Master Out of Network Billing: Boost Revenue, Reduce Denials
Out of network billing can help a practice protect margin, but only if you run it like a controlled revenue strategy instead of a loose exception process. If your higher-fee cases are sitting in A/R, getting underpaid, or turning into repeated appeals, the issue usually isn't whether you're out of network. It's whether your workflow, documentation, and negotiation discipline are strong enough to support it.
Most practice owners feel this when a handful of claims carry a disproportionate revenue impact. One underpaid anesthesia case, one delayed assistant surgeon claim, or one disputed behavioral health episode can distort monthly cash flow fast. That's why out of network billing belongs in the same conversation as denial rate, payment lag, and A/R aging, not just compliance.
What Out of Network Billing Means for Your Practice Revenue
A practice is dealing with out of network billing when it provides services without a contracted reimbursement rate from the patient's health plan. From the owner's side, that creates two very different possibilities. You may collect more per case than an in-network fee schedule would allow, or you may spend months fighting for payment while cash stalls.
I see this most often in specialty groups that are clinically strong but operationally inconsistent. The physician assumes the claim is valuable because the service was complex. The payer sees missing records, unclear consent, or a claim that wasn't built to survive review. Revenue then moves from expected cash to aged receivable.
That tension is one reason federal regulation tightened around this area. A major U.S. study found that among 13,579,006 emergency department visits between 2010 and 2016, the share with an out-of-network bill rose from 32.3% to 42.8%, while mean potential patient liability increased from $220 to $628 in 2018 dollars, according to JAMA Internal Medicine's analysis of surprise billing trends.
Why owners feel the pain in A R first
Out of network claims usually don't fail in one dramatic moment. They fail in stages:
- Verification breaks early: Staff confirms active coverage but never confirms out-of-network benefits or whether the service falls into a protected category.
- Financial documentation is thin: The practice can prove care was rendered, but not that disclosures, estimates, or consent were handled correctly.
- Claim construction is weak: Procedure coding may be accurate, but the submission lacks records that support complexity, medical necessity, or payer-specific claim expectations.
- Follow-up is passive: Teams wait for payer movement instead of managing deadlines and escalation points.
Practical rule: If your largest out of network claims age the longest, you don't have a pricing problem first. You have a process problem.
For physician owners, the strategic question isn't whether out of network billing is good or bad. It's whether your practice can reliably turn those claims into cash without creating compliance exposure or bloating staff workload.
A useful place to pressure-test that is your broader medical billing revenue strategy. If core RCM discipline is weak, out of network billing magnifies every weakness already in the system.
What it is not
It's not just a patient billing issue. It affects:
| Practice area | What changes financially |
|---|---|
| Fee setting | You have more pricing flexibility, but less payment certainty |
| Cash timing | Payment often slows when no contract rate governs the claim |
| Denial management | Underpayments and disputes require stronger back-end work |
| Contract leverage | Out-of-network capability can influence payer negotiations |
That's why owners should treat out of network billing as a margin lever with compliance consequences, not a side process the billing team can improvise.
The Regulatory Landscape of Surprise and OON Billing
The biggest mistake I see is treating the No Surprises Act like a legal memo instead of an operating rule. For practice owners, the law matters because it dictates which out of network claims can be billed how, when payment should arrive, and how fast your team must act when a payer underpays.
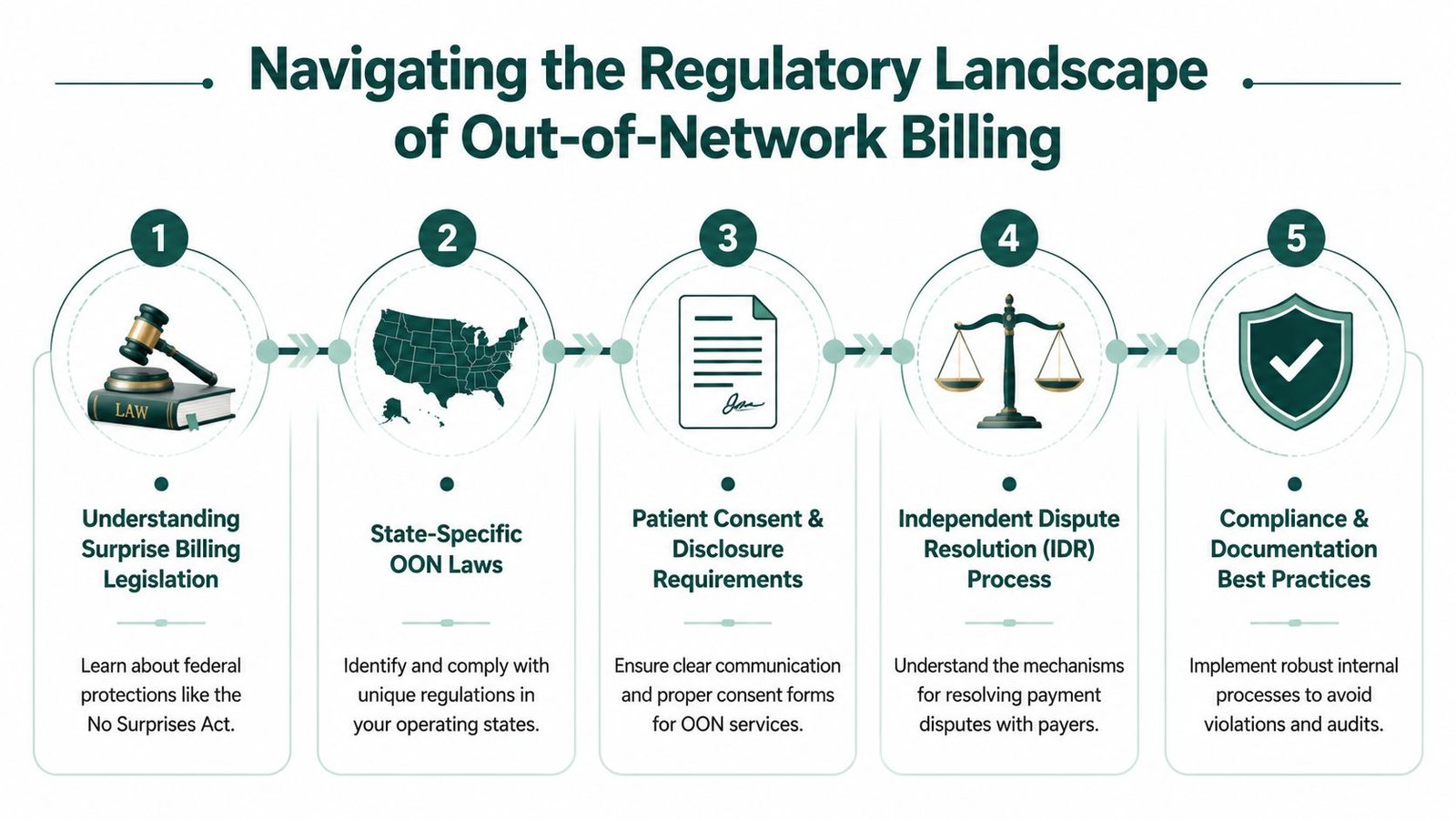
Under the federal framework, reimbursement disputes for emergency services, out-of-network care at in-network facilities, and certain ambulance claims move through open negotiation and then Independent Dispute Resolution. The operational timing matters more than most owners realize. Under the No Surprises Act, a payer has 30 days to issue an initial payment or denial for a clean out-of-network claim. The provider then has 30 business days to initiate a 30-day open negotiation period. If unresolved, the matter can proceed to IDR, and the same provider-plan pair can't re-arbitrate the same item or service for 90 days, as outlined in this overview of the federal IDR timeline.
What falls into the protected category
For owners, the practical issue is simple. Some services that used to create balance-bill opportunity now fall into a tightly regulated reimbursement track. That changes both cash expectations and staff responsibilities.
Three areas need management attention:
- Emergency claims: These are often the highest-risk from a dispute standpoint because payment may arrive without any meaningful alignment to your charge structure.
- Facility-based specialty care: If your clinicians practice at in-network facilities, certain services can trigger surprise billing rules even when your group itself is out of network.
- Communication workflows: Consent, disclosure, and estimate handling are no longer optional administrative tasks. They are revenue protection tasks.
A lot of practices also overlook the communication channel itself. When your front office or financial counseling team needs to review estimates, disclosures, or payer-facing documentation with remote patients or off-site clinicians, secure platforms matter. For teams tightening documentation discipline, AONMeetings for compliant calls is a useful reference point for HIPAA-conscious communication workflows.
Deadlines are revenue controls
Owners often focus on whether an appeal is winnable. The better question is whether the claim was managed on time. A clean claim submitted late, a negotiation opened late, or documentation assembled after the dispute window closes can all turn collectible revenue into write-off pressure.
Missing a deadline in out of network billing is not a clerical miss. It's a cash loss.
This is also where prior authorization discipline intersects with out-of-network performance. A practice that already struggles with medical necessity edits, payer-specific rules, or missing approvals will usually struggle more once disputes start. If your internal controls are loose, tightening your prior authorization workflow in healthcare operations is often part of fixing OON leakage.
What doesn't work
What fails most often is relying on generic appeal letters, scattered spreadsheets, and staff memory. The law rewards organized practices. It punishes reactive ones.
The owners who do best here know, for each disputed claim, who owns the file, what date triggered the next step, what documentation supports the rate, and whether the claim is worth escalating.
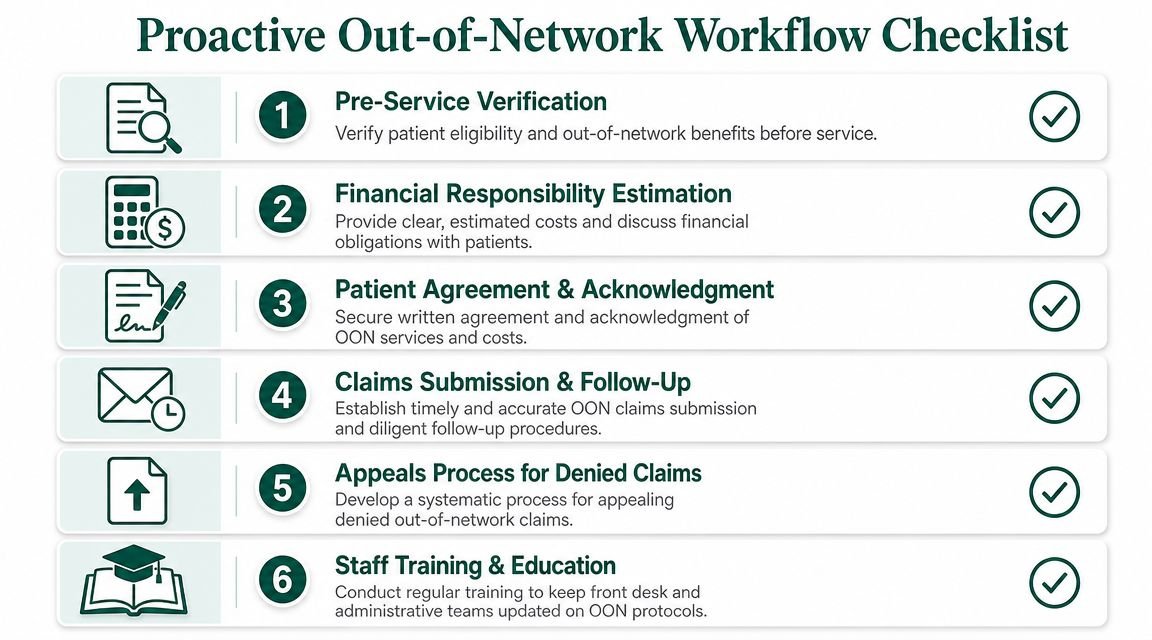
Building a Proactive Out of Network Workflow
Most out of network losses happen before the claim is ever submitted. The front desk misses the benefit nuance. Financial counseling is rushed. The chart supports care, but not the reimbursement argument. Then the back office inherits a weak file and tries to rescue it.
A proactive workflow fixes that upstream.
A landmark commercial-insurance study found that 22% of emergency visits to in-network hospitals involved out-of-network physicians, and those physicians charged an average of 637% of Medicare for identical services. That gap is one reason consent, estimation, and payment workflows became such a focal point in regulation, as described in the Yale policy analysis on surprise out-of-network billing.
The front-end checklist that protects cash
A strong OON process starts before the encounter. Not at claim submission.
Verify more than active coverage
Staff should confirm whether the plan includes out-of-network benefits, whether the service location changes the billing rules, and whether the case may fall under surprise-billing protections. For scheduled services, this needs to happen early enough to adjust scheduling, referrals, or financial expectations.Build the estimate conversation into intake
Financial responsibility shouldn't be discussed as a vague possibility. It should be addressed as a structured conversation with documented acknowledgment. If the service is recurring, like psychotherapy using CPT 90837, estimate discipline matters even more because one misunderstanding can repeat across multiple dates of service.Use service-specific consent language
Generic financial policies don't hold up well in high-friction claims. Procedure-specific or scenario-specific acknowledgment is stronger, especially when the service is elective or scheduled and your team is managing a waiver process where permitted.
The practice that explains money clearly before the visit usually spends less time defending the bill after the visit.
Clean claim means complete claim
For out of network billing, a clean claim is not just a claim without typos. It's a claim that arrives with enough substance to support payment.
That usually means your team has aligned these pieces:
- Coding accuracy: Correct CPT and HCPCS reporting, applicable modifiers, and diagnosis linkage
- Clinical support: Notes that show complexity, medical necessity, and provider role
- Administrative backup: Eligibility findings, authorization details if applicable, estimate records, and signed documentation
- Payer-specific routing: Correct claim form, attachments, and submission path
A few examples matter to owners because they change dollars fast. In anesthesia, modifier selection like QK can affect how the payer interprets medical direction and payment responsibility. In surgery, assistant surgeon modifiers such as 80, 81, or AS can determine whether the payer recognizes the role at all. In office-based specialties, modifier 25 can protect a separately identifiable E/M service, but weak documentation turns that into an easy denial target.
The underlying issue isn't coding trivia. It's whether the revenue for a complex encounter survives payer review.
Train the workflow, not just the biller
Out of network billing succeeds when scheduling, intake, financial counseling, coding, and follow-up act like one system. Most practices need written playbooks, payer-specific call scripts, and a standard packet for disputed claims. If you're trying to reduce handoff failures, tightening revenue cycle workflow improvements across front and back office teams usually produces more value than adding another person to collections.
Advanced Negotiation and Appeals for OON Claims
If your team accepts the payer's first out-of-network payment as the practical rate, you're giving up the core bargaining power of OON billing. The payer's initial determination is often just the opening position.
The right response is not to appeal everything. It's to triage aggressively. Some claims deserve immediate closure. Others deserve open negotiation. A smaller set deserves escalation because the documentation, service complexity, and economics support the effort.
What a serious negotiation file looks like
Payers usually respond to one of three things. Specificity, consistency, and proof.
A strong file includes:
- Procedure-level support: The exact CPT or HCPCS line under dispute, any relevant modifiers, and the clinical circumstances that made the service more complex than a routine case.
- Provider qualifications: Training, subspecialty expertise, or unusual case demands when that context helps explain value.
- Medical necessity record: Operative notes, anesthesia records, imaging interpretation detail, or longitudinal behavioral documentation, depending on specialty.
- Comparable payment logic: Not a generic demand letter. A rationale for why the initial payment doesn't reasonably reflect the service.
For example, an anesthesia group disputing payment on a medically directed case should not send a blanket appeal. It should show the reported anesthesia code, time documentation, provider roles, and the modifier structure that supports payment. A cardiology practice disputing imaging or procedural underpayment should anchor its argument in the chart, not frustration with the payer.
When to negotiate and when to stop
I advise owners to separate pride from economics. Some claims are annoying but not material. Others set a precedent with the payer or represent enough dollars to justify escalation.
Use a simple internal decision screen:
| Claim status | Best move |
|---|---|
| Minor variance, weak documentation | Close and repair the workflow |
| Material underpayment, strong file | Open negotiation quickly |
| Repeated low payment pattern on the same service line | Track and escalate systematically |
| Documentation gaps that cannot be cured | Don't throw labor at a losing dispute |
Owner view: The goal isn't to win arguments. It's to collect more net revenue with less staff drag.
Appeals work better when the practice learns from each loss
A denied or underpaid OON claim should feed back into the workflow. If the payer keeps challenging assistant surgeon necessity, tighten the operative documentation. If psychotherapy claims keep stalling over authorization history or plan terms, fix eligibility scripting before the next visit cycle. If facility-based specialty claims keep failing because disclosures are inconsistent, move that process out of ad hoc email and into intake.
Many groups benefit from a more disciplined denied insurance claim appeal process. The value isn't just recovering one claim. It's identifying which errors are causing repeat leakage and shutting them down.
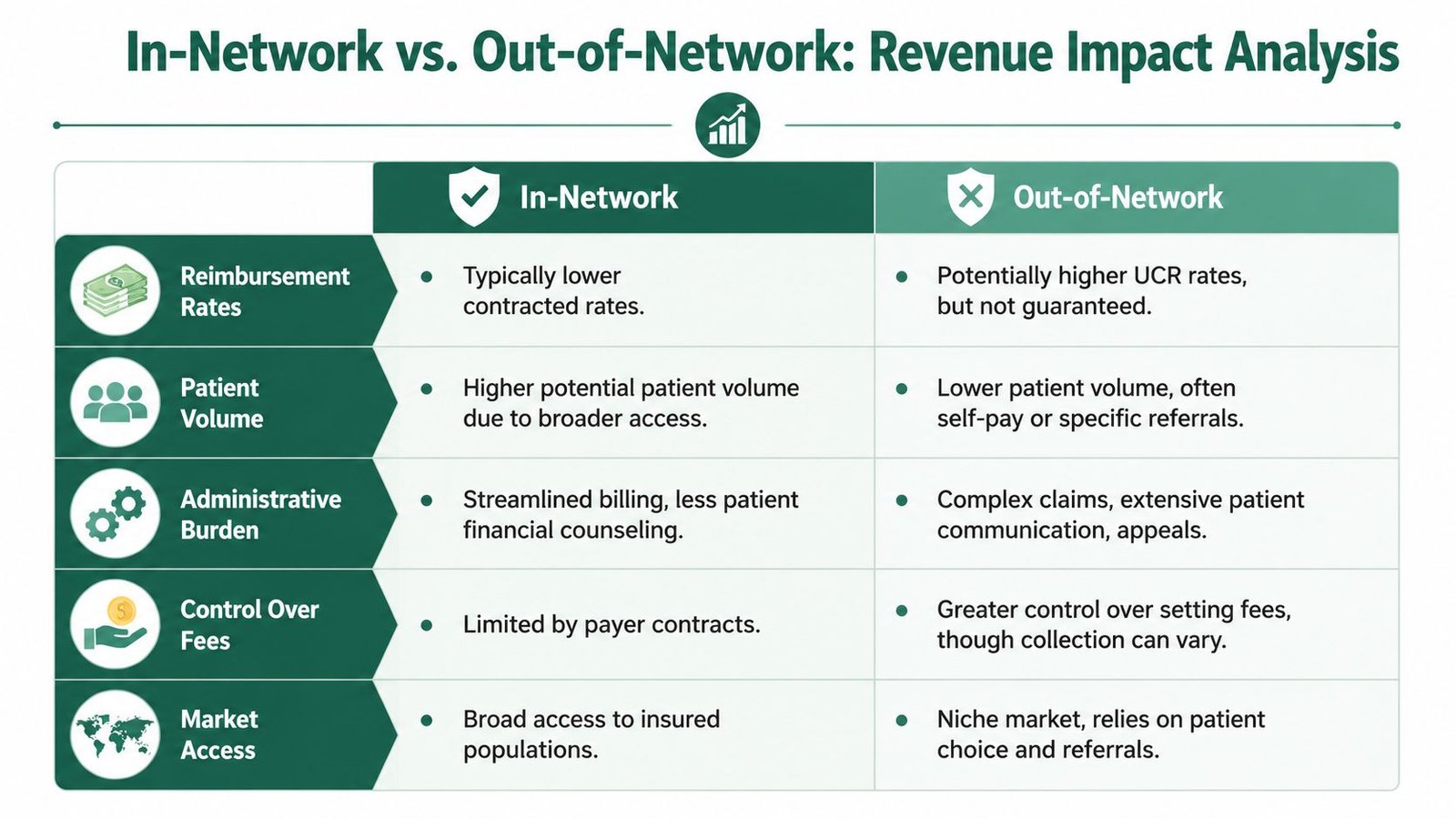
Modeling the Revenue Impact of Your Network Status
The strategic question isn't “Can we bill out of network?” It's “For this payer, in this market, does being out of network improve practice-level economics after friction, delay, and collection risk?”
That requires a model. Not a guess.
A Health Affairs analysis found that if specialists could not bill out of network, their payments from private insurance would fall by an estimated 13.4%, showing that OON capability affects reimbursement power well beyond a single claim, according to Health Affairs research on physician billing leverage.
The four inputs that matter most
Owners should compare network scenarios using these variables:
Reimbursement stability
In-network rates are lower but predictable. Out-of-network billing may offer stronger gross yield on selected services, but payment timing and final allowed amounts vary more.
Volume effect
Some payers drive referral access and patient acquisition. Going out of network may improve yield per case while shrinking total case volume. In some specialties, that works. In others, it damages downstream procedure flow.
Administrative cost
Out-of-network revenue is never just reimbursement. It comes with intake labor, estimate handling, payer calls, disputes, and appeal work. If your team is already strained, those hidden costs are real.
Negotiation leverage
A group that can credibly stay out of network has more bargaining power in contract discussions than one that must sign any rate offered. That doesn't mean every payer should remain OON. It means owners should negotiate from modeled economics, not fear.
A practical comparison
Use a worksheet that asks:
- What are the most common CPT codes by payer?
- Which of those services produce the largest margin gap between in-network and OON outcomes?
- How long do OON claims sit before payment?
- Which payer repeatedly underpays despite staff effort?
- Does this payer's patient volume justify the lower contracted rate?
A payer contract is only valuable if the predictability it creates is worth the revenue it gives away.
For some physician groups, the right answer is mixed strategy. Stay in network where patient access matters and contracted rates are workable. Remain out of network where the payer's fee schedule is structurally weak or where specialty bargaining power is strong enough to support better economics.
That decision gets sharper when you look at service lines separately rather than judging the whole payer relationship as one block.
Specialty-Specific Out of Network Billing Guidance
Out of network billing isn't managed the same way across specialties. The revenue risks are different, the coding pressure points are different, and the payer objections are different. Owners need specialty-specific controls, not generic OON policy binders.

One Health Affairs study found that 11.8% of anesthesiology claims and 11.3% of assistant surgeon claims at in-network hospitals were billed out of network, which is one reason these specialties face disproportionate scrutiny in OON payment disputes, based on this Health Affairs specialty billing analysis.
Anesthesiology and facility-based groups
Anesthesia groups lose money when time, concurrency, and medical direction details don't align. If you're billing medically directed cases, modifiers such as QK, QX, and AA aren't just coding mechanics. They affect whether the payer recognizes the provider arrangement and pays correctly.
For owner-operators, the key is documentation integrity. Your anesthesia record, start-stop times, provider assignment, and supervision narrative must support the exact claim structure. If those pieces don't line up, the payer has an easy path to downcode or deny.
Mental health and recurring visit models
Behavioral health groups face a different issue. The challenge isn't usually one giant claim. It's repeated friction across recurring visits. For CPT 90837, weak benefit verification and inconsistent authorization tracking can create a steady stream of avoidable denials.
That's why many practice owners in this space need stronger systems around eligibility, visit limits, and pre-service financial communication. A useful reference for that operational side is mental health revenue cycle management for recurring claims.
Cardiology and surgical specialties
Cardiology practices often run into trouble on diagnostic testing, interventional work, and assistant surgeon billing. If an assistant role is billed with 80, 81, or AS, the operative report must clearly support why that role was necessary. If it doesn't, payment arguments get weak fast.
Orthopedics has a parallel problem. The claim may be technically accurate, but global period logic, modifier use like 24, 25, 57, 58, 78, or 79, and implant-related documentation all influence whether the payer accepts separate payment or bundles more than it should.
Specialty practices don't lose OON revenue because they lack good clinicians. They lose it because specialty-specific billing rules aren't embedded into daily operations.
For owners comparing options by specialty, it helps to review workflows built around each service line's payer friction. The best place to start is the broader set of specialty billing solutions aligned to how different physician groups get paid.
FAQs From Practice Owners on Out of Network Billing
Can my practice still see out of network patients profitably
Yes, but profitability depends on discipline before and after the visit. Practices do well when they verify benefits carefully, explain financial responsibility clearly, submit a fully supported claim, and escalate underpayments on time. They struggle when out of network visits are treated as exceptions with no standard workflow.
When is out of network billing worth the administrative burden
It's worth it when the expected reimbursement justifies the extra intake work, documentation burden, and payer follow-up. Owners should review this by payer and by service line. High-value procedural claims may support the effort. Lower-dollar visits often don't unless the workflow is highly efficient.
What should I watch first if OON claims are hurting cash flow
Start with three pressure points:
- Aging concentration: Identify whether a small group of OON claims is driving a large share of old A/R.
- Underpayment patterns: Look for repeated low payments on the same CPT codes or the same payer.
- Front-end misses: Audit benefit checks, financial acknowledgments, and supporting documentation on disputed claims.
If the same issues keep repeating, the problem is operational, not random.
Should we manage complex OON claims in house or outsource them
That depends on whether your current team can handle payer-specific rules, dispute deadlines, specialty documentation, and consistent follow-up without neglecting core in-network collections. If OON claims are aging, appeals are inconsistent, or physician time is being pulled into billing disputes, it's usually time to reassess the model.
Many owners use that moment to request an outside review of their denial trends, workflow gaps, and payer behavior. A practical next step is a free revenue cycle audit for out-of-network claim leakage so you can see whether the problem is front-end process, payer underpayment, or back-end follow-through.
If your practice is losing time and margin on out of network billing, Happy Billing can evaluate where the revenue is stalling and what to fix first. We help specialty practices tighten front-end controls, reduce denial drag, and recover more from difficult claims without forcing an EHR migration or adding more work to physicians.