Accurate Wound Care Documentation Template for 2026
A detailed wound care documentation template is a structured form that captures the details payers and auditors expect, and its real job is to create an audit-ready record that supports medical necessity and payment. That matters because incomplete wound charting is common: 12% of wounds had no recorded diagnosis and 56% of leg ulcers lacked a differential diagnosis, which is exactly the kind of omission that slows payment and weakens appeals.
If you own a practice, this isn't a note-writing problem. It's a revenue leakage problem. Wound care claims rise or fall on whether the chart shows what was treated, why it was medically necessary, how the wound changed, and what response followed. When those details live in scattered free text, one clinician's shorthand turns into your denial, your rework, and your aging A/R. A disciplined wound care documentation template turns that around by making the billable story visible inside the chart the first time.
Why Your Wound Care Notes Are Hurting Your Revenue
Most practices don't lose wound revenue because the clinician didn't treat the wound correctly. They lose it because the record doesn't defend the service after the patient leaves.
A weak wound note usually looks harmless. It mentions the location, says "improved" or "debrided," and moves on. From an RCM standpoint, that's where trouble starts. Payers don't reimburse narratives. They reimburse defensible, specific, time-appropriate documentation that supports the claim line by line.
What public templates usually miss
Most public templates explain the clinical fields to capture, such as location, dimensions, and tissue type, but they rarely address the harder question of how to make the note defensible for reimbursement. That gap matters because wound documentation is often fragmented across team members, and UK guidance warns that blank fields can be interpreted as omissions of care, as discussed in this review of wound documentation gaps and reimbursement risk.
The business impact is straightforward:
- Blank fields create appeal problems. If the chart doesn't show why treatment continued or changed, your staff has to reconstruct the visit later.
- Free text invites inconsistency. One provider documents drainage in detail. Another writes "stable." The payer sees uneven support for similar claims.
- Delayed charting weakens the record. The longer the gap between care and documentation, the harder it is to defend the exact service performed.
Practical rule: If a clinician's note can't stand alone in an audit packet, the claim was never truly clean.
Why owners should care now
Wound care often includes repeat visits, ongoing reassessment, and procedures that attract scrutiny. That combination makes documentation quality a direct predictor of cash velocity. When your template forces consistency, your team submits cleaner claims, appeals fewer denials, and spends less time chasing records.
We've seen practices focus heavily on coding edits while ignoring the note template that feeds those edits. That's backwards. Coding can only work with what the chart gives it. If your current workflow still depends on memory, copied-forward wording, or optional fields, start there. A practical place to benchmark the issue is your denial workflow. This guide on how to reduce claim denials aligns closely with what we see in wound-heavy practices: the denial often starts upstream in documentation, not at claim submission.
The Anatomy of an Audit-Proof Wound Care Template
An effective wound care documentation template isn't a generic intake form. It's a repeatable dataset collected at every visit so the chart shows medical necessity, treatment logic, and progress over time.
One of the clearest standards in clinical guidance is that the template should capture etiology, location, dimensions, tissue composition, exudate, wound-edge status, periwound condition, pain score, infection signs, and interventions. That matters because omission risk is real. A review highlighted that 56% of leg ulcers lacked a differential diagnosis, which is a strong argument for structured documentation rather than open-ended narrative notes in this discussion of wound documentation compliance.
The fields that carry financial weight
Below is the core structure we recommend practices build into the wound care documentation template.
| Documentation Field | What to Record | Why It Matters for Billing |
|---|---|---|
| Etiology | Cause or differential diagnosis | Shows why the treatment plan fits the wound type and supports medical necessity |
| Exact location | Precise anatomical site | Prevents ambiguity when multiple wounds exist and helps match follow-up visits |
| Length, width, depth | Consistent measurements using the same method | Supports progress tracking and helps defend procedural intensity |
| Tissue composition | Granulation, slough, eschar | Helps justify what tissue required treatment and why a procedure was performed |
| Exudate | Amount and character | Supports clinical severity and need for ongoing management |
| Wound edge | Rolled, attached, undermined, irregular | Shows complexity and response to care |
| Periwound condition | Maceration, erythema, intact skin, edema | Demonstrates surrounding tissue impact and risk profile |
| Pain score | Standardized pain assessment | Supports the encounter's complexity and treatment tolerance |
| Infection signs | Odor, warmth, redness, systemic concerns | Helps justify escalation, monitoring, or change in plan |
| Interventions | Dressings, debridement details, offloading, cleansing, education | Connects the assessment to the actual billable service and response |
Standardization beats narrative skill
Narrative talent doesn't protect revenue. Standardization does.
A good template forces the same order every time. Etiology before intervention. Measurements before impression. Response after treatment. That sequencing matters because auditors and payers review whether the service was supported before it was billed. If the note reads like the treatment happened first and the rationale got added later, the claim becomes harder to defend.
A wound note should answer four questions without forcing the reviewer to infer anything: what wound, what changed, what was done, and why that service was necessary today.
What works inside the EHR
The most useful template is the one your clinicians will complete consistently in the live workflow. In practice, that usually means:
- Required fields for high-risk omissions. Etiology, measurements, tissue type, intervention, and response shouldn't be optional.
- Structured pick lists with room for nuance. Granulation/slough/eschar are easier to trend when standardized, but clinicians still need a comment box for unusual findings.
- One wound tracked as one record. Separate wounds should not be blended into one paragraph if you want clean longitudinal comparison.
- Measurement conventions built into prompts. If your template doesn't remind staff how to document tunneling or undermining consistently, variation creeps in fast.
This is also where front-end capture and back-end billing need to meet. If the template fields can't be translated easily into the claim support packet, your billers are left interpreting prose instead of validating documentation. Practices that still rely on encounter sheets and disconnected notes often benefit from reviewing how a superbill fits into medical billing workflows, especially when wound services involve multiple moving parts.
A note on scoring tools
Structured wound documentation didn't evolve by accident. A major foundation of modern templates is objective scoring and repeatable measurement. Clinical guidance points to standardized approaches such as the Pressure Ulcer Scale for Healing, often called PUSH, which was designed for trend reporting over time instead of one-time narrative charting. That shift is why high-performing templates behave less like a blank note and more like a flowsheet.
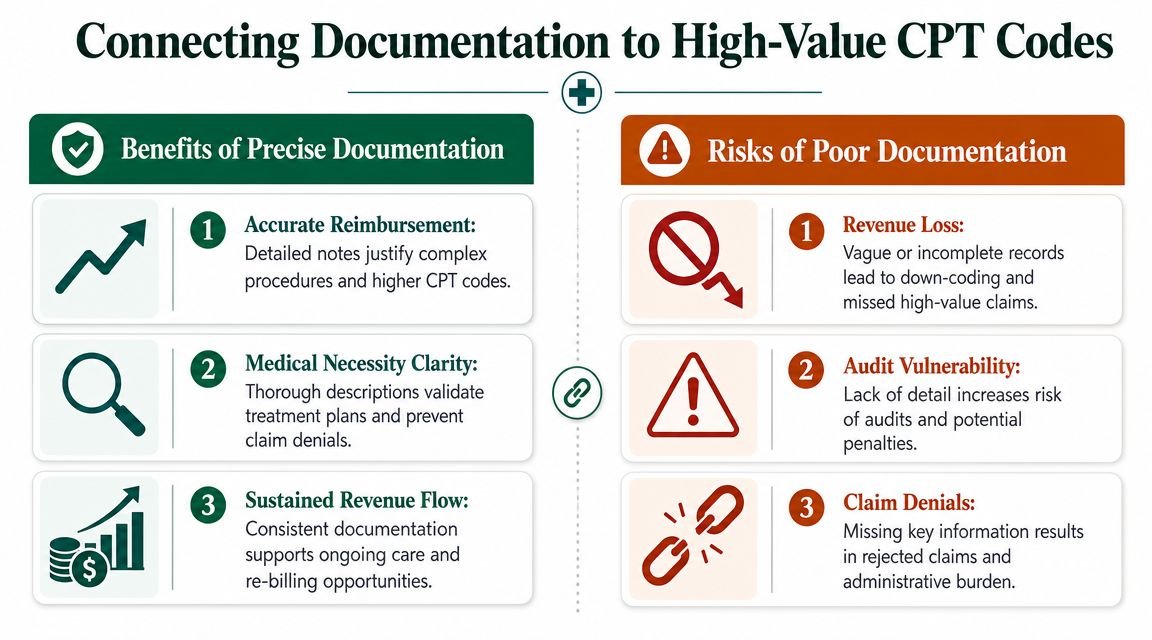
Connecting Documentation to High-Value CPT Codes
The fastest way to lose wound revenue is to assume coding can fix vague documentation after the fact. It can't. If the note doesn't establish tissue type, wound depth, wound size, treatment performed, and patient response, your team may be forced to downcode, hold the claim, or write off the denial when the record won't support an appeal.
Where documentation and coding meet
For wound encounters, owners should think in terms of supportable service categories, not just charge entry. Commonly reviewed services include E/M visits, debridement coding, and separate procedural reporting when payer rules allow. The exact code set, modifier use, and diagnosis linkage must be verified against current CMS guidance, CPT instructions, and payer policy before submission. That's especially important if your clinicians perform debridement and also bill a same-day E/M service.
Here's the practical issue. If the note says only "wound debrided, tolerated well," your billing team still doesn't know:
- what tissue was debrided
- how the wound was measured
- whether the service was selective or excisional
- whether the depth documented supports the procedure billed
- whether a separate E/M is distinct and defensible
Without that support, billing becomes guesswork. Guesswork leads to denials.
Modifiers and payer edits need documentation first
Many owners ask whether modifier usage can rescue a complicated wound claim. Sometimes it can prevent an edit from blocking payment, but only if the documentation already supports a distinct service. The common modifiers practices review in wound scenarios often include modifier 25 for a significant, separately identifiable E/M service and modifier 59 for distinct procedural circumstances. Those are not documentation shortcuts. They are claim signals that still require the chart to prove separation and necessity.
If your clinicians perform a procedure and also address broader management, the note should separate those components clearly. Distinct history, assessment, and medical decision-making for the E/M portion should not be buried inside the procedure paragraph. If they are, the procedure may get paid while the E/M is denied, or the entire claim may be flagged for review.
The modifier doesn't create reimbursement. The note earns it.
For practices that want a focused review of debridement billing logic, this resource on wound debridement CPT code requirements is a useful operational reference.
The owner-level takeaway
Don't ask only whether your team knows the right CPT code. Ask whether the wound care documentation template captures the details required to support whatever code your payer permits. If the answer is no, your clinicians are doing work your revenue cycle can't reliably monetize.
This is also where template discipline protects future appeals. A strong note gives your billing team the exact facts needed to defend the original claim without sending repeated chart queries back to the provider. That shortens rework time, protects filing deadlines, and keeps one weak note from becoming a multi-touch A/R problem.
Reducing Compliance Risk and Integrating with Your EHR
Audit-proof wound documentation depends as much on workflow as on clinical knowledge. If the template is hard to complete, buried in the EHR, or split across separate screens, clinicians will bypass it. Then your practice ends up with notes that are technically present but operationally weak.
Clinical guidance is clear that wound documentation should be completed in real time or immediately after the encounter and should include wound status, progress, and response to treatment. One Canadian flow-sheet example goes even further by requiring one wound per form, weekly measurements in centimeters, and wound-bed tissue documented in 10% increments, which shows how specific an audit-ready record can be in this review of wound documentation timing and structure.
What works in the EHR and what doesn't
The strongest setup is usually a dedicated wound flowsheet tied to the encounter note, not a loose dot phrase pasted into free text. Dot phrases are fast, but they fail when clinicians skip the hard fields or copy forward stale measurements.
A better build usually includes:
- One wound, one structured record. This avoids mixed findings when a patient has multiple wounds.
- Required measurement fields. Length, width, and depth should be entered before the note can be signed.
- Photo workflow standards. If your policy allows photos, keep the process consistent in angle, lighting, and use of a measurement guide.
- Treatment-plan reasoning. The chart should show why care changed, or why it didn't.
Operational fixes that reduce rework
Voice tools can help if they sit inside a structured workflow rather than replacing it. Practices exploring faster point-of-care charting should look at HIPAA-compliant voice recognition as a way to speed narrative capture while still requiring discrete wound fields in the EHR.
The implementation priority isn't speed alone. It's consistency. Your clinicians should be able to document the visit the same way whether they work in clinic, procedural space, or a mixed specialty setting.
If your EHR lets staff leave key wound fields blank, it isn't neutral. It's contributing to denials.
A practical next step is to map your documentation workflow to your revenue workflow. This overview of integrating revenue cycle management into practice operations is useful because the chart, charge, and appeal process should all pull from the same wound dataset rather than three different versions of the encounter.
Example Wound Care Notes That Prevent Denials
Most denial-prone wound notes don't fail because they're false. They fail because they're too thin to support the billed service.
Bad note example
Follow-up diabetic foot ulcer. Wound cleaned and debrided. Dressing applied. Continue current care.
This note creates obvious problems. It doesn't identify precise dimensions, tissue findings, depth, periwound condition, infection signs, or patient response. It also doesn't separate the assessment from the procedure, so a same-day E/M review becomes much harder to defend.
Better note example
Follow-up for diabetic foot ulcer at plantar forefoot. Etiology reviewed and unchanged from prior assessment. Wound measured using the same technique as prior visits. Length, width, and depth recorded in the wound flowsheet. Wound bed documented by tissue composition, with slough and granulation entered in structured fields. Periwound skin assessed and recorded. Drainage amount and character documented. Pain score recorded before treatment.
Selective debridement performed as documented in the procedure section. Tissue removed described in the note, and post-treatment wound status entered. Patient tolerated procedure. Response to treatment documented, and plan for next visit entered with reason for continuing current management.
That note is not longer for the sake of being longer. It's stronger because it gives the billing team support for the claim and gives the practice a better appeal file if the payer requests records.
Why this difference matters financially
The first note forces your staff to guess what happened or chase the provider later. The second note turns the encounter into a defensible claim package. That means fewer holds, cleaner review, and less back-and-forth between the clinic and billing team.
Practices with wound-heavy follow-up volume often see this problem inside broader multispecialty workflows, especially where foot, skin, vascular, or orthopedic issues overlap. If that sounds familiar, the operational lessons are similar to those we see on the orthopedics billing specialty page, where procedure support and documentation discipline directly affect payment reliability. For owners focused on the back end, this guide to medical billing denial management is the right companion to a template overhaul.
Wound Care Documentation FAQs
Is the default EHR wound template usually good enough
Usually not. Default templates often capture basic clinical description but leave too much optional. If fields like etiology, tissue composition, intervention details, and response can be skipped, the note may be clinically readable but financially weak.
What is the most common wound documentation mistake that leads to denials
The most common problem is incomplete linkage between assessment and treatment. The chart says what was done, but it doesn't document enough detail about the wound's characteristics, status, and response to justify why the service was necessary that day.
Should clinicians document photos in every wound case
That depends on payer policy, practice policy, and the clinical situation. Photos can strengthen continuity and audit defense when captured consistently, but they should supplement the written record, not replace precise measurements and structured findings.
How often should a practice audit wound documentation
Often enough to catch drift before it affects cash flow. In practice, owners should review denials, compare notes across clinicians, and audit whether the template is being completed consistently. If the same missing fields keep showing up, the problem is usually template design or workflow, not individual effort.
If your practice is seeing wound denials, repeated chart queries, or slow payment on procedure-heavy encounters, Happy Billing can help you find the leak. We review documentation workflows, billing logic, and denial patterns inside your current EHR, then show you where the note template is costing you reimbursement. If you want a practical starting point, request a free RCM audit and get a clearer view of what's blocking clean payment.