Expert Rehab Medical Billing Services: A Practice Guide
Rehab medical billing services are specialized revenue cycle management solutions designed for physical, occupational, and speech therapy practices. Unlike generic billing, they focus on navigating complex rehab-specific coding, authorization, and payer rules to reduce claim denials and accelerate cash flow.
If you're running a therapy practice right now, you probably don't need another definition. You need to know why claims that look clean at checkout still come back unpaid, why visit authorizations expire mid-plan of care, and why a co-treated session can create reimbursement leakage even when the clinical work was appropriate. Across healthcare, providers lose $125 billion annually to billing-related issues, and HIPAA violations can bring fines ranging from $100 to $50,000 depending on severity, according to SuperStaff's review of rehab billing outsourcing.
For a PT, OT, or SLP owner, that isn't abstract industry noise. It shows up as longer A/R, more staff touchpoints per claim, preventable write-offs, and clinicians getting pulled into documentation cleanup after the fact.
What Are Rehab Medical Billing Services
Monday morning. Your front desk checked the patient in, the therapist documented a co-treatment, and the claim still gets underpaid 30 days later because the payer applied multiple procedure reduction differently than your team expected. In 2024 and 2025, that kind of miss is common in PT, OT, and SLP billing. A rehab billing service exists to catch those payer-specific rules before they turn into avoidable A/R.
Rehab medical billing services are revenue cycle operations built for therapy practices with recurring visits, time-based codes, plan-of-care requirements, authorization limits, and discipline-specific payer edits. The work goes beyond claim filing. It includes benefit checks, visit tracking, authorization management, coding review, documentation review, charge scrubbing, payment posting, denial follow-up, and patient balance resolution, all done with therapy rules in mind.
The difference shows up fastest in interdisciplinary care. A general billing team may submit 97110, 97112, 97530, 92507, or 97165 correctly at a basic level and still miss how a payer wants co-treatment documented, how units should be split between disciplines, whether a therapy assistant modifier changes payment, or when one service falls into a postoperative global package and should not be billed separately. In 2024 and 2025, those details matter more because payers have kept tightening edits around PT, OT, and SLP sessions billed on the same date of service. If the billing team does not know that payer's reduction logic and documentation standard, the clinic gives up revenue through underpayments, not just denials.
That is why rehab billing became its own specialty. Therapy claims fail for reasons that generic physician-office workflows often miss. The note may support treatment, but not support the total timed minutes billed. The authorization may approve OT visits, but not PT on the same case. The CPT coding may be technically valid, but the payer may reduce the practice-expense portion of the second procedure or bundle services performed during a global period after surgery.
A qualified rehab billing service handles those therapy-specific failure points in real time. It reviews modifier usage such as 59, XE, GP, GO, GN, CQ, and CO where applicable. It checks whether the plan of care, progress note timing, and certification support payment. It compares posted reimbursement against contract expectations so underpayments do not get written off as normal variance.
Practice owners should expect three concrete outcomes:
- Fewer claims held or reduced because documentation, units, and modifiers were wrong for the payer's therapy rules
- Faster identification of authorization and visit-limit problems before treatment is delivered
- Better recovery of underpaid interdisciplinary claims, especially where PT, OT, and SLP overlap on the same day
For a plain-English baseline, this overview of what medical billers do in day-to-day revenue cycle work is useful. In rehab, every one of those tasks has to be configured around therapy coding, payer edits, and current interdisciplinary billing rules rather than generic medical billing assumptions.
The Core Scope of Services Explained
A rehab billing service manages the revenue cycle from the first insurance check to the last appeal. For a therapy practice, that scope has to be wider than claim submission because revenue leaks start before treatment and often continue after the payer issues a partial payment.
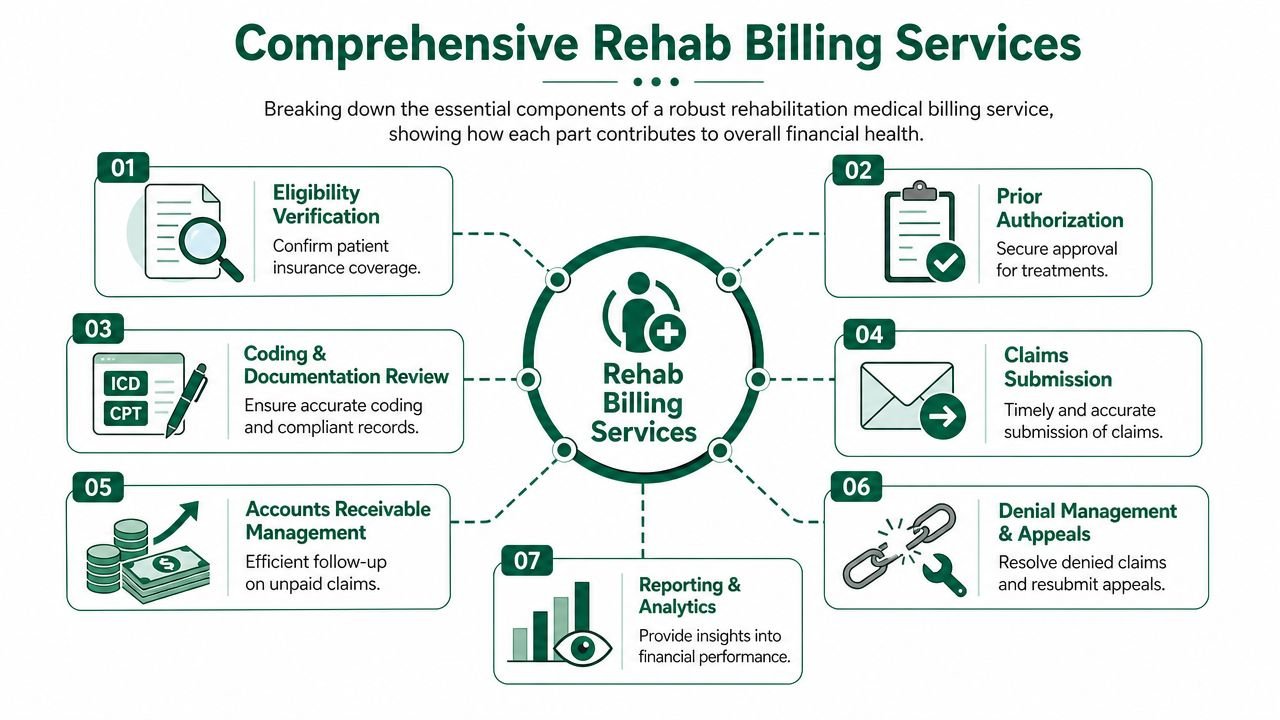
Front-end controls that stop bad revenue
The first job is to keep nonpayable visits off the schedule or, at minimum, flag them before staff deliver care.
- Eligibility verification: Confirm active coverage, therapy benefits, copay, deductible status, visit caps, and whether the plan tracks limits by discipline or by a combined rehab benefit.
- Prior authorization tracking: Monitor start and end dates, approved CPT ranges, units, and discipline-specific approvals. A payer may authorize OT and deny PT on the same case, or approve evaluations but require a separate request for ongoing treatment.
- Credentialing and contracting support: Keep payer enrollment current, match rendering and group NPIs correctly, and verify contract status before claims go out under the wrong entity.
For clinics that want a practical example of what this should include, a physical therapy billing service built around therapy-specific workflows should address benefit checks, authorization controls, coding review, denial work, and payment variance review as one connected process.
Mid-cycle work that protects reimbursement
Mid-cycle work is where specialized rehab billing earns its fee. Generic billers can transmit a clean 837. They often miss the therapy logic that determines whether the claim gets paid correctly.
A qualified team reviews common rehab codes such as 97110, 97112, 97116, 97140, and 97530 with the discipline modifiers GP, GO, and GN tied to the actual service line. It also checks whether modifier 59 or XE is defensible from the note, not just technically available in the software. If documentation does not clearly separate manual therapy from therapeutic exercise, billing both services on the same date invites bundling or post-payment review.
The 2024 to 2025 rule changes around interdisciplinary rehab make this mid-cycle review more important. Some payers are tightening edits on same-day PT, OT, and SLP billing, especially on co-treated sessions, and applying multiple procedure payment reductions more aggressively when timed codes overlap across disciplines. Others are scrutinizing services delivered during post-surgical global periods to determine whether therapy should pay separately, reduce, or deny based on diagnosis linkage and postoperative rules. A rehab billing service has to configure payer-specific edits for those scenarios before the claim drops, not after denial volume rises.
Operational test: Ask the billing vendor how it handles same-day PT and OT timed codes under payer-specific multiple procedure reduction rules, and how it flags therapy performed during a surgical global period. If the answer stays at "we have experienced coders," keep asking.
Back-end recovery that keeps A/R from aging out
A therapy claim still needs active management after submission. Payment posting alone does not protect margin.
| Service area | What it prevents |
|---|---|
| Payment posting | Underpayments, unapplied balances, and missed secondary billing |
| Denial management | Repeat denials from the same authorization, coding, or modifier issue |
| A/R follow-up | Claims sitting in payer queues until timely filing or appeal windows close |
| Patient balance workflows | Slow collection after insurance leaves deductible, coinsurance, or noncovered amounts |
| Reporting | Missed trends in payer reductions, therapist documentation risk, and staff handoff errors |
I usually tell owners to look for one simple sign of weakness. If the billing company can tell you how many claims were submitted but cannot explain why reimbursed units per visit dropped for one payer after a rule update, the service is too narrow for outpatient rehab.
For therapy practices, the core scope is operational control across the full claim lifecycle. That includes front-end verification, mid-cycle coding and payer rule review, and back-end recovery on denials, underpayments, multiple procedure reductions, and interdisciplinary claims that require more than generic medical billing habits.
Navigating Rehab-Specific Billing Challenges
Rehab billing breaks down when a team applies generic physician-office habits to therapy claims. Therapy reimbursement depends on time, medical necessity, visit sequencing, discipline distinctions, and payer edits that are often more aggressive than owners realize.

The mistakes that quietly drain therapy revenue
Take the 8-Minute Rule. If units are calculated loosely or documented inconsistently, the clinic may underbill legitimate time or overbill units that won't hold up under review. Owners usually feel this as shrinking reimbursement per visit, not as a dramatic denial spike. The claim gets paid, but not correctly.
Then there are medical necessity issues. A payer may accept an initial evaluation and early visits, then start questioning whether continued care is supported by the progress note, plan of care, or functional documentation. That creates a harder denial to overturn because the problem isn't just clerical. It's clinical support tied to payment.
Rehab practices also deal with modifier logic that can look simple and still go wrong. Discipline modifiers such as GP, GO, and GN have to align with the rendering service. Distinct procedural modifiers such as -59 need clear separation in the record. If the chart doesn't prove separate work, the modifier won't save the claim.
The 2024 and 2025 issue owners should press vendors on
The most under-discussed risk right now is how billing teams handle interdisciplinary therapy sessions under updated payer scrutiny around global periods and multiple procedure reduction logic. Existing content across the market stays vague here, but the actual problem is straightforward: when PT, OT, and SLP services overlap in one session or one date of service, payer edits increasingly flag claims when coding, timing, and documentation don't line up with the payer's automation rules.
That matters because many owners assume a biller can "know rehab." That's not enough. You need a team that can explain how it handles same-day overlap, how it distinguishes co-treatment from separate timed services, and how it adjusts claim construction when payer rules apply reductions or trigger algorithmic review. This issue is serious enough that we direct therapy groups to our physical therapy billing specialty guidance when they're trying to benchmark whether their current process is built for therapy-specific denials.
If a billing vendor can't walk you through PT and OT overlap on a real claim example, they probably aren't managing the risk. They're waiting to see what the payer does.
Where generic vendors usually fail
Three patterns show up repeatedly:
- They don't map documentation to payer edits: The claim may be technically complete but still unsupported.
- They rely on resubmission instead of prevention: That inflates A/R and staff time.
- They can't explain payer-specific rehab rules: Which means leadership has no way to judge whether denials are avoidable.
The rehab owner doesn't need a lecture on coding theory. You need a billing operation that understands which claim details are most likely to cost you money on the first pass.
Key Performance Indicators and Industry Benchmarks
Most owners know when billing feels broken. Fewer track it in a way that isolates where revenue is leaking. The right KPI dashboard makes your billing vendor easier to manage because it turns "we're having some denials" into measurable operational signals.
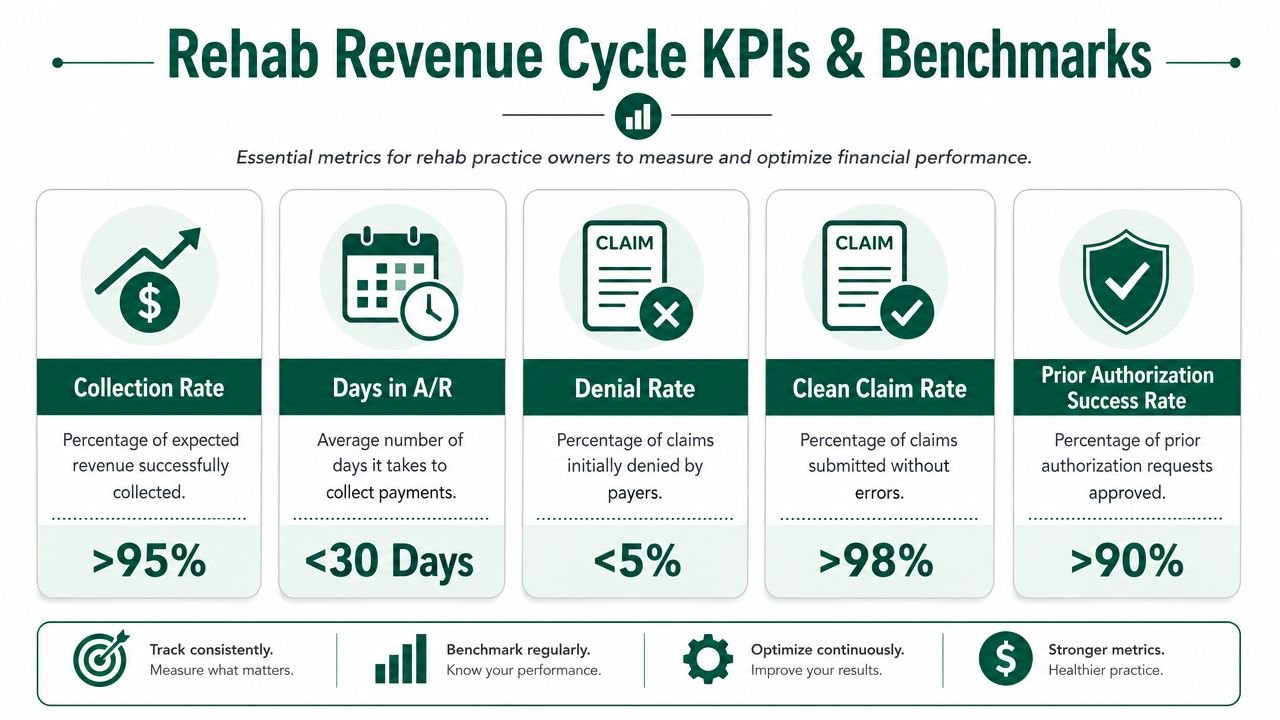
The KPIs that actually matter
Start with these:
- Clean claim rate: The share of claims that leave your system without avoidable errors.
- First-pass acceptance: How often payers accept the claim on initial submission.
- Denial rate: How much of your claim volume comes back unpaid at first adjudication.
- Days in A/R: How long revenue remains uncollected.
- Net collection rate: How much of the allowed amount the practice collects.
A strong billing process usually begins with claim scrubbing. One rehab billing provider says pre-submission claim scrubbing can push first-pass acceptance above 90% and reduce denials by more than 50%, as described in its rehab billing process overview. Even if you don't use that exact vendor, the takeaway is practical: front-end error checking is the most impactful control in therapy RCM.
What each metric tells an owner
A short formula table helps keep the discussion grounded:
| KPI | Basic formula | What it tells you |
|---|---|---|
| Clean claim rate | Clean claims / total submitted claims | How much preventable rework you're creating |
| Denial rate | Denied claims / total submitted claims | Whether payer edits and documentation issues are under control |
| Days in A/R | A/R balance divided by average daily charges | How fast claims turn into cash |
| Net collection rate | Payments collected / allowed amount | How much collectible revenue you're keeping |
If you already track broader business performance outside billing, this guide to essential financial metrics to track is a useful companion because it puts collections, cash flow, and operating discipline into the same management view.
How to use KPIs with your billing partner
Don't ask for "monthly reports." Ask for reports that isolate root causes. You want denial categories by payer, code family, rendering provider, and aging bucket. You also want to see whether front-end edits are reducing rework over time, not just whether staff are closing tasks.
For owners building or reviewing a dashboard, these medical billing KPIs to track give a solid framework. The point isn't reporting for reporting's sake. It's to identify which part of the revenue cycle is costing you the most money right now.
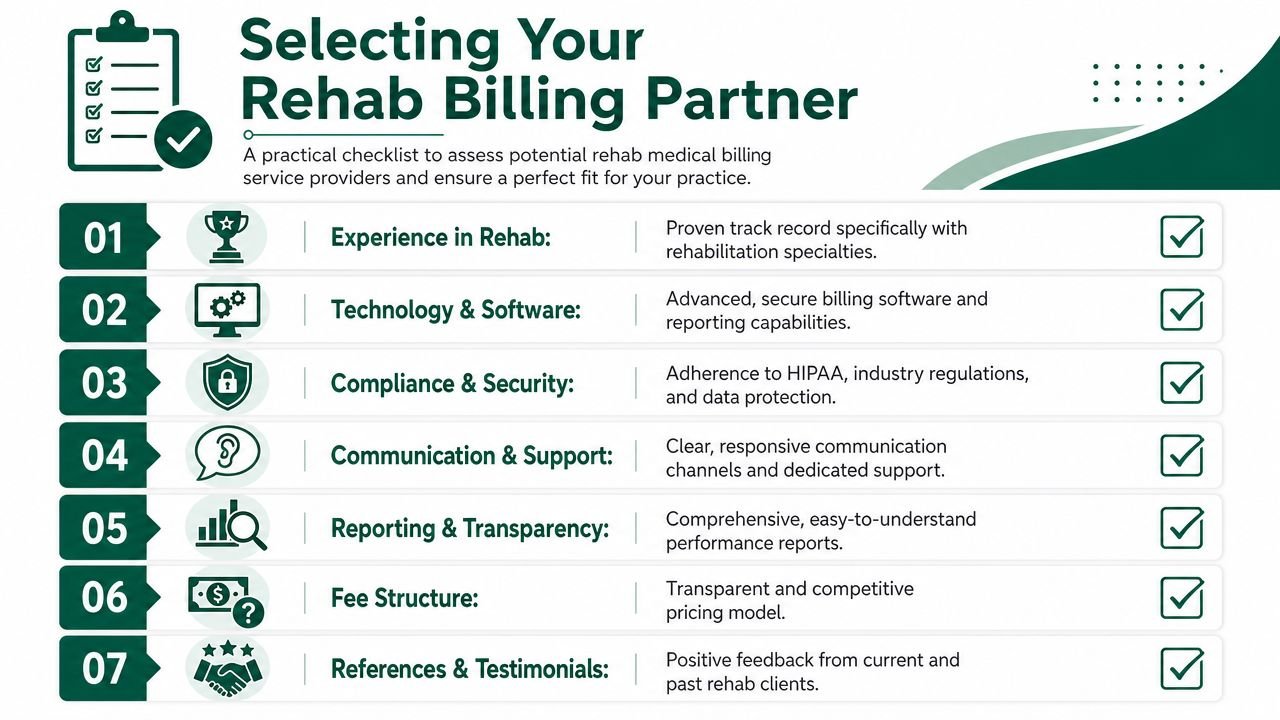
How to Evaluate a Rehab Billing Vendor
Most rehab billing vendors sound competent in a sales call. The actual difference shows up when you ask for process details. A therapy practice owner should evaluate a billing company the same way they would assess a clinical vendor. Look for repeatable workflow, not polished language.
Questions that reveal whether the vendor knows rehab
Ask for specifics, not promises.
How do you track authorizations and visit counts by payer and discipline?
If they can't describe the workflow for renewals, expired approvals, and therapist alerts, you'll eventually eat denied visits.Show me denial trends for therapy codes.
Ask for examples involving 97110, 97140, evaluations, re-evaluations, and same-day multi-service claims. You want to know whether they understand root-cause analysis at the CPT level.How do you review modifier combinations before claim release?
Many generic teams struggle at this stage. They know the modifier exists. They don't know when the documentation supports it.What happens when a payer asks for records?
This is a direct test of operational maturity.
A key benchmark here is turnaround discipline. This rehab billing best-practices review notes that CMS audit requests typically require a response within 45 days. Miss that window and a payable claim can become a total loss.
Slow document retrieval isn't an admin inconvenience. It's a revenue failure.
The vendor checklist owners should use
Use this list in every vendor conversation:
- Rehab-specific claim review: Can they explain PT, OT, and SLP claim logic in detail?
- EHR workflow fit: Will they work inside your existing system, or are they forcing process changes that create friction?
- Documentation request handling: Who gathers records, who reviews them, and how are deadlines tracked?
- HIPAA controls: Given the compliance exposure in billing, ask about encryption, access controls, and breach response.
- Reporting transparency: Will you get actionable denial and A/R reporting, or just summary totals?
- Escalation paths: When a payer issue affects many claims at once, who owns correction and communication?
If you're comparing options, this checklist of questions to ask a medical billing company before hiring is a practical screening tool.
One useful sign of fit
A credible partner should be willing to review your current workflows before talking about fee structure. For example, Happy Billing works inside an existing EHR and focuses on denial prevention, A/R follow-up, credentialing, and specialty-specific RCM. That kind of operating model can fit practices that don't want a platform migration, but it still needs to be tested against your therapy workflow, payer mix, and documentation habits rather than accepted on a generic pitch.
Pricing Models and Calculating Your ROI
Owners often ask the wrong first question about outsourcing. They ask what the vendor charges, when they should ask what the current billing setup is already costing the practice in delayed cash, write-offs, staff time, and missed appeals.
The common pricing models
Most rehab medical billing services use one of these structures:
| Model | How it works | Trade-off |
|---|---|---|
| Percentage of collections | Vendor fee rises or falls with collected revenue | Aligns incentives, but owners need transparency into posting and adjustments |
| Flat fee per claim | A set charge for each claim worked | Predictable, but it can overvalue simple claims and undervalue hard A/R |
| Per-provider flat fee | Fixed monthly amount by rendering provider | Easy to budget, but less tied to performance |
None of these models is automatically right. The best fit depends on claim complexity, visit volume, payer behavior, and whether your current pain is front-end denial prevention or back-end A/R recovery.
A practical ROI formula
Use this framework:
Net financial gain = new revenue captured + internal cost savings – vendor fee
"New revenue captured" includes claims that would otherwise deny, underpayments that get corrected, and balances recovered from old A/R. "Internal cost savings" includes less staff time spent on eligibility fixes, appeals, payment posting cleanup, and payer calls.
The mistake owners make is trying to force ROI into a neat projection before they have baseline data. Start with your current denial categories, oldest aging buckets, and the number of staff touches required to get a therapy claim paid. Then compare that to the vendor's process.
If you're also reviewing practice operations software at the same time, this comparison of Fresha competitors for growing businesses can help on the scheduling and management side. Billing ROI improves faster when the front desk, documentation flow, and revenue cycle aren't fighting each other.
For billing cost structure specifically, this breakdown of outsource medical billing cost is a good starting point. The right decision usually isn't "in-house versus outsourced" in the abstract. It's whether your current setup can stop preventable leakage in a therapy environment with strict payer rules.
FAQs About Rehab Billing Services
Should a physical therapy practice outsource billing or fix it in-house
If your denials come from a narrow process problem, such as weak authorization tracking or inconsistent payment posting, fixing it in-house can work. If the issues span coding review, payer edits, denial management, documentation requests, and aging A/R, outsourcing is often cleaner because it gives the practice a single accountable workflow instead of patching multiple internal gaps.
What makes rehab billing different from general medical billing
Therapy claims depend heavily on timed services, repeated visits, authorization control, discipline-specific modifiers, and medical necessity support across a treatment plan. A general billing team may submit claims correctly at a basic level but still miss the therapy-specific rules that determine whether those claims are paid without delay.
How long does it take to know whether a billing partner is improving revenue
You don't need to wait for a year-end summary. Owners should look early at cleaner submissions, fewer avoidable rejections, faster work on payer requests, and better visibility into denial categories. Those process changes usually appear before broader cash flow improvement becomes obvious in financial statements.
What should I ask before switching rehab medical billing services
Ask how the vendor handles prior auth tracking, same-day interdisciplinary sessions, modifier review, audit requests, old A/R, and payer-specific denial analysis. Also ask how they'll work inside your current EHR and what data they'll need from your team during transition. If they can't answer those questions in concrete workflow terms, keep looking.
If your therapy practice is seeing denials, slow collections, or unexplained leakage on recurring visits, a focused review usually finds the problem faster than another month of payer calls. Happy Billing offers a practical way to benchmark your current revenue cycle through a free billing audit so you can see where claims are breaking, where A/R is stalling, and whether rehab-specific billing support would improve collections.