Medical Billing Collection Services: Maximize Your Revenue
If you're looking at rising A/R, more patient balances aging out, and a billing team that keeps saying claims were “submitted,” then yes, medical billing collection services matter. They are the part of your revenue cycle that turns billed charges into cash, and when they fail, your practice funds payroll, rent, and growth out of a shrinking bank balance.
We have seen independent practices blame denials, payer mix, or patient responsibility when the underlying issue was weak follow-up after the claim left the door. A $300 office visit billed under CPT 99214 means nothing until the payer adjudicates correctly, the patient gets a clear bill, and someone collects the balance. For a practice owner, this isn't an administrative detail. It's revenue velocity, write-off control, and A/R discipline.
What Are Medical Billing Collection Services
Medical billing collection services are the systems and people responsible for pursuing payment after care is delivered. That includes insurance follow-up, denial resolution, patient balance collection, statement workflows, payment plans, and aged A/R recovery.
Most owners hear “collections” and think of old debt. That's too narrow. In practice, collections start the moment a claim for 99214, 93000, 20610, or any other service reaches adjudication and money is still missing. If your team can't convert adjudicated claims and patient balances into cash quickly, your practice is financing care for everyone else.
Why this matters to owners
When collections underperform, three things happen fast:
- Days in A/R rise: Cash arrives later, which forces you to carry payroll and overhead longer.
- Denials become write-offs: Claims that could have been appealed or corrected age out.
- Patient balances stall: Staff send statements, but nobody owns the money.
We have seen this pattern repeatedly. The front end works hard. Providers document. Claims go out. Then the back end goes passive, and revenue leaks for months.
The market has also changed. The U.S. medical billing services industry had 1,364 businesses in 2024, was valued at about $4.8 billion, and IBISWorld says the number of firms declined at a 3.4% CAGR from 2019 to 2024 while industry revenue contracted at a 2.5% CAGR over the same period, with a projected market size of $4.3 billion in 2026. That tells you the field is consolidating and weaker operators are getting squeezed out, while complexity remains high in reimbursement and collections workflows, according to IBISWorld's medical billing services industry profile.
Owner takeaway: collections is not a cleanup task. It's the final conversion point for every clinical dollar you earn.
If you want a plain-language baseline on the operational role itself, this overview of what medical billers do is useful. But from the owner's chair, the key point is simpler. If nobody owns follow-up with urgency, your practice gets paid last.
How Collections Fit Into Your Revenue Cycle
Collections sit at the end of the revenue cycle, but they also expose everything upstream that went wrong. Registration mistakes, weak eligibility checks, missing authorizations, sloppy coding, and poor modifier use all show up here as slower cash and harder recovery.

The anchor leg of your revenue cycle
Think of revenue cycle management like a relay race. Scheduling, registration, eligibility, coding, claim submission, posting, and denial handling all move the baton forward. Collections is the anchor leg. If that runner stumbles, the entire race is lost.
A common example is 99214 billed correctly but paired with bad insurance data, a missing referral, or a payer edit that nobody works promptly. The charge exists in your PM system. The revenue doesn't exist in your account.
For a broader operational view, this primer on what revenue cycle management means in practice is worth reviewing with your office manager.
Why owners should stop separating billing from collections
A weak practice treats collections like an afterthought. A strong practice uses collections data to fix upstream mistakes.
We have seen the best-performing groups ask questions like these every week:
- Which payer is delaying payment the longest?
- Which CPT codes trigger the most rework?
- Which balances are sitting with no next action?
- Which front-desk failures are creating avoidable patient A/R?
That is how you unlock trapped cash flow. Not by sending more statements. By tying every unpaid dollar to a broken process, assigned owner, and deadline.
A collection team that only “works old balances” is too late. A strong one prevents balances from becoming old in the first place.
The last mile is where practices lose money
Owners often focus on charge entry and denials because those are visible. Collections failures are quieter. The claim looks billed. The encounter looks complete. The month-end report looks acceptable until cash misses payroll targets.
That's why we audit the handoff points. Did the payer underpay? Was the patient balance explained early? Did someone follow up after the first statement? Was modifier usage correct on split services, diagnostic reads, or anesthesia concurrency? Those details decide whether the final mile is smooth or expensive.
The Outsourcing Decision Benefits vs Risks
Outsourcing collections can help, and it can also make a bad situation worse. The question isn't whether outsourced billing is better. The question is whether your current team can move money fast, protect patient relationships, and manage payer friction without constant owner intervention.
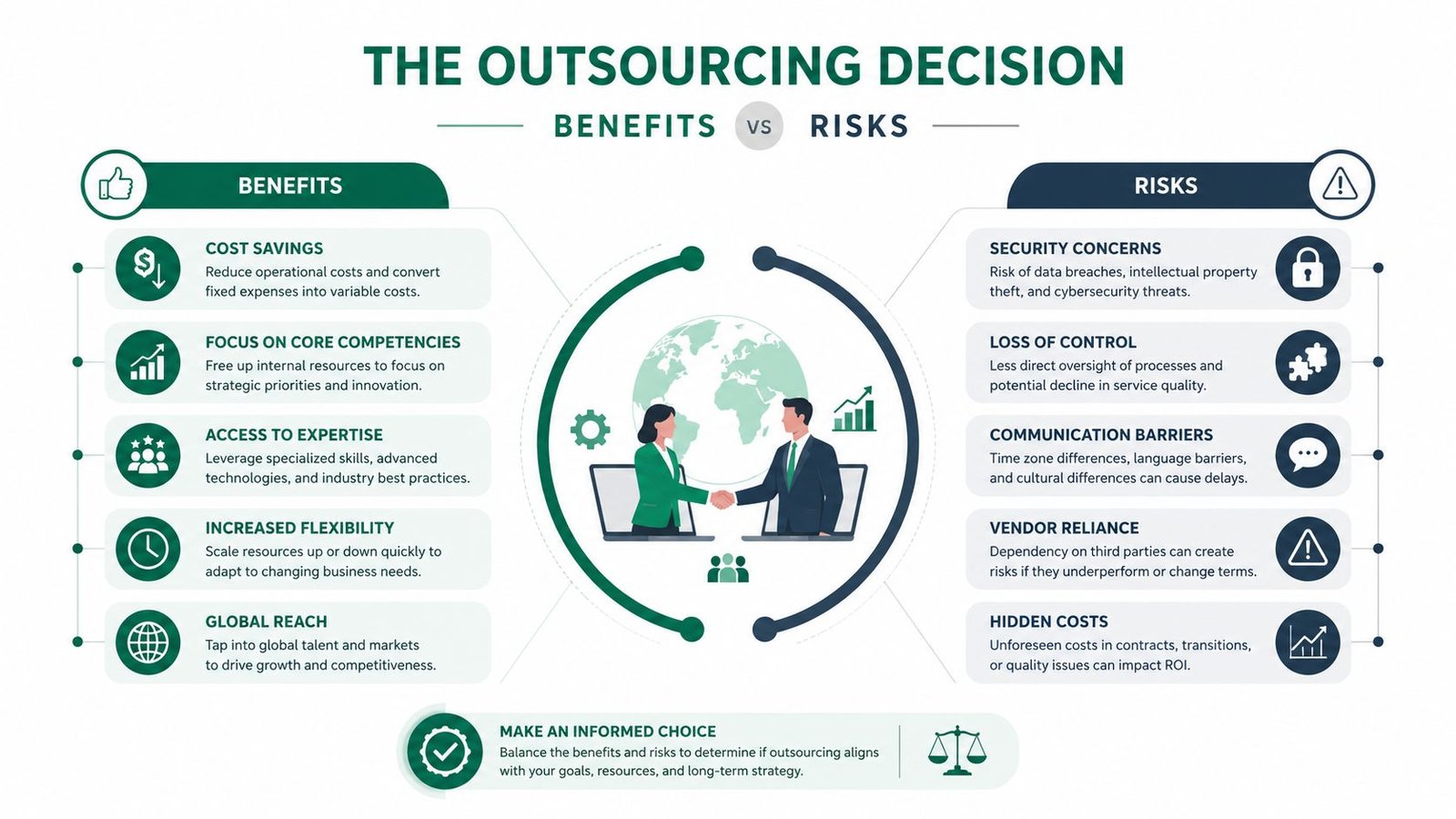
Where outsourcing helps
We have seen outsourcing work well when a practice has one or more of these problems:
- No consistent denial follow-up: Claims get touched once, then sit.
- No specialty depth: The team can post payments, but they can't handle modifiers like 26, TC, QK, or payer-specific edits with confidence.
- No patient collection discipline: Statements go out, but self-pay cash still drifts.
- No owner visibility: You receive summary reports, not actionable revenue intelligence.
A competent outside partner gives you scale, process discipline, and tighter management of claim status, patient balances, and payer follow-up. It also removes the single-point-of-failure risk you get when one experienced biller runs your whole back office.
Where outsourcing goes wrong
Now the hard truth. Plenty of vendors are good at onboarding calls and bad at collections. They promise dashboards, then hide behind generic reports. They say they “handle everything,” then push difficult payer issues back to your office. They talk about technology, but their patient billing experience still depends on mailed statements and reactive phone calls.
Outsourcing is a trade. You give up daily control in exchange for better execution. If execution doesn't improve, you've added cost without fixing revenue.
The biggest risks are straightforward:
| Decision risk | What it costs you |
|---|---|
| Weak specialty fit | More denials, undercoded services, slower appeals |
| Poor patient communication | Lower collections, more complaints, lost goodwill |
| Bad reporting | You can't tell whether A/R is improving or just being rearranged |
| Compliance gaps | Legal exposure and expensive remediation |
| Slow implementation | Cash disruption during transition |
If you're deciding between in-house and outsourced support, this comparison of in-house vs outsourced medical billing is a practical starting point.
A good outsourcing decision looks boring
The right partner isn't the one with the flashiest pitch. It's the one that answers specific questions with specific workflows. Who handles modifier 26 professional components in cardiology reads? Who works aged A/R by payer class? Who handles unresolved patient balances before they become bad debt? Who owns compliance review for collection communications?
We have seen owners get burned when they bought “full-service billing” but never defined what full service meant.
Your Vendor Selection Checklist
A weak billing vendor does not fail loudly. It shows up as cash drag. A/R creeps up, denial rework piles up, patient balances age past collectability, and the owner keeps hearing that the team is "working on it." If you are hiring medical billing collection services, evaluate the vendor the way you would evaluate a capital investment. Ask what revenue they protect, how fast they collect it, and where they usually fail.

Check specialty expertise first
Specialty fit affects cash within the first few weeks. A vendor that misses specialty billing rules will trigger preventable denials, slower appeals, and lower allowed amounts.
Ask specific workflow questions tied to your revenue. In cardiology, ask who reviews modifier 26 and TC splits before claim submission. In anesthesiology, ask how they manage modifier QK and concurrency documentation. In orthopedics, ask who tracks global periods and how they separate payable post-op visits from bundled follow-up. We have seen owners sign with a generalist vendor, then spend months cleaning up specialty-specific errors that cut collections and push A/R older.
Do not accept broad answers. You are not buying software access. You are buying judgment.
Demand modern payment workflows
Patient collections rise when paying is easy and follow-up is structured. AccessOne explains in its guide to medical billing collections that digital, mobile-friendly payment options matter because they remove friction from the payment process.
That only matters if the workflow is built correctly. Ask whether patients can pay by phone without a portal login, whether the system supports common digital payment methods, whether balances are worked by age and balance size, and whether pre-service and post-service collection activity sits in one process instead of being split across systems.
We have seen patient A/R improve after practices fixed payment friction alone. Same patient population. Better process. Faster cash.
Treat security and compliance as financial risk control
Security failures are revenue problems. A vendor that mishandles PHI, call recordings, or financial notes can trigger legal cost, remediation cost, and operational distraction right when your staff should be focused on collections.
Ask for documented access controls, audit trails, user-permission rules, and retention policies for statements, calls, and payment communications. If your practice uses dictated notes or recorded conversations in revenue operations, WhisperAI for secure healthcare transcripts shows the level of compliance detail you should expect from any company touching sensitive data.
If a billing company cannot explain its security controls in plain English, do not give it access to your accounts.
Make pricing transparent
Pricing hides more bad decisions than demos do. Percentage-of-collections pricing can work, but it also makes weak performance harder to spot if reporting is thin. Flat fees can look cheaper until denial work, old A/R recovery, patient calls, and appeals get carved out as extras.
Get a written breakdown of:
- What counts as collected revenue
- Whether patient balances are included
- Whether old A/R cleanup is separate
- Whether credentialing, appeals, call handling, and statements cost extra
- How fees change during implementation or after contract renewal
Happy Billing is one example of a vendor that offers full-cycle RCM, denial management, and A/R recovery inside existing EHR workflows. The brand matters less than the operating model. Check whether the vendor's scope matches the work your practice is failing to get done.
Put service levels in writing
A vague contract protects the vendor. It does nothing for your cash flow. You need written ownership for follow-up, denial rework, patient balance outreach, reporting cadence, escalation paths, and implementation deadlines.
Use this scorecard in vendor interviews:
| What to ask | Why it matters financially |
|---|---|
| Who owns aged A/R follow-up? | Prevents balances from rolling into write-offs |
| How do you report denial categories? | Shows whether recurring revenue loss is getting fixed |
| How often do you review payer trends with us? | Catches cash problems before month-end surprises |
| How do you handle patient complaints about bills? | Protects collection yield and referral reputation |
| What does implementation require from our staff? | Reduces transition-related cash disruption |
Before you sign, run the interview against these questions to ask a medical billing company before hiring. A good vendor should answer them with owners, workflows, turnaround times, and sample reports. If they answer with sales language, keep looking.
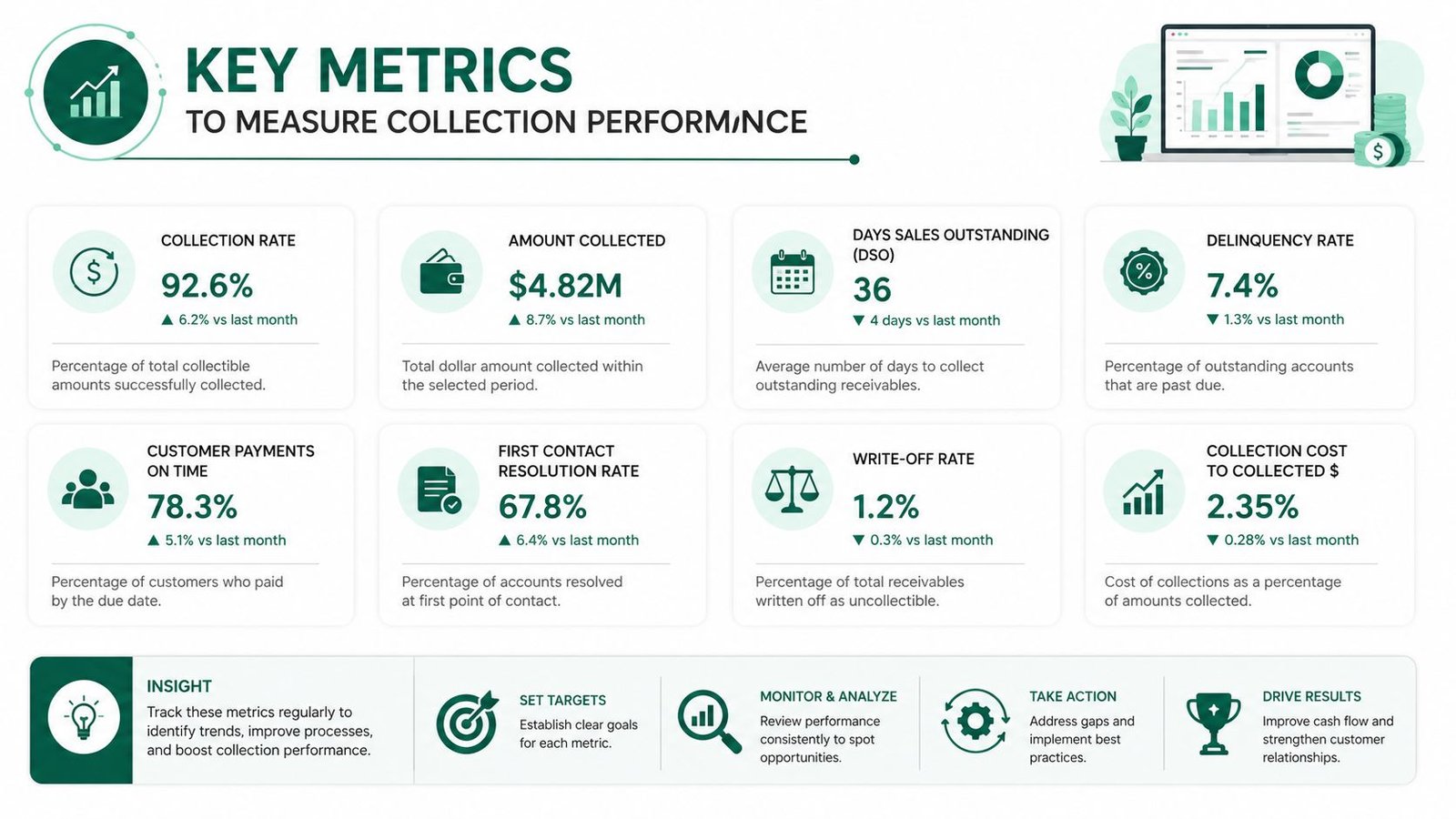
Key Metrics to Measure Collection Performance
A vendor can sound organized in meetings and still miss your cash targets by six figures a year. Measure collection performance the way an owner measures any financial operator. By cash collected, speed to cash, and revenue lost to avoidable failure.
Net collection rate shows how much earned revenue you actually keep
Net collection rate is the first number I check because it answers the owner's real question. Are we collecting the dollars we had a right to collect after contract adjustments?
Analysts at Experian cite a healthy net collection rate at 90 to 95 percent, with best-in-class at 95 percent or higher, in their discussion of patient collection metrics. If your practice sits below that range, the gap is not academic. It is lost revenue. On $4 million in adjusted annual charges, a three-point shortfall means $120,000 not making it into the bank.
We have seen owners tolerate weak net collection rates because charges were growing. That is a bad trade. Growth does not fix poor collection yield.
Days in A/R shows whether your money is arriving on time
Days in A/R measures cash speed. Owners should treat it like a liquidity metric, not a billing department detail.
A/R that sits too long creates real operating pressure. Payroll gets tighter. Physician distributions get delayed. Credit lines get used for expenses current collections should have covered. We have seen practices with acceptable monthly production still feel cash poor because too much value was trapped beyond 60 and 90 days.
Watch the trend, not just the snapshot. If Days in A/R rises while charges stay flat, your collection partner is getting slower or your front-end and denial problems are feeding the back end.
Patient collection rate tells you whether self-pay balances are collectible or just aging
Patient responsibility is where many practices lose margin. The numbers are usually worse than owners expect.
Experian's 2025 benchmark materials report overall patient collection rates averaging only 34 to 48 percent, with commercially insured patient collections falling as low as 34.4 percent. Collection on balances of $7,500 or more drops to 17 percent. That should change how you judge a billing vendor. If they rely on mailed statements and slow follow-up, they are not managing patient A/R. They are aging it.
We have seen patient collection rates improve when practices fix communication speed, bill clarity, and payment conversations early. The operational logic is the same one highlighted in SkipCalls' analysis of call revenue. When people cannot get answers, they delay action. In healthcare, delayed action becomes bad debt.
Use a short owner dashboard
Do not ask for 40 billing metrics. Ask for five that expose revenue gain or loss fast.
- Net collection rate: Measures how much collectible revenue you kept
- Days in A/R: Measures how quickly revenue turns into cash
- Patient collection rate: Shows whether self-pay balances are converting
- First-pass clean claim rate: Shows whether preventable errors are creating rework and delay
- Denial rate by payer and CPT code: Shows exactly where reimbursement is getting blocked
Review them monthly, and require trend lines. One month of data can hide a problem. Three months usually exposes it. If you want a practical owner-level template, use this guide to medical billing KPIs to track.
A billing partner should be able to explain every movement in these numbers, what they changed, and how much cash that change produced. If they cannot tie activity to lower A/R days, lower denial rates, or higher net collections, they are giving you process reports instead of financial performance.
Common Pitfalls That Leak Practice Revenue
The biggest collection failures aren't always dramatic. They're routine, tolerated, and expensive. We have seen owners lose revenue because nobody challenged the habits that felt normal.
Passive A/R management
A lot of teams “work A/R” by touching the newest problems first and avoiding aged balances that require persistence. That approach feels busy but doesn't recover much. Old claims need documented next steps, payer-specific escalation, and staff who know when to call, appeal, rebill, or write off with justification.
If your aging report keeps growing in the same buckets month after month, that isn't a staffing issue alone. It's a leadership issue.
Ignoring patient communication failures
Poor collection performance often starts before the statement. Unanswered calls, confusing bills, and weak payment explanations kill recovery. Owners who want a non-healthcare example of how missed communication turns into lost dollars should look at SkipCalls' analysis of call revenue. The principle carries over. When patients can't get clarity, they delay payment.
The fix isn't harsher collections language. It's cleaner financial communication, faster callbacks, and easier payment options.
Compliance blind spots
Many practices get careless concerning patient-debt rules. These are not just operational details. They are legal exposure.
California's DFPI notes that hospitals can't sell patient debt to a debt buyer unless certain conditions are met around financial assistance eligibility and patient outreach, and patients can request debt verification from both the collector and the provider, as explained in California DFPI guidance on medical debt collection rights.
Even if you're not a California hospital, the lesson is broad. If your collection workflow doesn't include debt verification handling, financial assistance screening where applicable, and documented patient-rights procedures, you're taking compliance risk you may not even see.
Your vendor can create the problem. Your practice still owns the consequences.
FAQs From Practice Owners
Should I outsource medical billing collection services or fix my current team first
Start with diagnosis, not ideology. If your current team has good specialty knowledge, strong payer follow-up, and clean reporting, fix the workflow. If nobody owns aged A/R, patient balances stall, and you still can't get straight answers on denials, outsourcing is usually faster than rebuilding from scratch.
What should I ask a billing company before I sign
Ask who owns denials, who owns aged A/R, how patient balances are collected, how often they review payer trends with you, and how they handle specialty-specific coding issues like modifier 26, TC, or QK. If they answer with sales language instead of process detail, keep looking.
How long should I give a new billing partner to prove results
You should see operational clarity quickly. That means cleaner reporting, visible ownership of A/R, and a concrete work plan for denials and patient balances. If a vendor still can't show what's being worked, why it's unpaid, and what changes they're making, you don't have a revenue partner. You have a reporting vendor.
How do I know if my practice needs an outside audit first
Get an outside audit when your numbers don't match your effort. If providers are busy, charges are posting, and cash still lags, something in your revenue cycle is broken. An independent review is the fastest way to find whether the problem is front-end errors, denial handling, patient collections, or poor vendor execution. If you want a starting point, request a free billing audit for your practice.
If your practice is carrying too much A/R, losing money on preventable denials, or tolerating slow patient collections, get a second set of eyes on the numbers. Happy Billing works with physician groups that need tighter revenue cycle control, clearer reporting, and a practical plan to improve cash flow without changing their clinical workflow.