but the pattern never fully surfaces because each remit gets treated as a separate event. A negotiation-focused review groups those claims by payer, identifies where adjudication logic diverges from contract expectation, and pushes a consolidated recovery effort instead of isolated rebills.
That kind of work succeeds because it turns anecdotal frustration into a documented payment pattern.
If you want to see what that style of recovery process looks like in a more structured format, review this revenue recovery case study blueprint. The useful lesson is not the specialty alone. It is the method: segment, document, escalate, and feed the findings back into front-end claim quality.
Frequently Asked Questions for Practice Owners
Are medical bill negotiation services just another collections agency
No. Collections agencies usually work after the account has already shifted into a debt-collection posture. Medical bill negotiation services work closer to the revenue cycle itself. They review whether a balance can be corrected, defended, repriced, appealed, or resolved before it becomes pure collections inventory.
That distinction matters for both recovery and reputation. Practices that send every difficult account straight to collections usually collect less and create more friction.
Will a negotiation service replace my in-house billing team
It shouldn't. The right partner handles the accounts your team doesn't have time, bargaining power, or technical specialization to pursue efficiently.
Your internal team should still own clean claim submission, payment posting, patient communication standards, and front-end issue prevention. The negotiation layer is most useful for payer disputes, stubborn underpayments, aged A/R pockets, and high-friction balances where routine follow-up has stalled.
Can a service really negotiate with payers on claims that were already paid
Yes, if the claim was paid incorrectly and there is still a valid reopening, appeal, or contractual challenge path. This is common when a payer applies bundling logic too aggressively, mishandles a modifier, or pays a service below the contracted expectation.
The key is evidence. A paid claim is not automatically a correct claim. But a recovery effort only works if the vendor can tie the variance to contract language, documentation, modifier support, or adjudication inconsistency.
When should I negotiate a balance instead of dispute it
Negotiate when the balance is valid but difficult to collect at full value. Dispute when the balance may be wrong.
That sounds obvious, but practices blur the line constantly. If the account reflects a coding issue, an EOB mismatch, a payer processing error, or a contractual payment problem, negotiation is premature. If the balance is accurate and the challenge is collectability, settlement structure becomes more useful.
If your practice has old balances, recurring underpayments, or payer behavior that your current team can't keep up with, Happy Billing can help you identify where negotiation belongs and where a deeper RCM fix will produce more cash. A practical starting point is to request a free billing audit so you can see which accounts are recoverable, which denials are preventable, and which write-offs should never have happened.