Pain Management ICD 10: Boost Coding Accuracy 2026
Most practices treat pain management icd 10 as a compliance task. That is a cash flow mistake. The faster path to cleaner claims is often not a better appeal process, but a more precise diagnosis strategy on the front end, especially because chronic low back pain coded as M54.5 was the most prevalent condition in a large COPC study, affecting over 43,000 patients with a 75.6% positive predictive value according to the COPC ICD-10 analysis.
In pain medicine, diagnosis coding controls far more than claim form accuracy. It drives medical necessity, sequencing, modifier logic, prior authorization support, and whether your staff spends the next month posting payments or reworking denials.
Mastering Pain Management ICD 10 Coding for Maximum Reimbursement
Revenue leakage in pain practices rarely starts with the procedure code. It starts when the diagnosis line is vague, sequenced incorrectly, or disconnected from the treatment performed.
A claim for an epidural, trigger point injection, or longitudinal chronic pain management service can fail even when the CPT code is correct. If the ICD-10 set does not tell a payer exactly what type of pain, why it exists, and where it is located, the claim reads like an incomplete medical necessity argument.
Where cash flow breaks down
The failure points are usually operational, not theoretical:
- Sequencing errors: Staff place the underlying condition first when the encounter is for pain control.
- Insufficient specificity: Teams default to broad chronic pain language instead of tying the pain to trauma, surgery, neoplasm, syndrome, or anatomy.
- Weak diagnosis to procedure linkage: The billed CPT makes clinical sense, but the ICD-10 combination does not fully support it.
- Missing documentation triggers: Providers document symptoms casually, while coders need explicit chronicity, laterality, and etiology.
That pattern creates avoidable rework. Front-desk collections look fine, procedure volume looks strong, but aging climbs because too many claims require edits after submission.
What works in practice
The best-performing workflows standardize diagnosis selection before the charge ever drops.
Use this order:
- Define the pain category first. Is it acute, chronic, postprocedural, trauma-related, neoplasm-related, or chronic pain syndrome?
- Add the site or causative condition. Pair the pain code with the anatomical or etiologic diagnosis.
- Sequence based on encounter purpose. Pain management visits do not follow the same diagnosis order as every condition-management visit.
- Match modifiers and procedure logic. The diagnosis should support why distinct structures, bilateral work, or same-day services were necessary.
Tip: If your team audits denials by CPT only, you are looking too late in the process. Pain denials often start with diagnosis construction, not procedural entry.
A useful operating principle is simple. Build each claim as if the payer medical reviewer only sees the diagnosis list, the procedure line, and one paragraph of note text. If those three elements align, payment usually follows faster.
For a broader revenue strategy lens, the operational discipline behind cleaner submissions is similar to the approach outlined in maximizing insurance reimbursements.
The Core Framework G89 Pain Codes
The G89 category is the foundation of pain management coding. If your team uses it loosely, reimbursement slows down. If your team uses it with intent, claims become easier to defend.
Per the G89 coding overview and CMS-linked discussion of G3002 and G3003, the category includes G89.11-G89.18 for acute pain, G89.21-G89.29 for chronic pain, G89.3 for neoplasm-related pain, and G89.4 for chronic pain syndrome. The same source notes that CMS introduced G3002 and G3003 effective January 1, 2024, and those services require a precise G89 diagnosis to support medical necessity. It also confirms that pain may be the primary diagnosis when pain management is the reason for the encounter.
How to think about the G89 family
Do not treat G89 as a filler code. Treat it as the code family that answers the payer's first question: what kind of pain is being managed?
- G89.1x acute pain codes fit documented acute pain states when they are not classified elsewhere and the record supports the acute nature and cause.
- G89.2x chronic pain codes fit documented chronic pain conditions when chronicity is explicit in the note.
- G89.3 is reserved for neoplasm-related pain.
- G89.4 is for chronic pain syndrome, not pain that has lasted a long time.
The distinction matters because these codes shape payer interpretation of intensity, duration, complexity, and expected management path.
High-value examples
A few examples show where teams go wrong:
| Scenario | Better diagnosis approach | Why it pays better operationally |
|---|---|---|
| Ongoing pain after documented trauma | G89.21 plus the site-specific pain or injury-related code | This tells the payer the chronic pain has a defined cause |
| Chronic postsurgical pain visit | G89.28 plus the relevant postprocedural or site code | This avoids flattening a postprocedural case into generic chronic pain |
| Cancer pain management | G89.3 plus the neoplasm code | This ties pain treatment directly to the malignant condition |
| Complex persistent pain syndrome visit | G89.4 plus supporting site or related diagnosis when documented | This supports a broader management model than a vague chronic pain label |
Where G3002 and G3003 fit
Practices billing G3002 or G3003 should build diagnosis support carefully. Longitudinal chronic pain management codes invite payer scrutiny because they depend on a documented treatment plan, ongoing management, and a clear diagnosis rationale.
The diagnosis stack should answer four things:
- What pain category applies
- Whether the pain is acute or chronic
- Whether there is a known cause
- What anatomical site or related condition is involved
For pain groups handling injections, medication management, and recurring follow-up, the operational side of this work is tightly connected to pain management billing workflows.
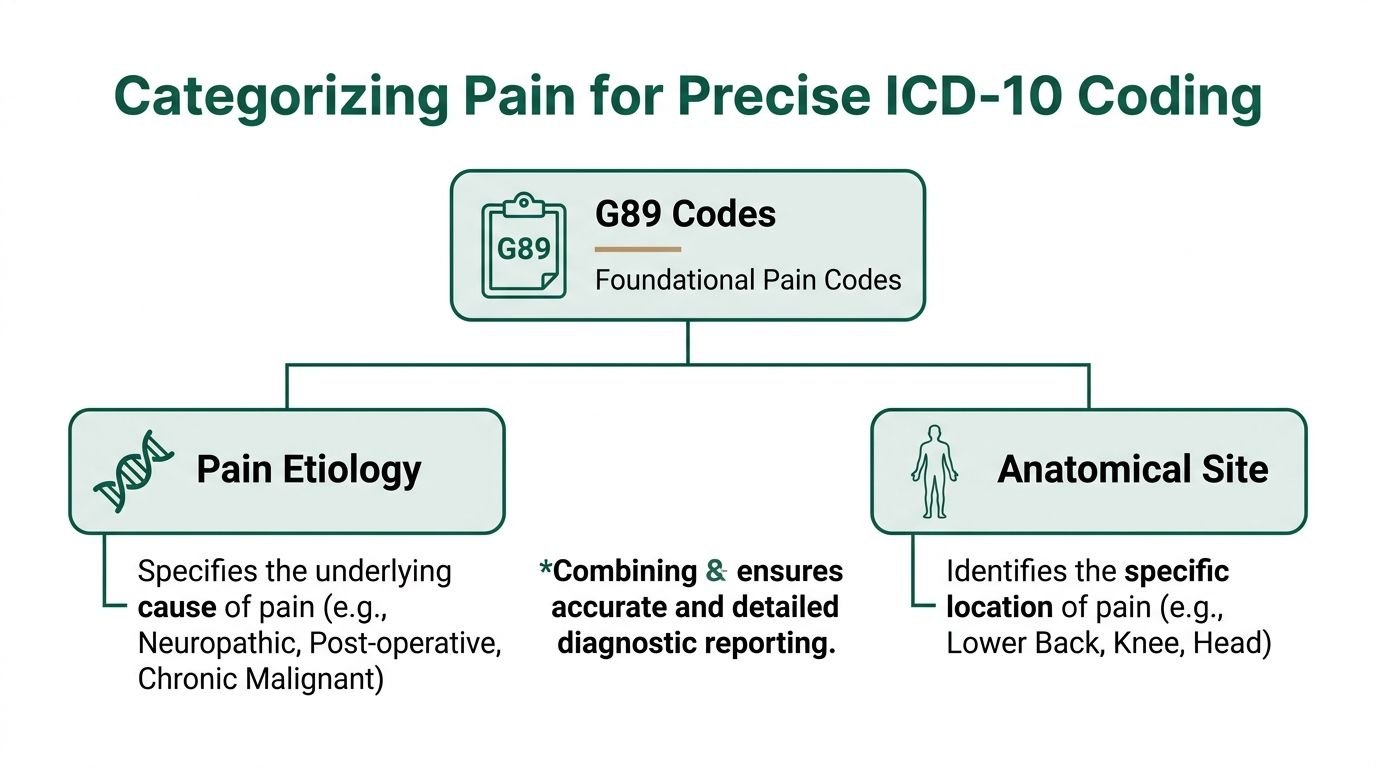
Categorizing Pain by Etiology and Site
Diagnosis selection in pain management directly affects cash flow. A vague diagnosis stack slows adjudication, triggers medical necessity edits, and turns routine claims into avoidable A/R.
High-performing pain practices code in two layers. The first layer identifies the pain category. The second ties that pain to the anatomical site or underlying cause documented in the note. That pairing gives the payer a reason to approve the visit, injection, ablation, or follow-up management service without sending the claim to manual review.
Start with the body system that supports the service
In production billing, pain claims usually fall into a few predictable diagnosis groups. Each group carries different documentation expectations and denial risk.
Musculoskeletal diagnoses
This category drives volume for many orthopedic, PM&R, and interventional pain groups. Low back pain, neck pain, myofascial pain, sacroiliac complaints, and joint-related pain appear on a large share of claims.
Examples include:
- M54.5 for low back pain when the record supports that diagnosis
- M54.2 for cervicalgia
- M54.31 and M54.32 for sciatica by laterality
- Other musculoskeletal codes when the physician identifies a more specific source of pain
Operationally, specificity matters. A lumbar epidural claim attached to a broad pain code may suspend for review. A claim tied to a diagnosis that matches the documented region, laterality, and clinical findings has a better chance of paying on first pass. That difference affects staff time, appeal volume, and days in A/R.
Neurologic and trauma-linked diagnoses
Neurologic support codes are often the difference between a clean claim and a denial on interventional pain services. If the note describes neuropathic pain, radicular symptoms, or nerve involvement, the diagnosis set should reflect that clinical picture rather than defaulting to a generic pain label.
Trauma-linked coding also needs discipline. If the provider connects the pain to a prior injury, the diagnosis stack should preserve that relationship. The same rule applies to postprocedural pain. Using a generic chronic pain code in a postsurgical case weakens the medical necessity story and can reduce the chance of first-pass payment.
The coding question is practical. Which diagnosis combination explains why the provider performed this service today, and will that logic survive payer edits and an audit?
Key takeaway: G89 defines the pain category. The companion code identifies the site or cause. Together, they create a cleaner path to payment than either code family can provide alone.
Codes to avoid unless documentation leaves no choice
Three diagnosis habits consistently create revenue leakage:
- R52 overuse: If the chart supports site, etiology, or chronicity, unspecified pain is too weak to carry many pain management claims.
- Standalone G89 use: A G89 code without a site or causative diagnosis often leaves the payer with an incomplete medical necessity rationale.
- Ignoring laterality: Right, left, and bilateral detail can affect whether the diagnosis supports the procedure billed.
I see this in audits every quarter. Practices rarely lose revenue because they failed to enter a diagnosis. They lose revenue because they entered a diagnosis set that was technically possible but financially weak.
Better categorization reduces manual reviews, lowers rebill volume, and helps claims hit the correct payer edit path on first submission. In pain management, that is not just cleaner coding. It is margin protection.
Sequencing Rules That Prevent Denials
One of the most expensive myths in pain billing is that the underlying condition should always be listed first. That is not how pain management icd 10 works when the encounter is primarily for pain control. Coder judgment must track the note, not habit, in these situations.
Per the AAPC discussion of official guidelines for pain code selection and sequencing, CMS guidelines require a G89 code to be listed first when the principal reason for the encounter is pain control. The same guidance gives a concrete example: G89.11 before M54.2 for acute neck pain due to trauma. That sequencing point is not cosmetic. It affects compliance and can draw audit attention when handled incorrectly.
When G89 belongs first
List the G89 code first when the visit is for:
- Pain control
- Pain management
- Chronic pain follow-up centered on analgesic or interventional management
- A procedure whose purpose is symptom control of the documented pain condition
In those situations, the G89 code establishes the principal purpose of the encounter. The site-specific or etiology code follows it.
Example logic:
| Encounter focus | Likely sequencing logic |
|---|---|
| Pain control for trauma-related neck pain | G89.11 first, then M54.2 |
| Chronic pain visit tied to trauma history | G89.21 first, then site-specific code |
| Cancer pain management | G89.3 first, then neoplasm code |
| Pain syndrome management | G89.4 first, then supporting site or related diagnosis |
When the underlying condition may lead
If the visit is not mainly for pain management, sequence can change. For example, if the provider is evaluating or treating the underlying condition itself rather than the pain-control aspect, the causative diagnosis may take priority.
This calls for coder judgment to track the note, not habit.
Review the opening line of the assessment. If the provider documents the reason for visit as pain control, chronic pain follow-up, analgesic management, injection for symptom relief, or similar language, sequencing should reflect that purpose.
The mistake that creates silent denials
Practices often train staff to “code the disease first.” That shortcut breaks in pain medicine.
A payer editing system may not issue a dramatic denial code that teaches your staff what happened. Instead, it may route the claim to review, suspend payment, or deny for diagnosis mismatch because the claim no longer reads as a pain-management encounter.
Audit view: Sequencing should follow clinical intent. If the chart says the patient came in for pain control, the diagnosis order must say the same thing.
The fastest fix is workflow-based. Require providers to open their note with a plain statement of visit purpose, such as pain control for chronic lumbar radiculopathy or management of chronic postprocedural pain. That single sentence gives coders a reliable sequencing anchor.
Common ICD-10 and CPT Code Combinations
Coding theory either survives contact with payer edits or fails in these situations. Pain claims get paid when the CPT and ICD-10 pairing tells one coherent story.
The safest pairings are the ones built from three aligned elements:
- Procedure performed
- Pain category
- Specific site or causative diagnosis
If one of those is missing, coders end up forcing claims through edits later.
ICD-10 and CPT pairing quick reference
| CPT Code / Procedure | Example ICD-10 Pairings (Primary + Secondary) |
|---|---|
| 62323 Epidural injection, lumbar or sacral | G89.29 + lumbar site/radicular diagnosis when documentation supports chronic pain management and the specific pain source |
| 64483 Transforaminal epidural injection, lumbar or sacral, single level | G89.21 + M54.31 or M54.32 when chronic trauma-related radicular pain is documented with laterality |
| 20552 Trigger point injection, 1 or 2 muscles | G89.29 or G89.4 + documented myofascial or anatomical pain diagnosis |
| 20553 Trigger point injection, 3 or more muscles | G89.4 + site-specific myofascial pain documentation with treated muscle groups clearly listed |
| 64490 Facet joint injection, cervical or thoracic, first level | G89 chronic or acute code as supported + cervical site diagnosis such as M54.2 when documentation shows pain management was the encounter purpose |
| 64493 Facet joint injection, lumbar or sacral, first level | G89 chronic pain code + lumbar pain diagnosis such as M54.5 when the note supports chronic low back pain management |
| G3002 Chronic pain management service | Precise G89 diagnosis plus the site or cause code documented in the treatment plan |
| G3003 Add-on chronic pain management service | Precise G89 diagnosis plus supporting secondary diagnosis tied to the ongoing management plan |
What these pairings are really doing
The ICD-10 pair is not there to “cover” the CPT. It is there to prove why that exact service was medically necessary on that date.
A few patterns matter:
- Injection codes need a diagnosis set that supports both pain type and target location.
- Trigger point services need muscle group documentation, not just “pain.”
- Facet and transforaminal services need anatomy that matches the procedural site.
- G3002 and G3003 require a diagnosis structure that supports longitudinal management, not one-off symptom language.
Common mismatch examples
Claims get unstable when teams submit combinations like:
- Trigger point injection with a broad pain diagnosis but no myofascial or site support
- Lumbar procedure with cervical diagnosis logic
- Chronic pain management service with no chronic G89 structure
- Radicular procedure without documentation of radicular symptoms or side
Those claims may not deny immediately. Some enter review, delay payment, and raise staff touch count. That is still revenue leakage.
For teams that regularly cross-check high-volume interventional services, a focused anesthesia and procedure coding reference helps standardize CPT selection before diagnosis linkage starts. This is especially useful alongside a practical anesthesia CPT code guide.
Essential Modifiers for Pain Management Procedures
Modifiers are not cleanup tools. In pain billing, they are payment logic.
A strong diagnosis set can still fail if the claim does not explain that the work was bilateral, performed at distinct structures, or separately reportable on the same day. Modifier discipline is where many financially healthy pain practices separate themselves from busy practices with bloated A/R.
Per the WebPT pain and injury ICD-10 billing guidance, -50 should be used for bilateral injections, XS for distinct structures in multi-procedure days, and 59 with a note if no X modifier fits. That guidance specifically ties modifier use to preventing multiple procedure reduction denials and supporting concurrency, including claims involving G3002/G3003.
Modifier 50 for bilateral work
Use -50 when the same eligible procedure is performed bilaterally and payer rules support bilateral reporting.
This matters in injection work because the operative note may clearly describe both sides, but payment software only sees one code line unless you report the bilateral nature correctly.
Checklist for bilateral reporting:
- Confirm payer preference: Some payers want one line with -50. Others may have line-item preferences.
- Match the note: The procedure note must state bilateral performance explicitly.
- Support anatomy: Diagnosis coding should not contradict bilateral treatment.
XS and 59 for distinct procedural work
Pain medicine often involves more than one service on the same date. That is where bundling edits become aggressive.
Use XS when procedures involve separate structures. A practical example is a gluteal trigger point injection and an L5-S1 steroid injection performed on the same day, when documentation supports that they addressed distinct anatomical targets.
Use 59 when no X modifier fits and the note clearly justifies separate reporting.
Practical rule: If you cannot explain the separation in one sentence from the op note, the modifier is probably not defensible.
Modifier risk areas that cost practices money
The most common operational failures are:
- Missing modifier on a valid second procedure
- Using 59 when XS is more precise
- Applying -50 without a bilateral note
- Forgetting that the diagnosis set should support the distinction claimed by the modifier
That last point matters. A modifier and diagnosis list should tell the same story. If you append XS for separate structures, the diagnoses and note should make those separate structures visible.
A useful internal education piece for coder training is a focused review of CPT modifier 59 and related distinct-service logic.
Documentation Requirements to Justify Medical Necessity
Auditors do not infer pain details. They code what the note says.
If the assessment says “back pain” and nothing more, the claim is weak before the biller touches it. If the assessment describes chronicity, site, laterality, cause, and treatment intent, coding becomes straightforward and denials drop.
What must appear in the note
For pain management icd 10, the provider note should document:
- Location: lumbar, cervical, thoracic, shoulder, gluteal, knee, pelvic, or other specific site
- Laterality: right, left, or bilateral when relevant
- Chronicity: acute, chronic, postprocedural, trauma-related, or neoplasm-related
- Pain character: sharp, dull, burning, radiating, aching, stabbing, or similar descriptors
- Cause or association: trauma, surgery, malignancy, syndrome, radiculopathy, myofascial pattern, neuralgia, and so on
- Reason for encounter: pain control, chronic pain follow-up, injection for symptom management, medication management
- Treatment plan: intervention chosen, surveillance, functional goals, and response when ongoing management is billed
Documentation phrases that help coders
Certain phrases make code selection easier because they answer coding questions directly.
Examples:
| Weak wording | Stronger wording |
|---|---|
| Back pain | Chronic right-sided low back pain with radicular symptoms |
| Neck pain after accident | Acute neck pain due to trauma with persistent cervical tenderness |
| Pain follow-up | Follow-up for chronic postprocedural pain management |
| Trigger point visit | Myofascial pain involving multiple muscle groups treated with trigger point injection |
G89 coding depends on explicit chronicity
If a physician means chronic pain, the note should say chronic pain. If the physician means pain syndrome, the note should support syndrome-level complexity. If the physician means postprocedural pain, that relationship should be spelled out.
This is also where routine postoperative discomfort must not be confused with reportable postprocedural pain coding.
Documentation tip: Start the assessment with one sentence that names the pain type, site, and reason for the encounter. Coders can build most of the claim from that line.
For G3002 and G3003, documentation should also show an ongoing management framework. A payer reviewing those services expects more than a symptom snapshot. The note should show why this is longitudinal pain care rather than a brief episodic complaint.
Payer Pitfalls and Proactive Denial Prevention
The fastest denial to predict in pain billing is the vague chronic pain denial. It usually starts with a claim built around G89.29 without enough site or etiology support.
According to the discussion of chronic pain ICD-10 coding and payer rejection patterns, nonspecific chronic pain codes like G89.29 are frequently rejected, and coding audits show this affects over 30% of chronic pain claims in major markets when payers want a stronger etiology link.

Three denial stories that repeat every week
The unspecified chronic pain denial
The provider documents a clear pain source, but the claim goes out with G89.29 alone or with weak support. The payer asks for specificity the chart already had.
Fix: Pair chronic pain with the site or causative diagnosis supported by the note. If the pain is due to trauma, surgery, neoplasm, or a syndrome, code that fact.
The bundling denial
Two valid procedures are performed on different structures the same day. The coder submits both but leaves off XS or uses 59 without note support.
Fix: Make the op note and modifier choice mirror each other. Distinct structures should be obvious from the documentation.
The sequencing denial
The visit is for pain control, but the claim leads with the underlying condition. The payer edits it as a condition-management visit rather than a pain-management encounter.
Fix: Put the correct G89 code first when pain control is the principal reason for the visit.
A front-end review that saves rework
Before submission, require a focused check for:
- Diagnosis specificity
- Sequencing logic
- Modifier support
- Procedure to diagnosis alignment
- Documentation of laterality and chronicity
- Global period or postoperative context
A disciplined denial prevention workflow is far cheaper than a strong appeals team. The best appeal is the one your staff never has to write.
For practices tightening this process, a structured medical billing denial management approach helps convert payer patterns into pre-bill edits.
Frequently Asked Questions for Pain Management Coding
When should G89 be billed as the primary diagnosis
Bill a G89 code first when the principal reason for the encounter is pain control or pain management. If the visit is centered on managing the underlying condition itself rather than the pain-control aspect, sequencing can differ. The chart needs to make the visit purpose obvious.
Is G89.29 enough for most chronic pain claims
Usually no. Broad chronic pain coding is a common source of denials when the record supports a more specific story. If the provider documents trauma, postprocedural status, neoplasm-related pain, syndrome, radicular symptoms, or a defined anatomical site, build the claim around that specificity.
How should same-day E/M and procedure services be handled in pain visits
Handle them carefully and only when the documentation supports a separately identifiable evaluation beyond the usual pre-procedure work. The E/M note must stand on its own. If your procedure claim also involves multiple structures or bilateral work, make sure the diagnosis list, modifiers, and procedural note all tell the same story.
What documentation matters most for chronic pain management services like G3002 and G3003
The note should establish that the pain is chronic, identify the pain type and site, and show an ongoing treatment plan. Functional goals, surveillance, and the management rationale matter. A brief symptom note without a structured chronic pain plan creates medical necessity risk.
Practices that want faster payment on pain claims usually do not need more billing noise. They need tighter diagnosis construction, cleaner sequencing, and audit-grade modifier logic. Happy Billing helps specialty groups build that discipline into daily operations so claims move cleaner, denials fall earlier in the workflow, and cash reaches the bank faster.