Balance Billing Guide for OON Practices Under the NSA
If you're an out-of-network physician owner, balance billing didn't disappear in 2022. It got regulated. The No Surprises Act changed which claims you can pursue from patients, which claims have to be fought with payers, and which workflow mistakes now turn directly into revenue leakage, avoidable write-offs, and compliance exposure.
Most OON practices don't have a fee schedule problem. They have a classification problem. Staff misclassify protected claims, fail to capture valid consent, accept weak initial payments, or let negotiable underpayments age in A/R until they become write-offs. That's why balance billing now sits inside revenue cycle strategy, not just compliance. If your team still treats the NSA as a patient-facing rule instead of a payer-facing reimbursement framework, you're leaving money on the table.
The OON Practice Owner's Guide to Balance Billing
Balance billing is the difference between your charge and the insurer's allowed amount. HealthCare.gov's balance billing glossary gives the simple example of a service billed at $100 with a plan-allowed amount of $70, leaving a potential $30 patient bill unless network or legal protections block it. For an OON practice owner, that gap is not an abstract definition. It's the revenue segment your team either collects lawfully, disputes successfully, or loses through bad process.
That matters most in specialties where out-of-network clinicians show up inside otherwise in-network episodes. Think anesthesia, radiology, pathology, and emergency medicine. If your practice touches facility-based care, the same encounter can produce three different financial paths: prohibited balance billing, permitted balance billing with valid consent, or insurer underpayment that belongs in negotiation and possible IDR.
Why owners should care now
We see the same operational failure over and over. Front-end staff assume every OON claim is now unbillable to the patient. Back-end staff assume every low payer payment is final. Both are wrong, and both increase A/R days.
Your owner-level question isn't "what is balance billing?" It's "which receivables belong in patient responsibility, which belong in payer dispute, and which require immediate compliance holds?" That distinction determines whether your practice preserves margin or bleeds it away through passive posting.
Practical rule: Every OON encounter should be tagged before claim submission as protected, consent-based, or dispute-track.
The revenue lens
A clean billing operation now needs more than coding accuracy. It needs encounter-level decision logic tied to eligibility, place of service, facility network status, provider role, and documentation. If your current billing partner can't map those variables consistently, your balance billing risk becomes an A/R problem first and a legal problem second.
For a broader framework on tightening these owner-level controls, review this guide to RCM for physician practices.
Decoding the No Surprises Act for Your Practice
The No Surprises Act is best understood as a rulebook for OON reimbursement. It took effect in 2022 and protects patients from balance billing in emergency care, air ambulance services, and in-network hospital settings when out-of-network clinicians are involved, according to CMS training materials on balance billing under the NSA. Those protections generally apply for plan years starting on or after January 1, 2022, and only to covered benefits under the patient's in-network terms.
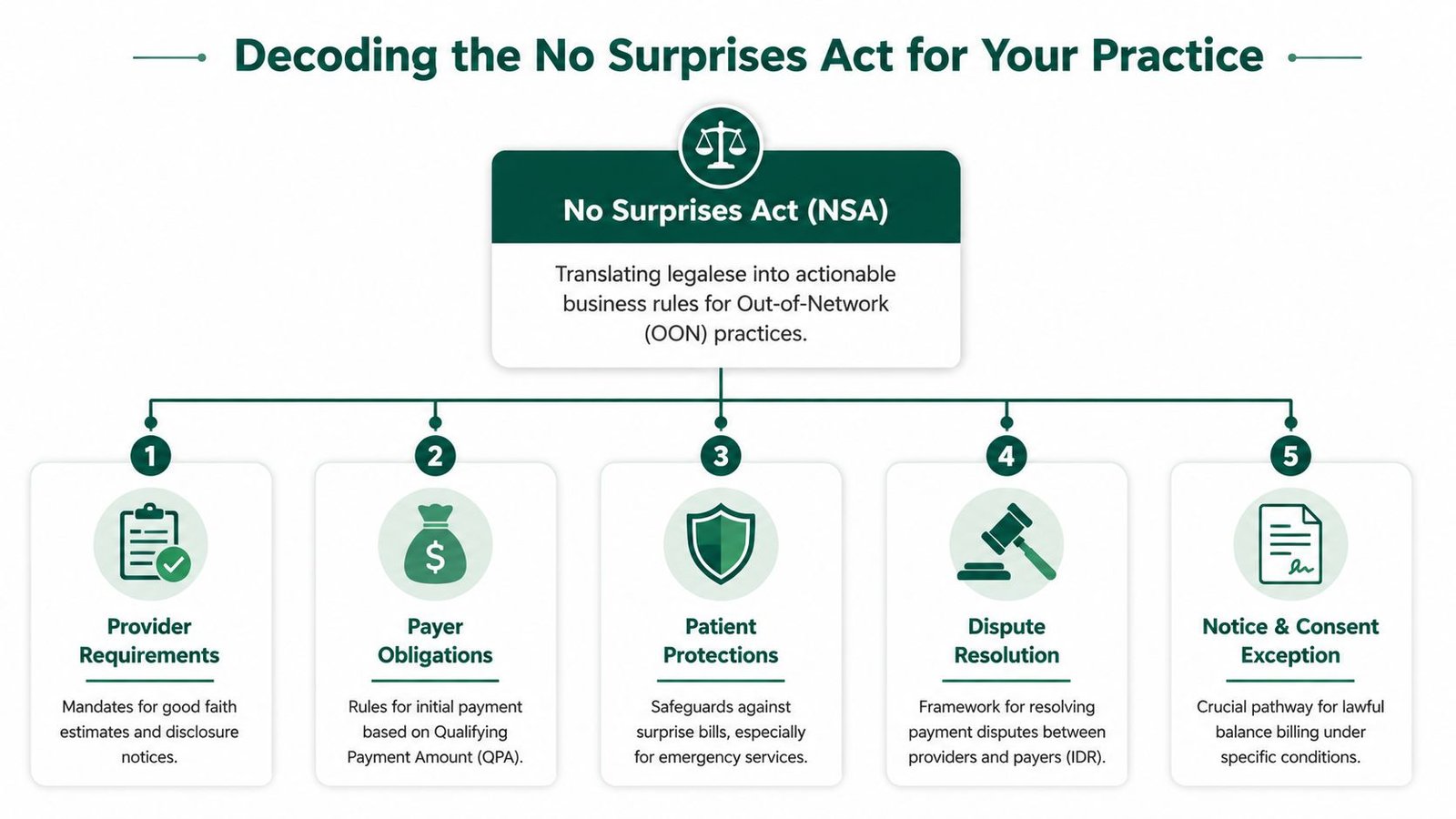
For an OON owner, that means one thing. You can still operate an OON model, but you can't use one collection strategy for every encounter. You need a triage model.
Three claim buckets that matter
Use this framework:
| Claim type | What it means for your practice | Revenue action |
|---|---|---|
| Protected claim | Federal rules bar balance billing | Bill insurer, verify cost-sharing logic, monitor underpayment |
| Consent-based claim | Balance billing may be allowed if notice and consent rules were followed | Validate documentation before patient billing |
| Dispute-track claim | Payment disagreement belongs with payer, not patient | Open negotiation, prepare for IDR if needed |
Owners lose money when they let staff collapse all three buckets into one generic OON workflow.
Where balance billing is off limits
The clearest prohibited categories are emergency services, air ambulance, and certain situations involving out-of-network clinicians in in-network facilities. If your physician furnishes emergency care, post-stabilization care subject to NSA rules, or certain facility-based ancillary services, the default assumption should be that patient balance billing is restricted unless a valid exception applies.
That creates a direct control point at registration and charge review. Your front office must identify whether the service is covered under the patient's plan, and your back office must know whether a patient statement is legally available at all.
If your team is trying to fix NSA exposure after statements go out, the process already failed.
Why documentation and communication systems matter
NSA workflows now intersect with phone, intake, scheduling, and disclosure practices. Practices that use automation for reminders, intake calls, or financial disclosures should also understand adjacent compliance expectations in payer communications and consumer outreach. This overview of AI calling regulations in insurance is useful context if your operation is adding automation to financial communication workflows.
For OON-specific reimbursement strategy, this resource on out-of-network billing is worth reviewing alongside your intake and claims process.
Challenging the QPA How to Fight Underpayments
Once a claim falls into the NSA payment framework, the insurer's initial payment is not the finish line. It's the opening position. If your team posts it and moves on, you've turned payer advantage into your own write-off policy.
The QPA, or qualifying payment amount, is the insurer's benchmark inside the NSA framework. Owners should treat it as a payer-generated anchor, not a neutral truth. The practical issue is simple: if the payer's benchmark doesn't reflect your subspecialty, your market, or the actual complexity of the case, a low initial payment can look administratively tidy while still being financially wrong.
Where payer QPA logic can break down
In our experience, practices should challenge payment logic when any of these issues appear:
- The code set doesn't reflect the service mix. A payer may benchmark a claim too broadly and ignore complexity signals built into the CPT selection.
- The geographic logic looks off. If the insurer's payment doesn't align with the market your practice serves, the QPA may be diluted.
- Subspecialty distinctions vanish. That's a common problem in anesthesia subspecialties, high-acuity procedural care, and facility-based consultative work.
- Case context gets stripped away. Time, medical necessity, post-stabilization facts, or unusual procedural burden may justify a stronger payment argument.
What owners should require from their team
Don't let underpayment review live only inside the EOB posting queue. Build an escalation standard around documents your practice already controls.
A strong underpayment file usually includes:
- The remittance or EOB showing the payer's payment position.
- The claim form and operative or encounter documentation supporting the billed service.
- Any records showing physician training, experience, or clinical complexity relevant to the service.
- Prior negotiation history with the payer, especially if the same code family is repeatedly underpaid.
- A written explanation tying the service facts to why the payer's payment is inadequate.
For owners reviewing high-risk service lines, modifier logic also matters. In anesthesia, payment arguments often live or die on whether the underlying record supports the billed units, concurrency position, and modifiers. In procedural specialties, disputed value may turn on assistant surgeon involvement, imaging guidance, or distinct procedural services. If your team can't read an insurer explanation precisely, they can't contest it intelligently. This walkthrough on how to read an Explanation of Benefits is useful for tightening that review.
Owner takeaway: The QPA is a benchmark you evaluate. It is not an instruction you obey.
When to escalate instead of adjust off
A denial can be a coding problem. An underpayment under NSA rules is often a negotiation problem. Those require different staff, different templates, and different deadlines. If your billers treat every short payment like a contractual adjustment, your OON strategy is broken at the posting level.
Mastering the Independent Dispute Resolution Process
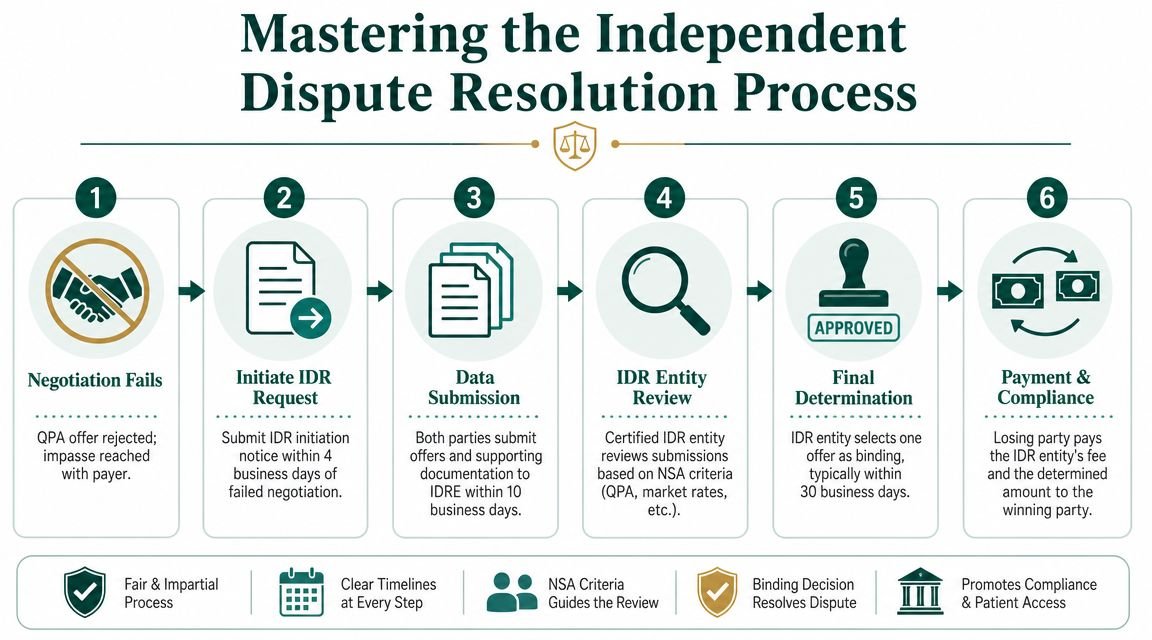
When negotiation fails, the federal Independent Dispute Resolution process becomes a business tool. Too many owners hear "IDR" and think lawsuit. That's the wrong mindset. IDR is a structured payment challenge, and practices that document well usually perform better than practices that rely on outrage.
The larger policy shift is already clear. A Georgetown review of early No Surprises Act complaint data notes that CMS reported 7,888 NSA-specific complaints in the first 22 months, while insurer trade groups estimated about 1 million claims per month were being submitted for care covered by the law. The same review explains that the law shifted payment disputes away from patients and into negotiations and binding arbitration between providers and insurers. For a specialty owner, that's the core lesson. Payment fights that used to spill onto the patient ledger now belong in a formal payer dispute channel.
How to think about IDR
IDR only works if your staff sees it early enough. The usual failure isn't weak argumentation. It's missed follow-up, incomplete files, and no escalation trigger after an inadequate initial payment.
Your internal workflow should answer four questions immediately:
- Was the claim NSA-governed?
- Did the payer issue an inadequate payment or denial?
- Did your team preserve all supporting documentation?
- Is the potential recovery worth formal escalation?
What a strong IDR package looks like
The best submissions read like a disciplined business memo, not a complaint letter. Include the facts that make your offer credible:
| Document or factor | Why it matters |
|---|---|
| Initial payment or denial record | Establishes the payer's position |
| Claim and clinical record | Supports coding, complexity, and medical context |
| Provider qualifications | Can help show why the service merits stronger payment |
| Prior contracting efforts | Shows market context and network negotiation reality |
| Written payment rationale | Gives the reviewer a clear reason to choose your offer |
Your file should be organized by claim, service line, and payer pattern. If you rely on one-off spreadsheet tracking, you'll miss repeatable underpayment themes.
Build IDR files the same way you build litigation holds. Complete, chronological, and easy for a third party to follow.
Where owners gain leverage
The financial decision isn't whether every underpayment should go to IDR. It won't. The decision is whether your practice has a filter that identifies which claims justify the effort. High-acuity services, repeated low payer positions on the same CPT family, and claims with unusually strong documentation often deserve priority review.
That also means your denial team and your underpayment team can't operate as separate silos. A payer that is habitually underpaying OON claims often leaves clues in appeal outcomes, EOB language, and remittance patterns. If you want those patterns surfaced early, your team needs a shared workflow. This guide on how to appeal a denied insurance claim can help align denial review with dispute escalation.
What owners should audit quarterly
Review these items every quarter:
- Protected-claim payment variance by payer and CPT family.
- Negotiation outcomes by service line.
- IDR filing readiness based on document completeness.
- Write-offs on OON claims that should have been disputed instead.
If you don't audit those categories, you won't know whether your billing operation is preserving your OON economics or conceding them.
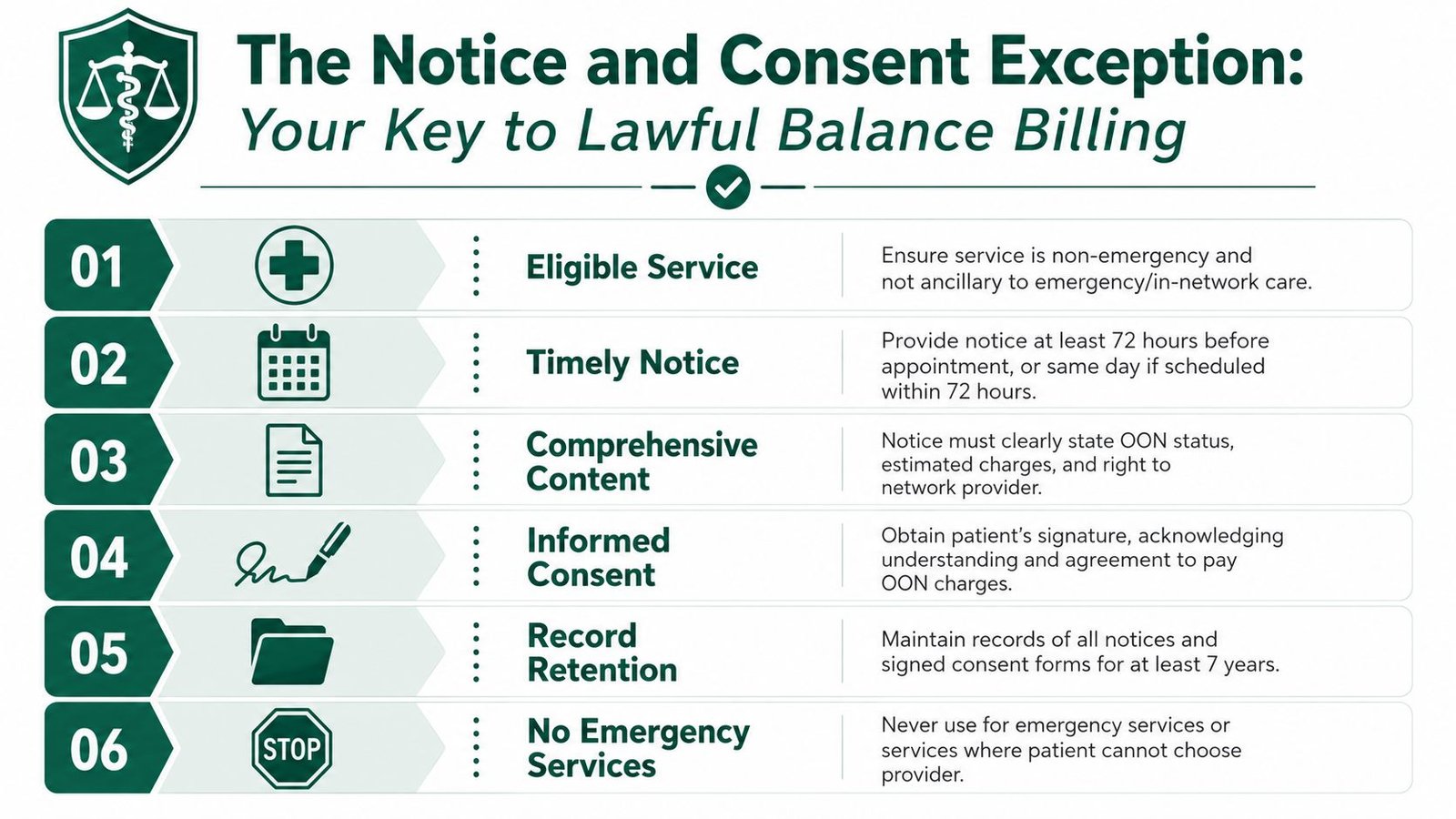
The Notice and Consent Exception Your Key to Lawful Balance Billing
This is the most misunderstood revenue protection tool under the NSA. The law reduced patient liability in many settings, but it did not eliminate all out-of-network billing scenarios, and the Mayo Clinic overview of the No Surprises Act notes that the law blocks balance billing for certain ancillary services such as anesthesiology and radiology and for emergency care, including some post-stabilization situations, unless the patient gives written consent. Owners need to stop treating notice and consent as a generic financial form. It is a narrow legal pathway, and sloppy execution destroys its value.
When consent may help and when it won't
Notice and consent is not a cure-all. It does not rescue emergency claims. It does not fix prohibited ancillary service situations just because the patient signed a paper. And it does not protect your practice if the form was bundled into general treatment paperwork or presented in a coercive way.
Owners should teach staff one hard rule: if the patient didn't have a meaningful choice, your consent strategy is weak before it starts.
The operational checklist
A usable internal checklist should cover at least these points:
- Correct encounter type. Confirm the service is one where notice and consent can apply.
- Timing control. Deliver the form early enough to support lawful use, not after the financial decision was effectively forced.
- Separate document. Keep it apart from clinical consents and routine registration paperwork.
- Clear OON disclosure. State plainly that the provider is out of network.
- Estimated charges. Include a realistic estimate tied to the planned service.
- Alternative availability. Inform the patient that in-network options may be available.
- Signature capture. Use a process that records date, time, and document version.
- Retention discipline. Store the executed form where billing staff can retrieve it before statement release.
- Claim flagging. Mark the account so the back office knows patient billing may be lawful.
- Pre-statement validation. Require a final review before any balance bill goes out.
A signed form that can't be retrieved quickly is the same as no form at all.
Specialty-specific warning
Facility-based specialists often get this wrong because they assume the surgeon's scheduling process solved the financial issue. It didn't. If your anesthesiology, radiology, or pathology group depends on the hospital or ASC to manage consent perfectly, you're relying on someone else's workflow to preserve your receivable.
For CPT-heavy specialties, the safest approach is service-line rules. For example, if the claim is tied to emergency medicine codes or protected facility-based ancillary scenarios, your billing platform should block patient balance billing by default. If the service is a scheduled non-emergency professional service where a lawful exception may apply, the account should require consent verification before statements release.
The owner's policy decision
Don't ask your staff to "use consent when needed." That's too vague. Give them a written policy that answers these questions:
| Policy question | Required owner decision |
|---|---|
| Which service lines may use notice and consent? | Define them explicitly |
| Who presents the form? | Assign ownership to a role, not a department |
| Who validates it before billing? | Require back-end review authority |
| What happens if documentation is missing? | Set automatic billing holds |
That policy protects revenue because it reduces false assumptions. It also protects the practice because it prevents unlawful patient billing based on incomplete front-desk execution.
Operationalizing NSA Compliance in Your RCM Workflow
A claim gets scheduled on Monday, the procedure happens on Thursday, the ERA posts two weeks later, and your staff sends a patient statement before anyone confirms whether the account was NSA-protected, consent-eligible, or ready for dispute. That is how out-of-network practices create preventable refunds, write-offs, and legal exposure.
Treat NSA compliance as routing logic inside your revenue cycle, not as a legal checklist sitting in a binder. The law changed the billing rules. Your workflow has to enforce them before cash is posted and before statements are released.
Build routing rules at intake
Your front end should collect the facts that determine the claim path downstream. If those fields are wrong, everything after them gets more expensive to fix.
Capture and verify:
- Plan status. Confirm whether the patient's coverage triggers NSA payment and cost-sharing rules.
- Site of service. Office claims do not follow the same path as hospital, ASC, emergency, or post-stabilization encounters.
- Provider type and role. Rendering specialist, assistant surgeon, anesthesiologist, radiologist, pathologist, and consultant claims carry different billing risk.
- Encounter classification. Separate elective scheduled care from emergency and facility-based protected scenarios.
- Consent documentation status. Staff should confirm that the record exists, matches the encounter, and is retrievable before billing activity starts.
Your PMS or billing platform should assign a billing path from those inputs. If the system cannot do that, require a manual pre-bill review. Do not let coders, posters, or statement teams guess.
Split the work into distinct revenue queues
A single A/R bucket hides NSA mistakes. Create separate queues so your team can work each claim under the correct business rule.
- Protected claims queue for payer follow-up, patient cost-sharing accuracy, and statement suppression.
- Consent-approved OON claims queue for accounts that can lawfully move to patient balance billing.
- NSA underpayment queue for claims that need negotiation support, QPA review, and possible IDR escalation.
That separation protects margin. It also gives you cleaner reporting on where revenue is stalling. If your team is redesigning workflows, automation, and queue logic, Resolut's billing automation insights are worth reviewing.
Review the right exceptions every week
Weekly management should focus on exceptions, not generic aging totals.
| Queue | Weekly review question |
|---|---|
| Protected claims | Did the payer apply the right payment method and patient responsibility? |
| Consent-approved claims | Is the documentation complete and validated before any patient statement goes out? |
| NSA underpayments | Has the claim been evaluated for challenge, negotiation, or IDR filing? |
Owners should also force specialty-specific checks into that review. Anesthesia claims can turn on modifier accuracy and concurrency facts. Surgical claims can shift payment position based on assistant surgeon modifiers and global rules. Imaging, pathology, and interventional groups need staff who can catch place-of-service, technical-professional split, and facility-based protection issues before those accounts age into bad debt.
Rule: statement release comes after compliance validation, never before it.
Audit the workflow like an owner
Do not limit audits to coding and claim edits. Audit the handoffs that decide whether you collect, appeal, dispute, or suppress billing.
Review these points:
- Registration accuracy for plan data, facility type, and encounter classification
- Document retrieval for signed notice and consent records
- Payment posting logic for underpayments versus true contractual adjustments
- Escalation rates on low OON payments that should have been challenged
- Statement controls that stop protected claims from reaching the patient
Use this section of your operation to tighten cash control. Strong NSA execution does more than avoid penalties. It preserves lawful patient billing where allowed, identifies underpayments faster, and keeps staff from writing off revenue that should have gone to negotiation or IDR. For a broader benchmark, review these revenue cycle management best practices and compare them against your current intake, posting, and escalation workflow.
Frequently Asked Questions for OON Practice Owners
Is an out-of-network model still viable after the No Surprises Act
A practice owner sees a clean remittance, assumes the payer position is final, suppresses the patient balance, and writes off the gap. That is how OON revenue disappears after the NSA.
An out-of-network model still works. It works when you treat the NSA as a payment rule set, not a ban. Practices that depended on routine balance billing in protected settings lost ground. Practices that classify claims correctly, use lawful notice and consent where available, and challenge weak payer payments through negotiation and IDR still have room to protect margin.
Should my practice rely on patient agreements to protect revenue
Only where federal rules allow it, and only with a disciplined process. A generic financial responsibility form does not preserve your right to bill the patient. The document has to match a valid notice-and-consent exception, be presented on time, be signed correctly, and be retrievable on demand.
If your team cannot prove every step, do not treat the balance as collectible.
When should we escalate an underpaid OON claim instead of writing it off
Escalate fast when the claim falls under NSA payment rules, the payer amount is weak, and your file supports a stronger reimbursement position. Watch payer patterns by code family, specialty, and facility. Repeated low payments usually signal a payer strategy or an internal posting failure, not a claim that deserves an adjustment.
Owners should set a hard rule here. Staff do not write off OON underpayments just because the ERA posted without an edit.
Do we need a specialist billing partner for OON claims
Yes, if your current team treats NSA claims like ordinary insurance billing. OON payment defense now depends on claim classification, consent validation, underpayment detection, dispute documentation, and deadline control. General billing teams miss revenue when they stop at claim submission and payment posting.
You need operators who understand how to preserve lawful patient billing where allowed and how to press payers when it is not.
If your practice is out of network, generic billing support is not enough. You need a partner that can find NSA compliance gaps, identify missed IDR opportunities, and stop underpayments from turning into write-offs. Happy Billing can review your current workflow and show you where your OON process is losing cash. Start with a focused free audit for your practice.