Master Revenue Cycle Management for Physician Practices
Cash flow problems in physician practices usually start long before a claim hits the clearinghouse. They start at registration, scheduling, coding, and payment review. A single missed eligibility check, an authorization gap for CPT 90837, a global-surgery billing error in orthopedics, or the wrong anesthesia concurrency modifier can delay or reduce payment even when the clinical work was done correctly.
I see the same pattern in audits. Revenue rarely leaks out through one large failure. It leaks through repeated process errors that staff begin to treat as normal: inactive coverage entered at check-in, modifier 25 appended without documentation support, secondary claims never crossing over, or payer underpayments posted without comparing the allowed amount to the contract.
Revenue cycle management is the control system for those failures. It connects front-desk intake, charge capture, coding, claim submission, denial follow-up, and patient balance resolution so the practice gets paid the correct amount within the expected time frame.
If you need a broader definition before getting into workflow and metrics, this guide on what revenue cycle management means in practice gives that foundation.
For physician owners, that is the point. Strong RCM protects margin at the code level, whether the problem is a cardiology stress test billed without medical necessity support, an OB claim filed against the wrong global package, or an underpaid 99214 that no one appealed.
What Is Revenue Cycle Management in a Physician Practice
Revenue cycle management for physician practices is the full financial lifecycle of a patient account, from scheduling and registration through claim submission, payment posting, denial recovery, and final patient balance resolution. It starts before the visit and ends only when the practice has collected the correct reimbursement from the payer and the patient.
That definition matters because many owners still treat RCM as “billing.” Billing is only one segment of the cycle. If the front desk captures the wrong member ID, if the physician documents an E/M service without support for modifier 25, or if staff miss a payer authorization requirement, the claim problem was created long before anyone hit submit.
A useful primer on the broader scope is this overview of what revenue cycle management means in practice.
Why RCM decides practice stability
A healthy revenue cycle does three things at once. It converts encounters into valid claims, it protects contract reimbursement, and it keeps staff from wasting hours on preventable rework.
A weak cycle does the opposite. Charges lag. Denials stack up. Aging grows. The business starts financing its own inefficiency.
Practical rule: Every denied claim already had a root cause somewhere upstream. The denial team often finds the problem, but rarely created it.
What good RCM looks like in daily operations
In real audits, strong physician practices usually share a few habits:
- Registration discipline: Staff confirm demographics, payer details, and coverage every visit, not just for new patients.
- Authorization control: Someone owns prior auth tracking for high-risk services and verifies the approval matches the rendering provider, place of service, and CPT code set.
- Code-level review: Charges aren’t released blindly. Teams check diagnosis support, modifier use, and payer edits before submission.
- A/R ownership: Aging isn’t just reviewed. It’s worked by payer, denial reason, and timely filing risk.
For physician owners, that’s the key point. Revenue cycle management isn’t an administrative layer around care. It’s the mechanism that keeps the practice solvent while clinicians focus on medicine.
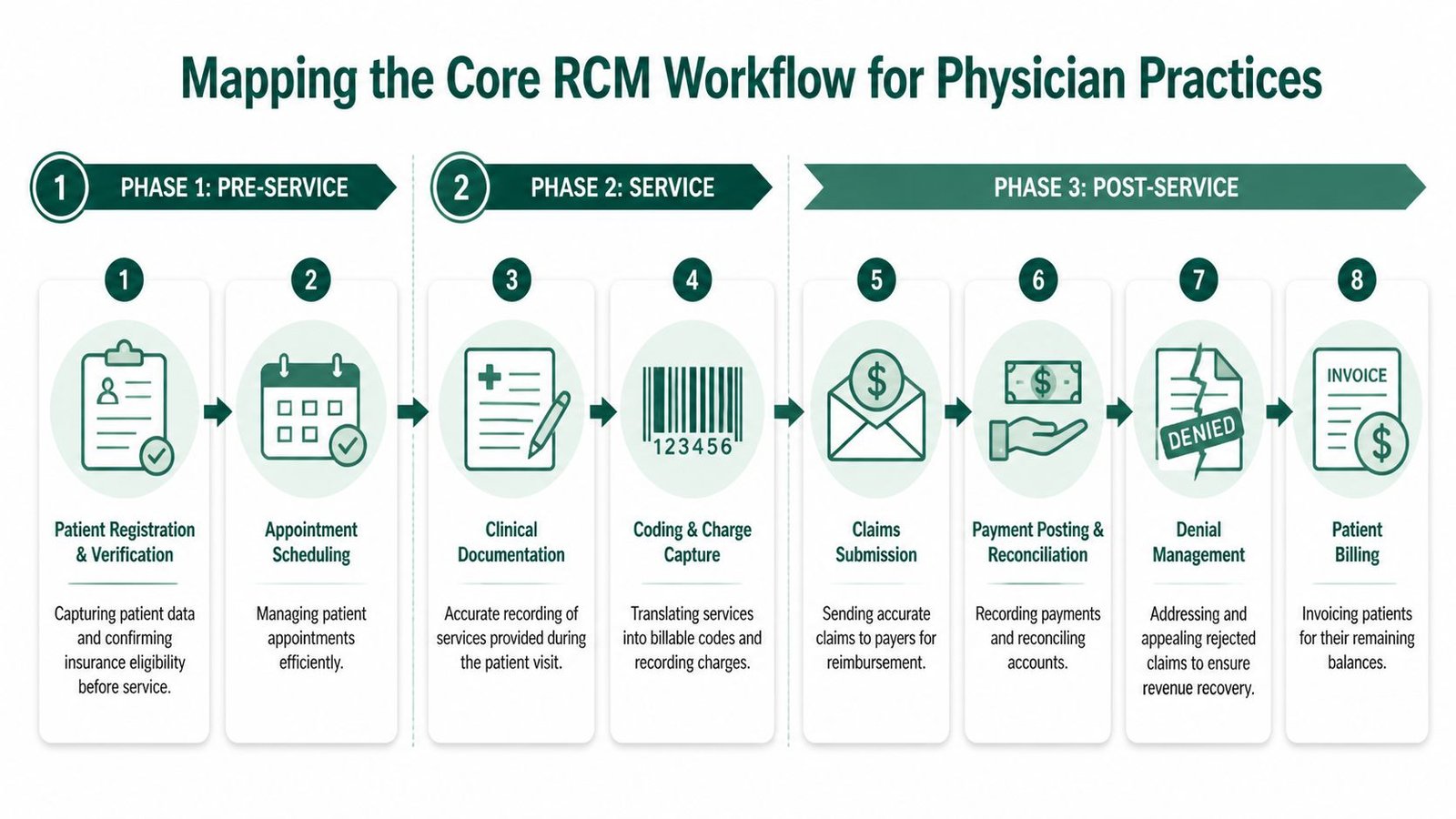
Mapping the Core RCM Workflow
The workflow is easiest to fix when you view it chronologically. Problems that appear in post-service follow-up usually began in pre-service setup or mid-cycle coding.
A practical operations guide for tightening handoffs across the cycle is this resource on revenue cycle workflow improvements.
Pre-service controls
Pre-service is where practices either prevent denials or schedule them.
Appointment scheduling sounds operational, but it affects revenue immediately. If a patient is booked with the wrong provider, at the wrong location, or under inactive coverage, the claim may never be clean. Registration has to validate name, DOB, subscriber data, plan details, and current eligibility before the visit.
Eligibility and benefits verification should answer basic reimbursement questions before the patient arrives. Is the plan active? Is a referral required? Is there specialist authorization? Does the payer require site-of-service limits or rendering-provider enrollment for this CPT family?
Credentialing belongs in this stage too, even though many groups treat it as a separate admin function. In multi-payer and multi-state environments, outdated manual credentialing processes can drain 10 to 20 percent of revenue through undetected lapses, as described in MedTrainer’s discussion of credentialing gaps that dry up revenue. If the provider isn’t properly enrolled, the cleanest claim in the world still won’t pay correctly.
Mid-cycle execution
Mid-cycle begins when care is delivered and documentation starts supporting payment.
Clinical documentation has to support the billed service, not just the clinical story. If a cardiologist bills CPT 93306, the record has to support the complete transthoracic echocardiography service. If only the professional component applies, modifier 26 may be necessary depending on the billing arrangement. If an orthopedist returns a patient to the OR during a postoperative period, the note must show whether the subsequent procedure is staged, related, or unrelated because that determines modifier 58 or 79.
Charge capture is where many practices leak revenue, often going undetected. Hospital-based and procedural specialties are especially exposed. Miss one add-on, one supply line, one time-based entry, or one correctly supported modifier, and the underbilling often survives unnoticed.
Post-service recovery and collection
Claims submission is not just transmission. It’s the last checkpoint before avoidable rework. Scrubbing should catch missing modifiers, diagnosis mismatches, invalid provider identifiers, and payer-specific edits.
After submission, payment posting and reconciliation must go beyond autoposting. Staff should compare ERA results to expected allowables and identify underpayments, bundling reductions, or denial patterns that need escalation.
The final steps are denial management, patient billing, and A/R follow-up. In these final steps, discipline matters most:
- Denial triage: Separate registration denials, coding denials, authorization denials, and medical necessity denials.
- Appeal logic: Resubmit corrected claims only when correction is the issue. File formal appeals when the payer misapplied policy.
- Patient balance controls: Bill patients only after payer adjudication is accurate and contractual adjustments are correct.
The practice that works denials well usually isn’t the practice with the best RCM. The best RCM is the one that prevents the denial from appearing in the first place.
The Key Performance Indicators of a Healthy Revenue Cycle
A practice can stay busy all month and still miss payroll targets if the wrong claims are stuck at day 45, denied for CO-16, or underpaid against the contracted fee schedule. A useful KPI set catches those leaks early and points to the exact workflow that needs correction.

If you want a tighter dashboard, this guide on medical billing KPIs to track is a useful companion.
Days in A/R
Days in A/R is still the fastest operational read on whether cash is moving. As noted earlier, many well-run physician practices target under 36 to 40 days. Once the number rises, the fix is rarely “work aging harder.” The key question is where the lag started.
Formula:
- Days in A/R = Total A/R ÷ Average daily charges
Review it by payer and aging bucket, then tie it to denial codes and claim status. If Medicare is paying on time but a commercial payer has a growing 61 to 90-day bucket, the issue may be authorization defects, missing records on review, or underworked secondary claims. In orthopedics, I often see days in A/R rise after postop claims are held for modifier review. In cardiology, the drag is more often missing documentation for stress testing or rhythm monitoring. The KPI matters because it tells you where to audit next.
Denial rate and clean claim rate
Denial rate measures how often the practice forces rework into the system. A low clean claim rate usually shows the same problem from the opposite angle.
IMED Claims cites a common target of keeping claim denial rate under 5%, and that benchmark is useful if you break it down far enough to act on it. A 4% denial rate with mostly timely filing denials is a front-end process failure. A 4% denial rate driven by CO-97 bundling issues, modifier misuse, or medical necessity edits points to coding and edit configuration.
Track denial categories, not just the total:
| KPI | Target | What a poor reading usually means |
|---|---|---|
| Days in A/R | Under 36 to 40 days | Submission delays, denials, weak follow-up |
| Denial rate | Under 5% | Eligibility gaps, auth failures, coding errors |
| Clean claim rate | High on first pass | Inconsistent edits, missing documentation, modifier mistakes |
Specialty context matters here. An ENT practice with repeat denials on nasal endoscopy claims should review diagnosis support and payer policy for the CPT billed, not just ask staff to “be more careful.” An orthopedic group seeing denials on fracture care follow-up should audit global-period logic and modifier assignment. If the clean claim rate drops after adding a new payer or EHR template, that is a system issue, not a staff attitude problem.
Bad debt and net collection discipline
Bad debt is often treated like a patient collections problem. In practice, it usually starts earlier.
IMED Claims notes a benchmark range of 2 to 3% of net patient revenue for bad debt write-offs. If a practice moves above that range, I check three things first. Were estimates accurate. Were statements sent after payer adjudication and correct contractual adjustment. Did staff collect at check-in for high-deductible plans when eligibility data already showed patient responsibility.
Net collection rate belongs on the same dashboard because it shows whether the practice received the dollars allowed under its contracts. If posted payments on CPT 20610, 99214-25, or 93000 keep landing below the contracted allowable and nobody compares ERA amounts to the fee schedule, the practice can look productive while losing margin on every session.
Audit lens: A KPI earns dashboard space only if it leads to a specific correction, such as rewriting a front-desk eligibility script, tightening edits for modifier 25, or escalating repeated underpayments to the payer contracting team.
Solving Specialty-Specific Billing and Coding Challenges
Generic advice fails in specialty RCM because payer edits are code-specific. The claim doesn’t deny because your team lacks motivation. It denies because one code, one modifier, one authorization, or one policy rule didn’t match what the payer expected.

For practices dealing with postoperative and procedural complexity, this overview of orthopedic revenue cycle management is worth reviewing.
Orthopedics and global period mistakes
Orthopedic denials often come from misunderstanding the postoperative package. If a surgeon performs another procedure during the global period, staff need to determine whether it is staged, more extensive, or unrelated.
Modifier 58 is used for a staged or related procedure during the postoperative period. Modifier 79 is used when the procedure is unrelated to the original surgery. Those are not interchangeable. Using 79 when documentation supports a staged return can trigger avoidable payer disputes. Using 58 without chart support can create audit risk.
A common failure point is the op note. If the physician doesn’t clearly document why the patient returned and how the second procedure relates to the original surgical plan, billing is guessing.
Anesthesiology and concurrency rules
Anesthesia billing is where weak RCM shows up fast because time units, base units, and concurrency logic must align. Modifier selection matters. Clarity RCM notes that incorrect or missing modifiers cause frequent denials, and in anesthesiology a mismatch in concurrency modifiers such as QK can reduce reimbursement by 20 to 50 percent per claim under NCCI-related payer edits in its discussion of revenue cycle management steps and modifier accuracy.
That matters operationally. If the claim uses QK for medical direction, the record has to support the required supervision conditions. If the anesthesiologist personally performed the case, the modifier logic changes. If time units don’t reconcile with the anesthesia record, payer edits are expected, not surprising.
Cardiology and component billing
Cardiology groups regularly hit issues around diagnostic imaging, professional versus technical components, and procedure bundling. A practice billing CPT 93306 has to know whether it owns both components or only the professional read. If only interpretation is billable, modifier 26 may be necessary.
The denial here often isn’t a coding textbook problem. It’s an operational one. The billing team may not know the current site arrangement, equipment ownership, or whether another entity already billed the technical component.
Mental health and authorization-sensitive services
Behavioral health groups face a different kind of leakage. The code may be correct, but payment stalls because authorization tracking broke earlier in the cycle.
Take CPT 90837. The service itself isn’t exotic. The risk sits in payer rules around visit limits, authorization requirements, and documentation support for medical necessity. When staff schedule recurring therapy without validating current authorization status, the denials arrive in batches.
A practical specialty workflow usually includes:
- Code-specific edit rules: Build edits around recurring risk codes such as 90837, 93306, and anesthesia concurrency claims.
- Modifier governance: Require coder review when modifiers 25, 26, 58, 79, QK, AA, or similar specialty modifiers are used.
- Payer-policy mapping: Keep carrier-specific rules tied to the actual CPT families your physicians bill most.
Choosing Your RCM Model In-House vs Outsourcing
The right RCM model depends less on ideology and more on failure points. Some practices do well in-house because they have experienced staff, stable payer mix, tight oversight, and low turnover. Others keep billing internal long after the warning signs are obvious because “control” feels safer than change.
A balanced framework helps. This explainer on in-house vs outsourced medical billing covers the same decision from an operating-model perspective.
The trade-offs that matter
Here is the comparison that usually matters most to physician owners:
| Factor | In-House RCM | Outsourced RCM |
|---|---|---|
| Cost | Fixed payroll, software, training, and management overhead | Variable service cost tied to scope and performance terms |
| Control | Direct visibility into staff and workflows | Less day-to-day control, stronger need for governance |
| Scalability | Harder during growth, leave coverage gaps, or specialty expansion | Easier to scale across providers, payers, and locations |
| Specialized expertise | Depends on who you can hire and retain | Broader payer, coding, denial, and credentialing depth if vendor is specialty-focused |
What works in-house and what usually fails
In-house works when leadership actively manages it. That means daily claim holds review, weekly denial analysis, monthly payer trend review, credentialing oversight, and periodic coding audits. It doesn’t work when one biller carries registration corrections, claim edits, payment posting, appeals, and patient calls at the same time.
The common in-house failure pattern looks like this:
- Single-point dependency: One key employee knows everything.
- No specialty guardrails: Complex modifiers and payer edits live in memory, not process.
- Weak reporting cadence: Owners see month-end totals but not leading indicators.
Outsourcing works when the practice defines scope, escalation paths, and measurable expectations. It fails when leadership hands over billing without validating security controls, reporting depth, coding expertise, or who owns denials versus who merely reports them.
A bad outsourcing relationship doesn’t remove administrative burden. It adds another layer of it.
Transition to outsourcing checklist
If a practice is considering a transition, use a checklist instead of a sales demo impression.
Map your current leakage
Pull your top denied CPT codes, open aging by payer, authorization denials, and credentialing risk points.Review security and compliance
Confirm HIPAA controls, role-based access, audit trails, and business associate agreement terms.Set code-level responsibility
Decide who owns coding edits, modifier review, appeal drafting, underpayment analysis, and patient balance disputes.Define reporting rhythm
Require regular dashboards for A/R, denials, claim acceptance, aging movement, and payer-specific issues.Clarify implementation
Ask how the partner works inside your current EHR or PM system, how historical A/R is handled, and how unresolved denials transfer.Choose success metrics upfront
Don’t use vague goals. Define what improved turnaround, stronger denial control, and cleaner claim flow should look like for your practice.
The best model is the one that closes leaks consistently. Ownership structure matters less than process quality.
Practical Next Steps to Optimize Your Revenue Cycle
Start with a 60-minute KPI spot-check. Pull your current days in A/R, denial rate, clean claim trend, aging by payer, and bad debt write-offs. If the numbers are hard to produce, that’s already a management problem.
Next, isolate one leak that has a clear owner. Don’t launch a full RCM overhaul on day one. Pick a repeatable issue such as modifier-related denials on procedural claims, missing authorization on recurring behavioral health visits, or aging tied to one payer’s documentation edits.
Then test a contained fix:
- Front-end leak: tighten eligibility and auth verification scripts
- Coding leak: add coder review for high-risk modifiers like 25, 26, 58, 79, QK, or AA
- Back-end leak: assign payer-specific follow-up and appeal accountability
Finally, benchmark your process critically. If your team can’t produce timely reports, can’t explain why a code family keeps denying, or can’t keep credentialing current across payers, the issue isn’t effort. It’s operating design. Revenue cycle management for physician practices improves when leaders stop treating denials as isolated events and start fixing the system that created them.
Frequently Asked Questions About RCM
How can a small physician practice track RCM performance without advanced analytics
Start with a simple monthly dashboard. Small groups don’t need enterprise BI to see whether revenue is leaking. They need a few consistent measures, reviewed on a fixed schedule.
That approach works because it makes bottlenecks visible. Revantage notes that a family practice using simple monthly dashboarding reduced A/R days by 18% after identifying charge-entry bottlenecks in its article on hidden revenue gaps in medical practices. For a small office, that’s the model to copy. Keep the dashboard basic: aging, denials, top rejected CPT codes, and unapplied cash issues.
What are the biggest front-desk mistakes that lead to denials
The most common ones are outdated insurance data, skipped eligibility checks, missing referrals, and authorizations that don’t match the actual rendering provider or scheduled service. Front-desk teams also create downstream trouble when they copy old insurance data forward without re-verifying active coverage.
In specialty settings, one registration error can invalidate an otherwise correct claim. A therapy visit may be performed under an expired authorization. A cardiology diagnostic service may be scheduled under the wrong place-of-service assumptions. A surgical follow-up may be registered without recognizing the patient is still in a global period.
What should physician owners watch for in an RCM vendor contract
Watch how fees are defined, how performance is reported, and where responsibility stops. You want clear language around claim submission, denial follow-up, coding support, payment posting, underpayment analysis, and patient billing.
Ask direct questions. Is the company being compensated on actual collections or on charges? Who handles old A/R? Who files appeals? Who manages credentialing issues that block payment? If those answers are vague, the relationship will be vague when revenue stalls.
How does RCM strategy affect the patient financial experience
A strong RCM strategy reduces confusion before the first statement goes out. Patients get cleaner estimates, more accurate balances, and fewer corrected bills after payer adjudication changes.
That matters for collections and reputation. When eligibility is verified upfront, benefits are explained clearly, and claims are adjudicated correctly before patient billing, staff spend less time defending broken balances. Patients don’t want a “billing experience.” They want the right bill, at the right time, with a clear explanation of what they owe and why.
Happy Billing helps physician practices tighten the full revenue cycle without forcing an EHR migration. If your group needs specialty-aware support for anesthesia modifiers, orthopedic global periods, cardiology procedure coding, behavioral health authorizations, denial recovery, or credentialing oversight, explore Happy Billing and review their specialty expertise at their physician specialty billing pages.