What Is a Superbill in Medical Billing: Your Complete Guide
TL;DR: A superbill is an itemized document that captures every billable service from a patient encounter and serves as the source record for claim creation or patient reimbursement, especially for out-of-network care. After ICD-10 took effect on October 1, 2015, diagnosis coding expanded from about 14,000 codes to over 68,000, which raised the stakes for superbill accuracy because coding gaps, CPT to ICD mismatches, and missing modifiers became common denial triggers.
If you're dealing with repeated payer pushback, out-of-network patients asking for corrected paperwork, or staff reworking claims because the visit details didn't make it cleanly from chart to bill, you're already feeling what a weak superbill costs. The problem usually isn't the final claim form. It's the document upstream.
Practice owners often think of the superbill as a checkout artifact. In real operations, it's closer to a revenue integrity document. If the superbill is incomplete, your claim build is shaky, your denial defense is weaker, and your patient reimbursement process becomes harder than it needs to be.
What a Superbill Is and Why It Matters for Your Practice
A superbill in medical billing is a detailed, itemized document created by the provider after the encounter. It captures the services performed, the diagnoses that support them, and the billing identifiers needed to turn clinical documentation into a reimbursable claim or a patient-submitted out-of-network request.
That sounds basic. It isn't.
When a front desk team prints a generic visit summary and calls it a superbill, payers usually expose the gaps fast. Missing modifiers, weak diagnosis linkage, absent provider identifiers, and vague service descriptions don't just slow things down. They create preventable rework and open the door to denials.
Why this document became more important after ICD-10
The coding environment got much more demanding after the U.S. adopted ICD-10 on October 1, 2015. Diagnosis codes expanded from approximately 14,000 under ICD-9 to over 68,000 unique codes, which increased specificity but also made documentation and billing alignment much less forgiving, as outlined in this overview of superbills and ICD-10 billing specificity.
That matters because the superbill is where coding precision has to show up clearly. If your clinician documents an office visit and a minor procedure on the same date, your billing staff can't just infer everything later. The superbill needs to carry the logic that supports the claim.
Practical rule: A superbill isn't a receipt with codes added. It's the first billing document that has to make medical necessity, coding specificity, and provider identity line up.
The financial stakes are high. The same Combine Health summary notes that coding gaps, CPT-ICD mismatches, and missing modifiers appear in up to 30% of initial claims, and CMS reported $31.3 billion in Medicare Fee-for-Service improper payments due to coding errors in 2022.
What the superbill solves in day-to-day RCM
In a healthy workflow, the superbill closes the gap between charting and billing. It gives your team one encounter-level document that answers the questions payers will ask later:
- Who rendered the service with the correct provider identifiers
- What was done using CPT or HCPCS codes
- Why it was done using diagnosis coding that supports medical necessity
- Where it happened with the right place-of-service logic
- How the service should be interpreted when modifiers are required
If you want a simple way to think about it, the superbill feeds the downstream claim just like source documentation feeds an audit. A messy source creates messy output. For a practical look at how those encounter details move into the payer-facing document, review this medical claim form resource.
What works and what doesn't
What works is a specialty-aware superbill that mirrors how your clinicians document and how your payers adjudicate.
What doesn't work is:
- Using one generic template for every specialty, visit type, and payer situation
- Leaving modifier decisions to memory instead of building prompts into the form
- Treating diagnosis linkage as optional when it's central to payment logic
- Hand-editing details later in the day after the visit context is already gone
Owners usually notice the problem late. They see A/R stretch, more patient calls, payer requests for records, and a growing stack of corrected claims. The root cause often starts much earlier, at the superbill.
Anatomy of a Compliant Superbill
A compliant superbill has to do two jobs at once. It has to accurately reflect the clinical encounter, and it has to present the data in a format a payer can adjudicate without guessing.
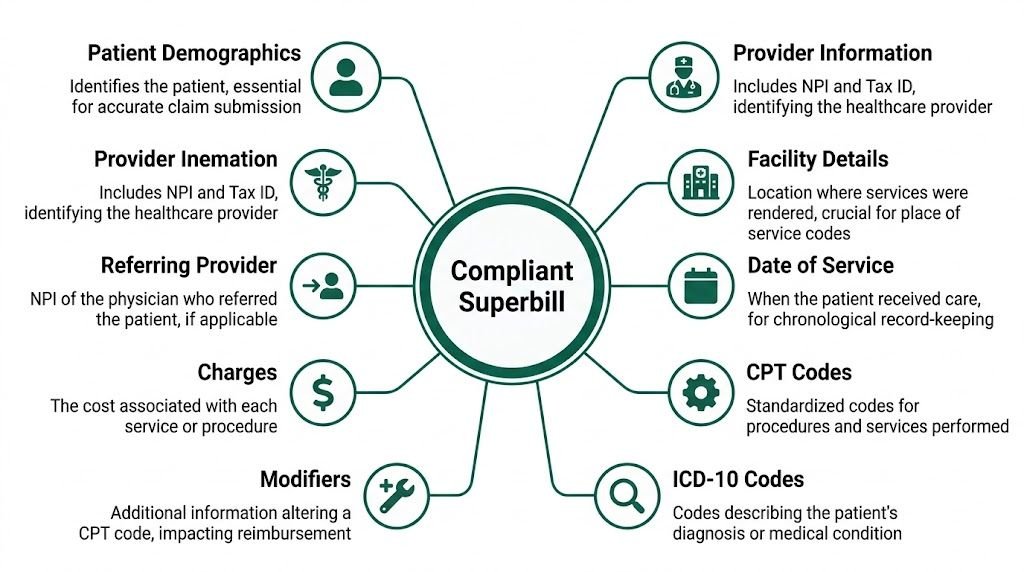
For out-of-network workflows, that standard is even tighter because the payer isn't getting a directly submitted provider claim with follow-up attached. The superbill itself has to carry enough detail for review. A technical summary from MedXpert notes that a proper superbill includes CPT codes such as 99213, ICD-10-CM diagnosis codes such as F32.9, relevant modifiers such as -25, POS code 11 for office, provider NPI, patient demographics, dates of service, service descriptions, and itemized charges. The same summary notes that incomplete coding and mismatched diagnosis linkage can trigger 20-30% denial rates in out-of-network submissions because payers apply NCCI edits. See their breakdown of required superbill elements and NCCI-related denial risk.
Provider and patient identifiers
The top of the superbill needs clean administrative data. That includes the rendering provider's name, credentials, NPI, and practice details, plus the patient's full name, date of birth, and address.
These fields aren't clerical filler. Payers use them to determine who rendered the service, where the service occurred, and whether the submission can be matched to the member record. If the NPI is wrong or missing, the rest of the document can be perfectly coded and still fail.
A referring provider field also matters when the service line or payer expects it. If you're in a specialty with referral-driven care, leaving that blank can create unnecessary questions later.
Date, place of service, and line-item charges
Every superbill needs the date of service and the Place of Service code. A common example is POS 11 for an office encounter.
Those details affect more than formatting. They shape payer logic. A code billed in the office may be reviewed differently than the same service in another setting, and date precision matters when payers assess frequency edits, duplicate billing concerns, or same-day modifier use.
Charges must also be itemized. A lump-sum total doesn't give the payer enough structure to evaluate the service lines individually.
The fastest way to create denials from a technically correct visit is to collapse line items that should've stayed separate.
CPT, ICD-10, and diagnosis linkage
At this juncture, most superbills either hold up or fall apart.
A line for CPT 99213 tells the payer an established patient office visit level 3 was performed. By itself, that isn't enough. It needs an ICD-10 diagnosis that logically supports the service. If the encounter is tied to F32.9, the diagnosis and procedure pairing has to make sense in the context of the visit documentation.
The issue isn't whether each code is valid on its own. The issue is whether they belong together.
Use the superbill to make that linkage explicit. Don't force billers to reverse-engineer medical necessity from chart notes after the fact.
Modifiers and why generic forms miss them
Modifiers are where many otherwise decent superbills fail.
If the provider performs a significant, separately identifiable E/M service on the same day as another procedure, modifier -25 may be required on the E/M line. If the form doesn't prompt for that review, staff may submit the service unmodified, and payer edits may treat the E/M as bundled or unsupported.
A compliant superbill should have room for modifiers at the line level, not buried in notes. The same goes for HCPCS when applicable.
Here is the minimum field logic I want to see on a usable superbill:
- Encounter data: Patient, provider, date of service, and location
- Procedure detail: CPT or HCPCS code, plain-language service description, and fee
- Diagnosis support: ICD-10 code linked to each service line where appropriate
- Claim logic detail: Modifier field, POS field, and referring provider field if needed
For teams that want to sanity-check whether their encounter data is complete enough to flow downstream, this completed CMS-1500 example is useful because it shows what the payer-facing form ultimately expects.
What a compliant superbill should look like operationally
A strong superbill is readable, structured, and hard to misuse. The best versions don't rely on memory. They build prompts into the form itself.
That means:
- Common codes are preloaded for the specialty, but not forced when they don't fit
- Modifier fields are visible on each relevant line
- Diagnosis linkage is explicit instead of implied
- Charge capture is itemized instead of summarized
- Signature or authentication workflow is defined so there isn't confusion about finalization
If your billers regularly have to stop and ask what the provider meant, your superbill isn't compliant enough for real-world payer scrutiny, even if it technically contains most of the required fields.
Superbill vs Invoice vs Claim Form A Clear Comparison
Practice teams mix these up all the time, and the confusion creates workflow errors. A superbill is not the same thing as a patient invoice, and it isn't the same thing as a CMS-1500 claim form.
The simplest way to separate them is by purpose. The invoice asks for payment or documents a balance. The claim form is the formal payer submission. The superbill sits between clinical care and reimbursement logic.
Document Comparison
| Attribute | Superbill | Patient Invoice | Claim Form (CMS-1500) |
|---|---|---|---|
| Primary purpose | Captures coded encounter details for reimbursement support | Requests payment or reflects patient balance | Submits billable services to payer for adjudication |
| Primary audience | Patient, billing staff, payer reviewer in OON context | Patient or guarantor | Insurance payer |
| Includes CPT codes | Yes | Not necessarily | Yes |
| Includes ICD-10 diagnosis codes | Yes | Usually no | Yes |
| Includes modifiers | Should, when relevant | Usually no | Yes |
| Includes provider NPI | Yes | May not | Yes |
| Includes itemized charges | Yes | Yes | Yes |
| Functions as a direct payer claim | No | No | Yes |
| Best use case | Encounter-level billing source document and OON reimbursement support | Collecting patient responsibility | Formal insurance billing |
Where practices go wrong
The biggest mistake is handing a patient an invoice when they require a superbill. An invoice might show that the patient paid for an office visit, but it often won't include the coded details needed for reimbursement review.
The second mistake is assuming the superbill itself is the claim. It isn't. The claim form is the payer submission format. The superbill is often the source document used to populate it.
If your staff can't explain the difference in one sentence, they will use the wrong document at checkout.
A practical workflow distinction
Use the superbill when you need coded encounter detail. Use the invoice when you need to collect or document payment. Use the CMS-1500 when you're submitting the claim to the payer.
That distinction also matters when you're trying to improve clean claims. A claim can only be clean if the source data is right. This explainer on what a clean claim means in medical billing is worth reviewing with your team because it clarifies why source-document accuracy matters before the claim ever leaves your system.
Strategic Uses of Superbills Beyond Out-of-Network Billing
Most articles stop at the basic definition: patients pay out of pocket, then submit the superbill for possible reimbursement. That's accurate, but it's incomplete.
A well-built superbill also gives your practice a stronger position when a payer challenges medical necessity, questions coding logic, or bundles services in a way that doesn't match the encounter. It can support deductible tracking and create a cleaner audit trail when patient responsibility becomes disputed.

A useful industry note from HSA for America points out that even when an insurer doesn't reimburse the patient, the superbill can still help the patient receive credit toward the deductible. Their discussion also highlights a larger gap: practices often underuse the superbill as documentation that can reduce payer disputes over medical necessity, coding accuracy, or service bundling. See their write-up on how superbills support deductible credit and denial appeals.
Denial prevention starts before the denial
When a payer reviews a service line, the fight is usually over one of a few things. Was the service medically necessary? Was it correctly coded? Should it have been bundled into something else? Was the modifier justified?
A detailed superbill helps you answer those questions early. For example:
- Same-day E/M and procedure scenarios: If you bill an office E/M and also report a procedure, the superbill should clearly separate the work and support the use of modifier -25 when appropriate.
- Distinct procedural service disputes: If two procedures are separate and not components of one bundled service, the source document should make that distinction obvious before the payer challenges it.
- Diagnosis support questions: A line item without clear diagnosis linkage leaves the payer room to downgrade, deny, or request records.
Deductible and patient responsibility tracking
Practice managers usually think of deductible tracking as a front-end eligibility issue. It isn't only that.
When a patient pays your office and later needs to prove that expense to the insurer, the superbill becomes the evidence packet. If the patient later says the insurer didn't apply the amount correctly, your team needs a document that shows exactly what was provided, on what date, by which provider, and at what charge.
That has two operational benefits:
- Cleaner patient communication: Staff can point to a formal coded record instead of reconstructing the visit from notes.
- Stronger balance defense: If a patient questions coinsurance or deductible handling, you have documentation that aligns the service and charge structure.
A vague receipt creates a customer service problem. A detailed superbill creates a defensible record.
Why specialty practices benefit most
Specialty groups see this first because their denials are rarely simple. The dispute is often about coding nuance, not whether the visit happened.
For example, a cardiology group may need to show that multiple diagnostic services weren't improperly bundled. An anesthesiology group may need to support concurrency and units. An orthopedic group may need to separate work inside and outside a global period. In each case, the superbill isn't just a checkout document. It's part of claim defense.
Practices that treat superbills strategically tend to have fewer internal handoffs later. Billers spend less time chasing clarifications. Managers spend less time handling escalations. And when appeals are necessary, the source document is already closer to what the payer wants to see.
Optimizing Superbills for High-Stakes Specialties
Generic superbills fail specialty practices because generic billing logic doesn't survive specialty edits. The form that works for a routine office encounter won't hold up for anesthesia concurrency, behavioral health authorization requirements, interventional cardiology coding, or orthopedic global-period disputes.
An Amazing Charts discussion points out that search results usually describe superbills in generic terms while missing the specialty-specific components that drive denials. Their summary highlights examples such as anesthesiology base units and modifiers, mental health authorization details, orthopedics global periods, and cardiology imaging bundling. See their overview of specialty-specific superbill requirements.
Anesthesiology needs unit logic on the form
An anesthesia superbill can't stop at a procedure description and a diagnosis. It needs room for the anesthesia code, base-unit logic, time documentation, and concurrency modifiers such as -AA, -QK, or -QX when applicable.
If those elements are captured outside the primary superbill workflow, staff end up stitching together critical reimbursement logic from multiple places. That's how unit mismatches and modifier errors happen.
For anesthesia groups, the form should prompt for:
- Anesthesia code selection
- Start and stop time
- Concurrency detail
- Applicable modifier selection
- Supporting diagnosis and service date alignment
Mental health needs authorization-aware superbills
Behavioral health practices often use a basic coded receipt and assume that's enough. It usually isn't.
If you're billing services such as 90837, the superbill should also make room for session-specific compliance details and any authorization reference your team must track. Without that, the billing office ends up hunting across intake records, portals, and chart notes to confirm that the service was authorized and documented correctly.
A mental health superbill should reflect how the clinic gets paid, not just how the visit is described clinically.
Cardiology needs space for procedural relationships
Cardiology is where a generic superbill often creates downstream bundling headaches. A form that lists codes without enough procedural context leaves your billers exposed when payers question how services relate to one another.
If the encounter includes a procedure such as 93458, your form needs enough structure to distinguish the primary service from related diagnostics or supporting lines. That doesn't mean the superbill should become a full coding manual. It means the source document should preserve the clinical relationships that matter to reimbursement.
For groups working through interventional and diagnostic complexity, this guide to cardiology revenue cycle management is a useful operational reference.
Orthopedics needs global-period awareness
Orthopedic denials often come from timing and service separation problems. The superbill has to help your staff determine whether a service falls inside a global period or qualifies as distinct work that should be separately reported.
Line-level notes and modifier prompts are important. If the encounter involves multiple services and one may need modifier 59 to show that it was distinct, your form should make that review visible during charge capture, not after the denial comes back.
A specialty superbill should reduce coder interpretation, not require more of it.
What a specialty-ready template changes
A strong specialty template doesn't just collect data. It shapes behavior. It prompts the provider or staff member to capture the details most likely to affect adjudication for that specialty.
That's the difference between a superbill that documents a visit and one that protects revenue.
Best Practices for an Optimized Superbill Workflow
Most superbill problems aren't caused by one bad employee or one missed code. They're caused by a loose workflow. If the encounter moves from clinician to checkout to billing without a defined review process, errors show up downstream where they're harder to fix.
An optimized workflow makes the superbill predictable, reviewable, and specialty-aware from the moment the visit closes.

Build the workflow around the encounter, not around cleanup
The cleanest setups start inside the EHR and push structured visit data into a standardized superbill template. That reduces free-text dependence and lowers the chance that billing staff will have to interpret vague notes later.
The workflow should answer four questions before the document leaves the encounter stage:
- Was the rendering provider correctly identified
- Were all reportable services captured
- Do the diagnosis codes support each service line
- Were modifiers, POS, and specialty fields reviewed before release
If your current process relies on billers to catch everything after checkout, you're using the most expensive quality-control point in the workflow.
Standardize where you can and customize where you must
Practices need standardization, but not the kind that flattens specialty nuance. The best approach is a controlled core template with specialty-specific sections layered in.
That usually looks like this:
- Core universal fields: patient demographics, provider identifiers, date of service, CPT, ICD-10, POS, charges
- Specialty modules: anesthesia units and concurrency, behavioral health authorization fields, cardiology procedural grouping prompts, orthopedic global-period review prompts
- Review rules: line-item check for modifier necessity, diagnosis linkage, and missing identifiers
Audit the source, not just the denial
Many managers audit denials and think they're auditing billing quality. They aren't always the same thing.
You should also audit the superbill itself. Pull recent encounters and inspect whether the source document gave the billing team enough information to code, submit, and defend the claim cleanly. If not, fix the template or the handoff process.
A practical internal checklist should include:
- Completeness: Were all required fields present?
- Specificity: Did the diagnosis and procedure logic match the encounter?
- Readability: Could another staff member understand the service lines without asking the provider?
- Specialty relevance: Did the form prompt for the fields that matter for that service line?
Operational advice: If the billing office regularly sends messages back to providers for the same missing detail, that detail belongs on the superbill template.
Use technology to reduce memory-based billing
EHR-generated superbills are usually stronger than manually built ones when the template is configured correctly. Automation helps because it can carry forward demographics, provider data, and documented service details consistently.
But automation only helps if the rules are right. A poorly configured template just reproduces errors faster.
For managers refining workflow across departments, these revenue cycle management best practices provide a useful framework for aligning front office, clinical documentation, coding, and claims follow-up around cleaner source data.
Frequently Asked Questions About Superbills
Can a superbill replace a CMS-1500 claim form
No. A superbill isn't the formal claim submission. It's the encounter-level source document that contains the coded and administrative data needed to build or support the claim. In out-of-network situations, the patient may use it to seek reimbursement, but that doesn't make the superbill itself a CMS-1500.
What's the most common superbill mistake in physician practices
The most common mistake is using a generic template that doesn't force the team to capture the details that affect reimbursement. In primary care that may be diagnosis linkage and modifier review. In specialties, it's usually something more specific, such as anesthesia time units, authorization references, or global-period context.
Should providers or billers own the superbill review process
Both, but for different reasons. Providers should own clinical accuracy and service capture. Billing staff should own coding completeness, modifier review, and payer-facing readiness. If one side assumes the other is checking everything, gaps slip through.
How often should a practice update its superbill template
Update it whenever your code set, payer requirements, specialty mix, or workflow changes make the current version incomplete. At minimum, review the template on a routine schedule and after recurring denial patterns appear. If you're seeing the same clarification requests over and over, the template is already behind your operation.
If your practice is losing time to claim rework, denial follow-up, or specialty-specific billing complexity, Happy Billing helps tighten the process at the source. Their team works inside your existing EHR, combines agentic AI with human auditors, and supports high-stakes specialties that need cleaner superbills, faster claims, and tighter revenue cycle control.