Denial Management Services: Boost Your Revenue

If your practice is losing even one in ten claims, you're already giving away revenue, and 41% of providers say that's exactly where they are. Denial management services matter because the cost to rework each denied claim climbed from $43.84 in 2022 to $57.23 in 2023, which means every preventable denial now hits your cash flow twice: once in delayed payment and again in staff labor.
We've seen this pattern in independent practices over and over. A/R stretches out, front-desk errors keep resurfacing, authorizations slip, coding misses pile up, and the owner ends up funding payer friction with physician margin. Good denial management services fix that by acting as a proactive system for preventing, identifying, and resolving claim rejections, not just a team that files appeals after the damage is done.
For a practice owner, that distinction matters. Reactive denial work feels busy. Preventive denial management protects revenue.
What Are Denial Management Services
Denial management services are the operational and analytical systems that stop claims from failing, sort denied claims by recoverability, correct root causes, and push the lessons back into scheduling, registration, eligibility, authorization, documentation, coding, and payer follow-up.

A lot of owners hear "denial management" and think "appeals team." That's too narrow. If your current vendor only touches the claim after the ERA posts a denial, they are solving the most expensive version of the problem.
According to Experian's 2025 State of Claims report, 41% of providers state that at least one in ten of their claims are denied, and the administrative cost to rework a single denied claim rose from $43.84 in 2022 to $57.23 in 2023. That should end the debate about whether denials are a billing nuisance or a financial threat. They're a margin problem.
What practice owners should hear in that data
When denials climb, your business feels it in several places at once:
- Cash slows down: Payments that should have funded payroll, supplies, and growth get pushed into follow-up queues.
- Staff gets buried: Your team spends time touching old claims instead of getting new claims out cleanly.
- Write-offs increase: Some denials age out, some miss filing windows, and some never get the attention they should.
- A/R gets distorted: Old balances make your reports look collectible when they really aren't.
Practical rule: If your denial workflow starts after remittance, you're already late.
What good services actually include
Strong denial management services usually combine these functions:
- Front-end controls: Eligibility verification, demographic checks, payer selection review, and authorization tracking.
- Claim quality review: Scrubbing for coding conflicts, modifier misuse, missing documentation, and payer-specific edit failures.
- Denial analytics: Sorting by payer, reason code, location, rendering provider, service line, and denial stage.
- Recovery workflow: Correcting claims, filing appeals, monitoring deadlines, and escalating high-value accounts.
- Root-cause feedback: Fixing the workflow that caused the denial so it doesn't repeat next week.
That last part is the difference between a billing department that stays underwater and one that gets control back. We've seen practices cut frustration fastest when they stop treating denials as isolated events and start treating them as process defects with owners, deadlines, and accountability.
Beyond Appeals The Full Denial Management Workflow
A serious denial management program is a closed-loop system. It prevents what it can, triages what still fails, and feeds every denial lesson back into the front end so the same claim doesn't break the same way again.
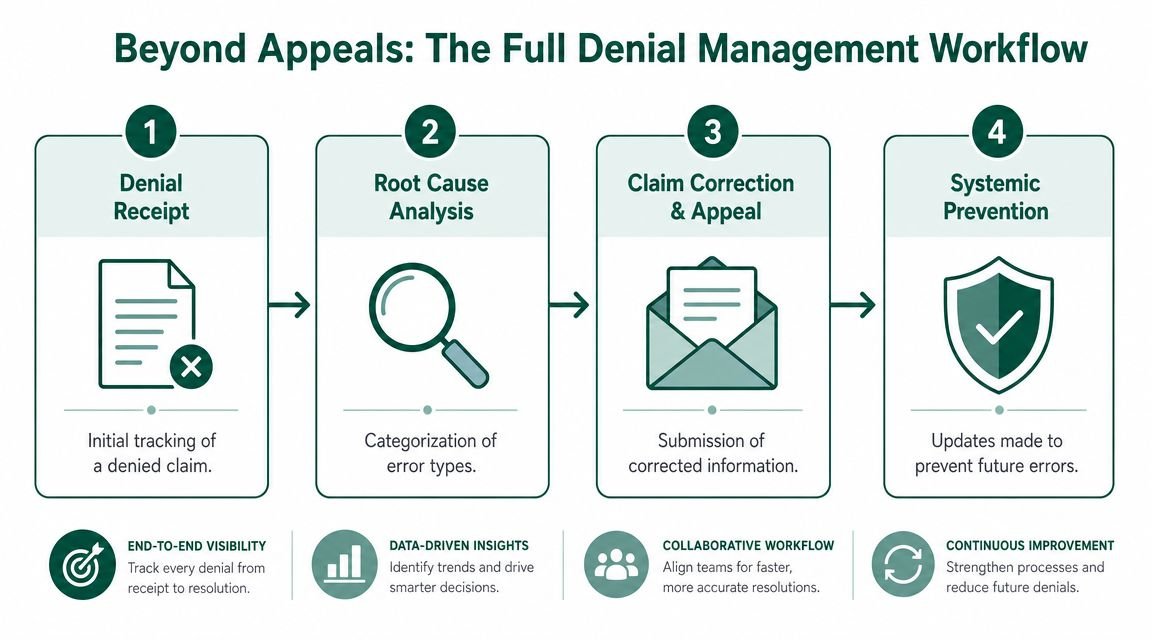
The economics are straightforward. The administrative cost to rework a single denied claim is estimated at $25 to $40 in this overview of denial management economics. That's why prevention beats heroics. You want fewer claims entering rework in the first place.
Pre-bill prevention
The highest-value denial work happens before the claim goes out.
That means confirming eligibility, checking whether the patient is active on the date of service, verifying whether prior authorization is required, and making sure the rendering provider, place of service, and payer routing are all correct. In practices with heavy documentation demands, we've also seen better results when physicians standardize templates and dictation workflows. If you're cleaning up documentation gaps tied to medical necessity or incomplete notes, this guide on choosing healthcare voice recognition software is worth reviewing because better documentation capture often reduces downstream claim friction.
For procedure-heavy specialties, this stage also includes reviewing modifiers, bundled services, global periods, and payer edits before submission. Owners don't need every coding detail. They do need to know whether their current workflow catches obvious revenue killers before they become denials.
Intelligent claim scrubbing
Claim scrubbing should do more than flag missing fields.
The best workflows run claims through payer-specific edits and specialty-specific rules before transmission. That includes checking diagnosis-to-procedure alignment, modifier logic, authorization references, documentation attachments, and common edits tied to recurring CARCs and RARCs.
We've seen ordinary scrubbers miss issues because they apply generic rules to specialty-heavy claims. A denial management service should know the difference between a general billing edit and a specialty workflow defect.
Prioritized triage, not random work queues
Once a denial lands, the claim shouldn't just be dumped into a shared spreadsheet.
Use a triage model that sorts claims by:
- Dollar value
- Timely filing risk
- Probability of overturn
- Payer behavior
- Missing documentation burden
A $ high-value denial with a short filing window deserves immediate attention. A low-value denial with weak appeal odds may not. Owners should expect the partner to make those calls rationally, not emotionally.
For the actual resubmission and appeal mechanics, this walkthrough on how to appeal a denied insurance claim gives a solid overview of what disciplined follow-up should look like.
The real win isn't filing more appeals. It's building a system that sends fewer bad claims and works the right denied claims first.
Strategic appeals and feedback loops
Appeals still matter. They just shouldn't be the main event.
A mature workflow documents the denial reason, fixes the claim, supports the appeal with payer-appropriate records, tracks the response deadline, and then updates the front-end process so the issue doesn't recur. If a payer keeps denying for authorization, the answer isn't "appeal faster." It's to fix authorization capture. If denials cluster around documentation, the answer is better physician workflow, not more collector labor.
That's what owners should buy. Not just denial rework. A revenue-protection system.
Common Denials By Specialty and Their Financial Impact
Generic denial management services usually underperform because they flatten every specialty into the same workflow. That's a mistake. This specialty-focused denial management guidance makes the point clearly: the most preventable denials in anesthesiology, mental health, and orthopedics require different upstream controls.
If your vendor can't explain specialty-specific denial patterns in plain English, they're not managing revenue. They're processing tasks.
The denials that hit different specialties differently
Here is the version practice owners need to see:
| Specialty | Common Denial Reason | Example Code/Modifier | Financial Impact |
|---|---|---|---|
| Orthopedics | Global period conflicts and modifier misuse | Modifier 59, modifier 25 | Post-op visits or related services may be denied or bundled, forcing rework and delaying payment on high-value surgical episodes |
| Cardiology | Bundling and documentation mismatches on imaging | CPT 93306 | Echocardiography claims can be delayed or denied when documentation, diagnosis support, or payer edit logic doesn't line up |
| Anesthesiology | Concurrency and time-unit disputes | Anesthesia time reporting, concurrency rules | Incorrect concurrency handling can reduce payable units or trigger denials that directly cut case revenue |
| Behavioral health | Missing or invalid authorization | CPT 90837 | Sessions may be denied outright when authorization requirements aren't met or aren't documented properly |
That table is exactly why broad, one-size-fits-all billing support fails. The root cause isn't "claims." The root cause is how each specialty generates claims.
Orthopedics and post-op leakage
Orthopedic practices lose money when the billing team doesn't respect global periods and modifier logic. Modifier 25 on a significant, separately identifiable E/M service and modifier 59 on distinct procedural services can be valid, but they need clean documentation and payer-aware logic. If your team applies them loosely, payers deny. If your team avoids them out of fear, you underbill.
We've seen orthopedic groups get stuck in both errors at once. They fight avoidable denials on one side and leave legitimate revenue unclaimed on the other.
Cardiology and imaging edits
Cardiology gets hit by payer scrutiny because imaging, testing, and interventional services carry frequent bundling and medical-necessity review. A code like 93306 looks straightforward until diagnosis support, ordering documentation, NCCI logic, and payer-specific edits collide.
If you run a cardiology group, your denial strategy should look very different from a primary care workflow. This breakdown of cardiology billing denials is useful if you're trying to identify which denial categories are draining revenue in cardiac imaging and testing.
Owners shouldn't ask, "Do you handle denials?" They should ask, "Which denial categories are most preventable in my specialty, and what workflow changes stop them?"
Anesthesiology and behavioral health need different controls
Anesthesiology denials often hinge on time reporting, base unit support, modifier accuracy, and concurrency. Behavioral health has a different problem set. Authorizations, visit limits, and payer-specific utilization rules often drive denials more than raw coding mechanics.
That means your controls should be specific:
- For anesthesiology: Review concurrency logic, time capture, and modifier accuracy before claim submission.
- For behavioral health: Build airtight authorization intake, renewal tracking, and documentation checks around services like 90837.
- For orthopedics: Audit global period edits and modifier use before the payer does.
- For cardiology: Pair imaging documentation with payer edit review before the claim leaves the system.
If your specialty faces recurring denials, look beyond generic billing advice. Start with a specialty-focused revenue cycle review through the medical billing specialties page and evaluate whether the workflow matches your claim complexity.
KPIs That Prove Denial Management ROI
If a denial management partner can't show you results in metrics that affect cash, don't hire them.
Owners should track initial denial rate and final denial rate separately. HFMA's denial metric guidance recommends monitoring initial denial rate, primary denial rate, denial write-offs as a share of net patient service revenue, time from initial denial to appeal, time from initial denial to claim resolution, and the percentage of initial denials overturned. That's the right framework because it separates front-end failure from back-end recovery.
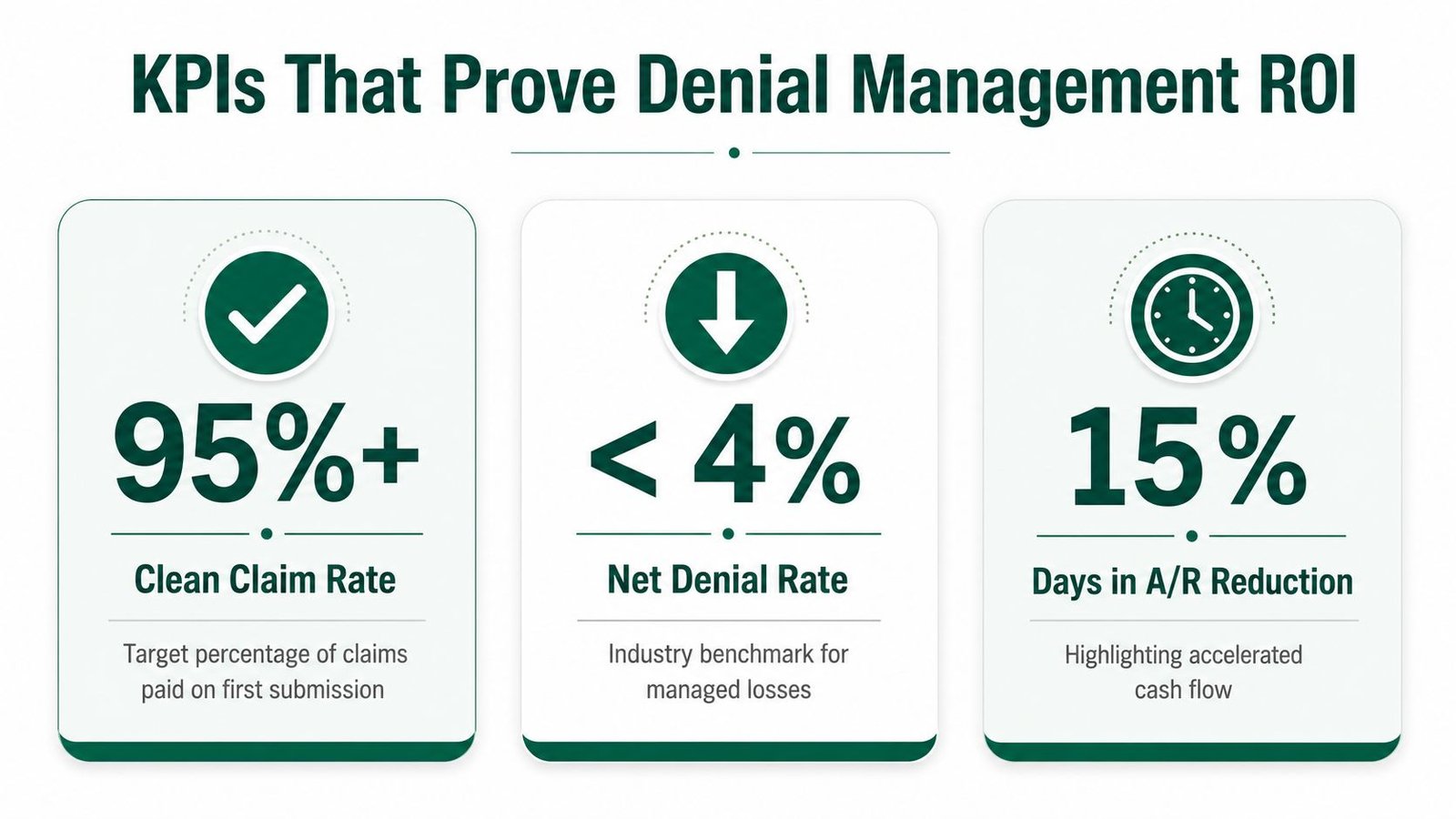
The KPI set that actually matters
A healthy operation should target a clean claims rate over 95%, a denial rate under 5%, and days in A/R under 40 according to FinThrive's denial management benchmarks. Those aren't vanity metrics. They tell you whether your front end is stable and whether cash is moving.
Use this lens:
- Initial denial rate: Shows how many claims fail on first submission. If this is high, your registration, eligibility, authorization, coding, or documentation process is breaking upstream.
- Final denial rate: Shows what remains unrecovered after appeals and corrections. Real revenue leakage becomes permanent at this stage.
- Clean claim rate: Measures whether claims go out correctly the first time. A low number usually points to systemic front-end defects.
- Days in A/R: Tells you how long cash is trapped. The longer claims sit, the more effort they take and the less likely full recovery becomes.
- Appeal success rate: Reveals whether your team is choosing the right denials to work and supporting them properly.
How to read the dashboard like an owner
Don't let a vendor hide behind one good number.
A practice can have a respectable final denial rate because staff is doing heroic cleanup while still having an unhealthy initial denial rate. That means you're funding inefficiency with labor. We've seen owners miss this because they only reviewed collections, not the steps it took to get there.
A strong dashboard should segment by payer, denial reason, service line, location, and denial stage. If you want a useful framework for reporting and accountability, this guide to medical billing KPIs to track is a good benchmark.
Owner test: Ask your billing partner which metric tells them your front desk is causing denials and which metric tells them their appeals team is failing. If they can't answer cleanly, their reporting isn't mature.
For practices trying to reduce overhead while improving speed, this resource on how to lower healthcare processing costs is also useful because denial reduction and admin-cost reduction are tightly connected.
Your Vendor Selection Checklist
The denial management market is getting bigger because practices are tired of carrying denial waste internally. A market report projects the U.S. Healthcare Denial Management Market will reach $8.93 billion by 2030, and it identifies integrated systems as the fastest-growing segment in this market projection. That matters for one reason. You should favor partners that work inside your existing EHR and PM stack instead of forcing a disruptive migration.
What to demand before you sign
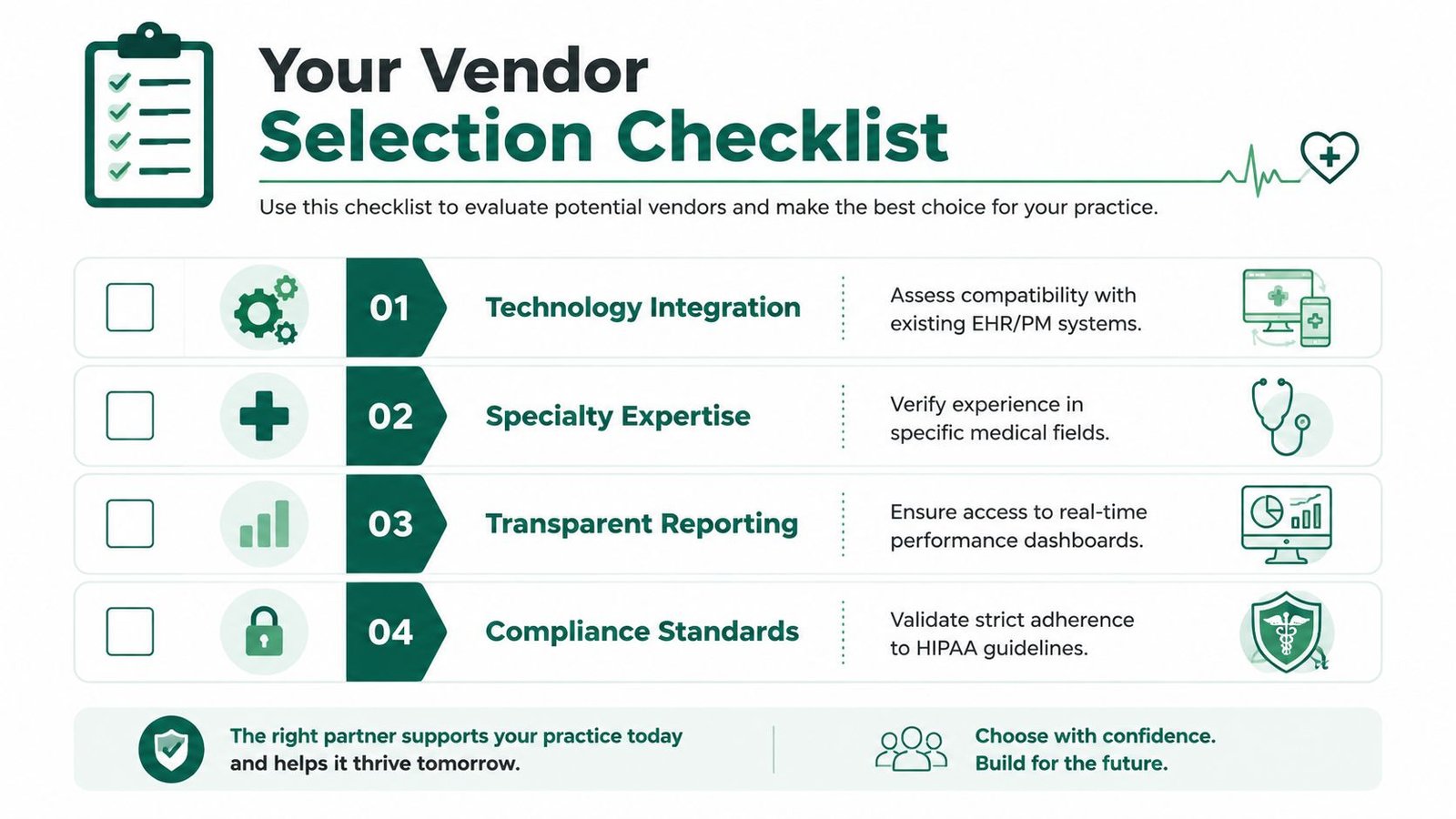
Use this checklist and be blunt.
- Specialty fit: Ask which specialties they handle best and which denial categories they prevent well. If you're in anesthesiology, ask about concurrency. If you're in behavioral health, ask about authorization controls. If you're in orthopedics, ask about global periods and modifier handling.
- System integration: Ask whether they can operate inside your current EHR, billing, and practice management tools. Migrations create risk, slowdowns, and staff resistance.
- Reporting clarity: Require dashboards that show denials by payer, reason, provider, location, service line, age, and recoverability.
- Appeal discipline: Ask how they prioritize denied claims and what documentation package they expect for each appeal category.
- SLA ownership: Require defined turnaround times for denial posting, claim correction, appeal submission, and follow-up.
Questions owners should ask in the meeting
These questions expose weak vendors fast:
- Which denials do you prevent before claim submission?
- How do you separate initial denials from final denials?
- What specialty rules do you apply for my practice type?
- How do you handle payer-specific edits and authorization failures?
- What can my physicians or front desk change immediately based on your findings?
If the answers are vague, move on.
Security and compliance still matter
Revenue improvement doesn't excuse sloppy compliance. The vendor will touch PHI, payer correspondence, and financial workflows. Review their HIPAA posture, access controls, audit discipline, and incident response process. If you want a practical outside reference, this article on healthcare IT compliance for SMBs is a useful checklist for small and midsize practices evaluating operational risk.
For a side-by-side framework on what a strong partner should look like overall, review this guide on the best medical billing company.
The wrong vendor gives you more reports. The right vendor gives you fewer denials, faster cash, and less physician distraction.
If you're evaluating options right now, the smartest next step is a free billing audit focused on denial root causes, not just claim volume.
What to Expect During Implementation
Most owners worry that changing denial management workflows will disrupt billing. It doesn't have to, if the transition is controlled and someone owns it.
In the first month, the partner should get system access, review payer mix, map your denial categories, inspect aged A/R, and identify where front-end failures are entering the claim stream. We've seen the smoothest transitions when the practice appoints one internal decision-maker who can resolve questions quickly.
A practical 30 60 90 view
- First 30 days: Access, workflow mapping, denial categorization, payer trend review, and the first round of corrective actions.
- By 60 days: Front-end fixes start to stabilize claim quality, denial work queues get cleaner, and appeal handling becomes more disciplined.
- By 90 days: You should have a much clearer picture of whether the partner is improving A/R velocity, reducing preventable denials, and cleaning up old inventory.
This isn't magic. It's operational discipline.
What helps implementation succeed
A short list makes the difference:
- Single owner inside the practice: One point of contact prevents delays and mixed instructions.
- Weekly review cadence: Denials move fast. Your oversight should too.
- Provider cooperation: If documentation is part of the denial pattern, physicians need short, specific feedback.
- Clear escalation rules: High-value claims and payer deadline risks need immediate attention.
If you're comparing whether to build this internally or hand it to a partner, this guide on outsourcing medical billing is a good place to pressure-test the decision.
Your Denial Management Questions Answered
Should I outsource denial management or fix it in-house
Outsource it if denials are recurring across multiple workflow points and your internal team is stuck in rework mode. Keep it in-house if you already have specialty expertise, strong reporting, disciplined front-end controls, and leadership capacity to manage constant payer changes. Most independent practices don't have all four.
How do I know whether a denial management service is actually preventing denials
Ask what changed upstream. If the vendor only talks about appeals filed, they are describing labor, not prevention. A real partner should point to workflow changes in eligibility, authorization, documentation, coding edits, or payer routing.
Will outsourcing make me lose control of billing
Not if it's structured correctly. You should gain visibility, not lose it. The right setup gives you cleaner dashboards, faster escalation, and clearer accountability than most in-house denial workflows.
Which practices benefit most from denial management services
The biggest upside usually sits in specialties with complex payer rules, frequent authorizations, procedure-heavy billing, or modifier-sensitive claims. Anesthesiology, behavioral health, cardiology, and orthopedics are common examples because denial patterns there are rarely generic.
If you're tired of watching denials inflate A/R and distract your physicians, Happy Billing can help you find the actual leak points. Their team works inside your current systems, builds specialty-specific workflows, and gives practice owners a practical path to fewer denials, faster collections, and less rework.