Medical Billing Services for Physicians: A 2026 Guide
Outsourcing billing pays for itself only when it fixes specific leaks in your revenue cycle. That is the standard. If a billing partner cannot cut denials, shorten A/R, and raise net collections after fees, it is not a solution. It is another expense line. Physician groups in Texas can also review our Texas medical billing services for state-specific support.
Physician practices lose margin in predictable places: inaccurate charge capture, weak claim scrubbing, slow follow-up, underworked denials, and patient balances that age out before anyone collects them. Owners who frame billing as an admin task miss the financial reality. Billing determines how much of the care you already delivered turns into cash.
That is the decision lens to use. Compare the vendor fee to the dollars you are currently failing to collect, not to one biller’s salary. A proper review starts with your baseline KPIs: first-pass acceptance rate, denial rate, days in A/R, percentage of A/R over 90 days, net collection rate, and cost to collect. If those numbers are weak, outsourcing is a financial decision, not a staffing decision.
This guide uses that framework. You will see how to evaluate medical billing services for physicians by break-even point, specialty-specific leakage risk, and the operating metrics that show whether a partner is producing a real return. For a related overview of revenue cycle management benefits for medical practices, review the full-cycle impact before you compare vendors. If your practice also operates in adjacent wellness services, you should also learn wellness clinic bookkeeping so your collections data and financial records stay aligned.
Why Smart Practices Treat Billing as a Profit Center
Billing controls realized revenue. If you treat it like back-office overhead, you will accept lower collections than your practice should produce.
Too many physicians run the wrong math. They compare a billing vendor’s percentage fee to a biller’s salary, then stop there. That misses the vital question: how much collectible revenue is your current process leaving behind each month?
Use a break-even test. Start with your baseline net collection rate, denial rate, days in A/R, A/R over 90 days, and cost to collect. Then estimate what even modest improvement would be worth. A one to three point gain in collections on a high-volume practice can outweigh the vendor fee fast, especially if your current team is stuck reworking avoidable denials, posting payments late, or letting old patient balances die on the ledger.
That is why disciplined operators treat billing as a profit center. The function does not just process claims. It determines cash velocity, labor efficiency, and how much of the care already delivered turns into usable revenue.
Outsourcing growth reflects that shift in how owners view the billing function, but the smarter takeaway is operational, not market driven. Practices do not hand off billing because it feels modern. They do it when internal performance stalls and the revenue loss is larger than the outsourcing fee.
The patterns are easy to spot:
- Denial volume keeps climbing: your staff keeps spending labor dollars on rework instead of prevention.
- Days in A/R stay high: charges are posted, but cash arrives too slowly to support hiring, payroll, and physician draws.
- A/R over 90 days is growing: old balances become less collectible every month.
- Coding support is inconsistent: documented work gets paid below the level earned.
- Turnover hits the billing desk repeatedly: each replacement resets payer knowledge, follow-up discipline, and productivity.
Here is the rule I give practice owners. If billing problems are showing up in your bank balance, they are already management problems, not clerical problems.
This section of the decision is financial. You are buying lower leakage, faster follow-up, tighter reporting, and better yield on the visits you already worked to generate. For a broader look at the operational side of that equation, review these revenue cycle management benefits for medical practices.
A practice that wants stronger margins also needs clean accounting around the revenue cycle. If you offer adjacent wellness services, learn wellness clinic bookkeeping so your books, deposits, and collections reporting stay aligned.
Judge billing the same way you judge any other investment. Measure whether it reduces A/R days, raises net collections, cuts preventable denials, and produces more cash after fees. If it does, it is a profit center.
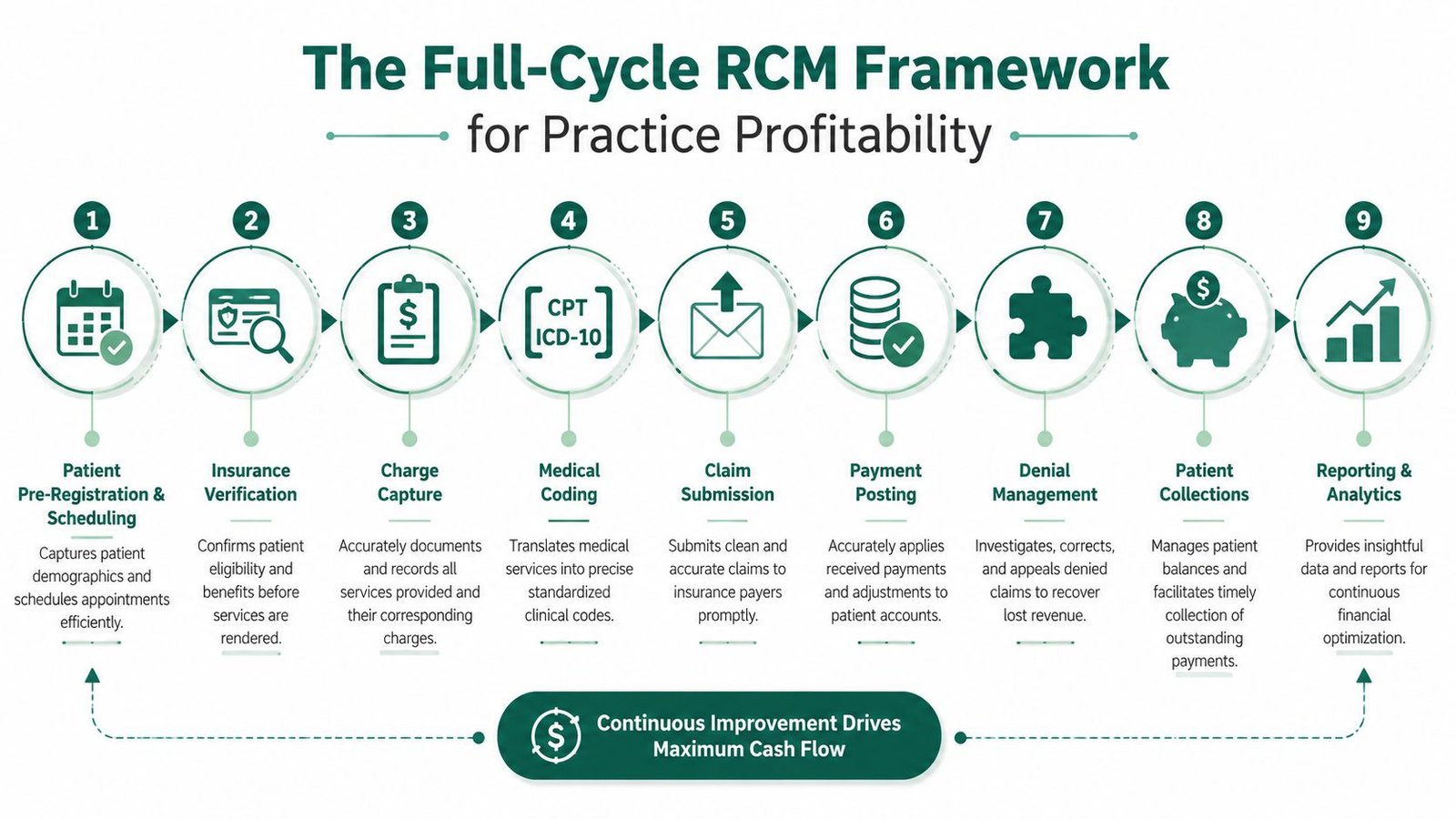
The Full-Cycle RCM Framework for Practice Profitability
Billing either protects margin at every handoff or bleeds revenue in small, repeatable ways. Practices that outperform on collections do not rely on claim submission alone. They control the full cycle, from front-desk data capture to denial prevention to payment variance review.
That matters because revenue loss usually starts upstream. An eligibility miss at scheduling, weak documentation at the visit, or a coding mismatch after the visit can all produce the same result: slower cash, higher rework, and lower net collections. By the time a denial appears, the practice is already paying for a process failure that should have been caught earlier.
The four operating pillars that actually move cash
Charge capture and claim submission
Clean claims start before the encounter closes. Scheduling, registration, eligibility checks, authorization status, and chart completion all affect whether the claim will pay cleanly.
This is the first place I look when a practice says cash is inconsistent. Missing diagnosis pointers, unsupported modifiers, incorrect place of service, and incomplete demographics create rejections that should never hit the payer. A billing partner should run claim edits, hold bad claims before submission, and tighten provider feedback loops so documentation supports the code set being billed.
Denial management
Denial work should reduce future denials, not just close old tickets.
A capable team tracks denial reasons by payer, provider, CPT family, and location. That tells you whether the problem sits with registration, coding, prior authorization, filing limits, or undertrained follow-up staff. If your vendor cannot show denial trends with root causes and corrective action, they are doing clerical work, not managing revenue.
The goal is simple. Fewer preventable denials next month than this month.
Payer and patient follow-up
Unworked A/R is not an accounting issue. It is lost cash.
Follow-up needs rules, ownership, and timing. Every unpaid claim should have a next action date. Every underpayment should be compared against contracted rates. Every patient balance should move through a defined collection sequence. If your reports cannot show where dollars are stuck by aging bucket, payer class, and claim status, you do not have enough control over collections to judge vendor performance.
This is also where technology matters. Clearinghouse workflows, eligibility tools, payment posting rules, and account security all affect speed and accuracy. Practices that depend on outside platforms should also vet vendors that handle IT and cybersecurity for Canadian healthcare, especially if remote teams or cross-border infrastructure are involved.
Credentialing and enrollment
Enrollment delays can wipe out the value of a busy schedule. A physician can see patients for weeks and still wait on payment because payer records are incomplete, group affiliations are wrong, or revalidation was missed.
Credentialing belongs inside the revenue cycle because it determines whether claims are billable, payable, and paid at the correct rate. If your billing company treats enrollment as somebody else’s job, expect avoidable delays and cleanup work later.
What a complete framework looks like in practice
Use this sequence to evaluate whether your current process is built to produce cash, not just activity:
- Before the visit: registration accuracy, insurance verification, authorization checks, fee schedule alignment
- At the visit: complete documentation, charge capture, coding support, modifier accuracy
- After the visit: claim scrubbing, submission speed, payment posting, underpayment detection
- After adjudication: denial analysis, appeals, patient collections, KPI reporting
That sequence gives you a practical way to measure outsourcing ROI. If an outside billing team improves first-pass acceptance, lowers denial volume, reduces A/R over 90 days, and raises net collections after fees, the model is working. If those numbers do not move, the vendor is not fixing the full cycle.
For a closer operational view, review this RCM framework for physician practices.
Why Specialty-Specific Billing Is Non-Negotiable
Generic billing breaks down fastest in specialties where one documentation mistake changes reimbursement, triggers manual review, or creates repeat denials.
Modifier-driven and rule-heavy specialties can’t afford a vendor that “does a little of everything.” They need teams that understand where revenue leakage happens. Under CMS and payer documentation standards, that means tying coding choices to defensible chart support, not just pushing claims faster.
Modifier 25 is a perfect example
One of the most common denial triggers is modifier 25 misuse on same-day E/M plus procedure claims. The issue is not whether the provider documented something. The issue is whether the note proves a significant, separately identifiable E/M service with distinct medical decision making, rather than a routine pre-procedure exam. Payers often flag these claims for manual review when the documentation doesn’t support separation (modifier 25 denial risk and documentation standards).
For an orthopedic, dermatology, ophthalmology, or pain practice, that directly affects cash. If you bill an office visit with a same-day procedure and the note reads like one combined event, the payer has an easy reason to deny or downshift payment.
The fix is operational:
- Separate the note structure: The E/M problem, assessment, and plan should stand apart from the procedure note.
- Audit by provider: Some clinicians create most of the pattern risk.
- Retrain on recurring payer edits: Denials often cluster around the same workflows.
If your vendor can’t explain why modifier 25 gets denied in your specialty, they can’t protect your margin.
Specialty workflows create different leakage points
Cardiology, anesthesia, orthopedics, and behavioral health do not fail in the same place.
- Cardiology: Financial risk often sits in diagnostic versus interventional coding logic, imaging documentation, and payer-specific edits. If you want a concrete example of specialty depth, this cardiology billing resource is the kind of specialized lens you should expect.
- Anesthesia: Base units, time units, modifiers, and concurrency create obvious underbilling and denial risk when the workflow is generic.
- Orthopedics and pain: Global periods, procedure bundles, and multiple procedure reductions punish sloppy review.
- Behavioral health: Authorization management and visit-level payer rules matter more than most generalist vendors admit.
This is also where systems matter. Specialty billing now depends on secure workflows, payer portal discipline, and access controls across distributed teams. If your group is reviewing cross-border support models or hardening infrastructure, resources on IT and cybersecurity for Canadian healthcare are useful because billing performance and security operations now overlap more than most owners expect.
If you’re comparing vendors, ask one blunt question: “Show me the denial patterns you see most often in my specialty, and show me the workflow you use to prevent them.” If they answer with generic service lines, move on.
Your Vendor Selection Checklist
Most physicians choose a billing company the wrong way. They ask about price first, then discover later that reporting is weak, follow-up is slow, and nobody owns denial prevention.
The better sequence is performance, visibility, workflow fit, and only then pricing. That matters because the primary inflection point is simple: physicians often underestimate the downside of in-house billing, and outsourcing makes financial sense when revenue leakage from high denials, aging A/R, and staff turnover exceeds the fee of a specialized RCM partner that can guarantee performance metrics (financial tradeoff of in-house versus outsourced billing).
Questions every owner should ask before signing
Performance and reporting
Ask for the dashboard before you ask for the proposal.
You should see exactly how the vendor reports on denial categories, aging buckets, payer follow-up, underpayments, and provider-level trends. If reporting is vague, accountability will be vague too.
Ask:
- What do you report monthly: denial trends, net collections, aging by bucket, payer lag
- How do you separate rejections from denials: they are not the same operational problem
- How do you show root cause: payer issue, registration issue, coding issue, documentation issue
Technology and workflow fit
A vendor should adapt to your operating environment, not force disruption for its own convenience.
Ask whether they work inside your current EHR or PM system, how they handle task queues, and how quickly they turn same-day charges. If they need a major migration just to start billing, friction will show up before collections improve. Happy Billing is one example of a model that operates inside the existing EHR while combining AI-assisted workflows with human auditors, which is the kind of setup many practices now prefer when they want change without replacing core systems.
Security and compliance
This is not boilerplate. It affects vendor risk, payer trust, and your own exposure.
If a vendor uses offshore or distributed teams, ask how they control PHI access, monitor activity, and maintain HIPAA discipline. Owners evaluating software-heavy billing workflows should also understand the basics of protecting patient data in software because security failures are expensive distractions.
Pricing and incentives
The wrong pricing model can hide a bad operating model.
Ask what is included, what triggers extra fees, and whether credentialing, old A/R work, patient collections, and denial appeals are bundled or separate. Then ask the question vendors hate: “How does your compensation align with improved collections and cleaner A/R?”
In-house billing vs outsourced RCM
| Factor | In-House Billing | Outsourced RCM Partner |
|---|---|---|
| Staffing risk | Dependent on one or two key employees | Broader team coverage and continuity |
| Specialty expertise | Often limited unless you hire deeply by specialty | More likely to provide specialty-focused workflows |
| Reporting discipline | Varies by manager and software use | Usually structured if the vendor is mature |
| Denial prevention | Often reactive because staff are overloaded | Should be process-driven if the vendor is strong |
| Credentialing coordination | Frequently split from billing operations | Can be integrated into the revenue cycle |
| Technology burden | Practice owns setup, training, and maintenance | Shared or vendor-managed workflow burden |
| Visibility | Immediate if managed well, weak if unmanaged | Strong only if dashboards and review cadence are defined |
| Cost predictability | Salaries are predictable, leakage is not | Fees are visible, ROI depends on collections improvement |
Owner test: If a vendor can't explain how they will reduce leakage before they talk about fees, they are selling labor, not outcomes.
If you want a sharper list of warning signs, review these medical billing company red flags.
The Onboarding Process What to Expect When You Switch
The biggest reason practices delay switching billing partners is fear of disruption. Most of that fear comes from bad transitions, not from switching itself.
A controlled onboarding process should feel like a staged handoff, not a hard cutover. In our experience, the cleanest transitions happen when the new partner treats implementation as a revenue-protection project from day one.
Phase one starts with an audit, not a promise
The first step should be discovery. That means reviewing current denial categories, aging patterns, charge lag, payer enrollment status, and documentation weaknesses by provider.
If a new billing company wants to start immediately without auditing your current leakage points, that's a red flag. You don't fix a revenue cycle by guessing.
Setup should be operational, not theoretical
After discovery, the team should map your workflows inside the existing stack. That usually includes EHR and practice management access, payer portal setup, clearinghouse coordination, enrollment review, and responsibility splits between your front office and the billing team.
A practical transition plan usually includes:
- System access controls: who can see, edit, and submit what
- Payer enrollment review: active, pending, or broken enrollments
- Charge routing rules: who posts encounters and when
- Open A/R ownership: what happens to old balances and denied claims
Go-live should include overlap
A short parallel period is often smart. It lets the new team validate charge capture, claim formatting, edits, and payment posting before full handoff.
That overlap also protects your physicians. If there is a recurring issue with a payer rule, modifier pattern, or provider documentation habit, it shows up early while the old process is still available as a reference point.
Clean onboarding isn't about speed alone. It's about protecting collections while the new workflow takes control.
Once the handoff is complete, reporting should become more transparent, not less. If the first month after transition feels quieter than before, ask questions. A good partner gets louder with data as soon as they take over.
Measuring the ROI of Your Billing Partner
If you can't measure ROI, you don't have a billing strategy. You have a vendor relationship.

The fastest way to evaluate medical billing services for physicians is to compare pre-switch performance to post-switch performance on a short list of financial indicators. Not vanity metrics. Revenue metrics.
The KPIs that matter
Start with these:
- Days in A/R: Is cash moving faster?
- Denial rate: Are fewer claims falling out of the cycle?
- Net collections: Are you keeping more of what you earned?
- First-pass claim quality: Are claims reaching payers in payable condition?
- Lag to claim submission: Are charges getting out quickly enough?
You don't need a complicated formula to judge progress. You need a baseline and a review cadence.
A simple owner-level ROI lens looks like this:
- Revenue recovered or protected
- minus billing fee
- minus internal labor still required to support billing
- equals net operational gain
Watch for documentation-driven underpayment
One of the easiest places to miss ROI is E/M leveling. Under the 2023 E/M framework, audits focus on medical decision making, not note length, and claims such as 99285 can be downcoded when the documentation does not support the required MDM intensity (E/M leveling and downcoding risk under the 2023 framework).
That matters beyond the emergency department. The lesson for owners is broader: if your providers are doing higher-complexity work but documenting in a way that supports lower reimbursement, your practice is bleeding revenue in a way most monthly reports won't show clearly.
A good billing partner should help surface:
- Provider-level level-distribution anomalies
- Payer-specific downcoding patterns
- Chief-complaint categories with repeat documentation gaps
The right vendor doesn't just collect faster. They show you where documentation habits are suppressing payment.
If you're comparing fees and trying to model the business case, this medical billing outsourcing cost guide will help frame what to compare beyond the percentage rate.
The cleanest next step is simple. Get your current numbers audited before you make a switch. A billing partner should be able to show you where the leaks are before they ask you to trust the fix.
FAQs From Practice Owners
How do I know if my practice should outsource billing or fix it in-house
Outsource when the problem is structural, not temporary. If denials repeat, A/R keeps aging, payer follow-up is inconsistent, and your billing knowledge lives in one or two employees, you don't have a staffing issue. You have a system issue. If your in-house team is strong and the problem is limited to one workflow, fix that first.
What should I expect from a medical billing company in the first few months
You should expect more visibility, tighter claim submission discipline, and clearer accountability for unpaid claims. You should also expect uncomfortable findings. A serious partner will show you where registration errors, documentation gaps, payer edits, or provider habits are suppressing collections. If the onboarding period feels vague, the operating model probably is.
Will outsourcing billing make me lose control of my revenue cycle
Only if you choose the wrong vendor. A well-run outsourced model increases control because reporting is cleaner, ownership is defined, and follow-up is more consistent. Loss of control usually comes from poor dashboards, weak communication, and unclear division of responsibilities.
What should I ask before switching to a new billing partner
Ask how they will report on denial trends, who owns old A/R, how they handle payer enrollments, what specialty-specific denial patterns they see in your field, and how they work inside your current systems. Then ask for a real audit. If they can't identify your leakage before the contract starts, they're not ready to manage it after.
If your practice is comparing medical billing services for physicians, don't make the decision on percentage fees alone. Measure the cost of denials, old A/R, and underpaid claims first, then compare that leakage to what a stronger RCM model could recover. The fastest way to do that is to book a free billing audit with Happy Billing. You'll get a clearer view of where cash is stalling, what your current workflow is missing, and whether switching providers will improve collections.