Your Ultimate Anesthesia CPT Code Reference Guide for 2026
Anesthesia CPT codes, found in the 00100 to 01999 range, are billed using a specific formula: (Base Units + Time Units + Modifying Units) x Payer Conversion Factor. Unlike fixed-fee procedural codes, every component of this formula—from the primary code to time increments and modifiers—must be meticulously documented and calculated to ensure accurate reimbursement. Mastering this calculation is the foundation of a financially healthy anesthesiology practice.
The Foundation of Anesthesia Reimbursement
Unlike most medical billing, where one CPT code equals one fee, anesthesia reimbursement is a moving target. Every component in that formula—base, time, and modifiers—has to be documented with precision. A mistake in any single part, whether it’s the wrong primary code or a miscalculation of time, leads straight to underpayments or denials.
The American Medical Association (AMA) maintains the CPT code set, but it’s the American Society of Anesthesiologists (ASA) that assigns a base unit value to each anesthesia code. This value is a direct reflection of the procedure's complexity, inherent risk, and the skill required from the provider.
The difference is stark when you compare procedures. A simple case has a low base value, while a complex, high-risk surgery commands a much higher one.
- CPT 00100: Anesthesia for procedures on salivary glands, assigned a base value of 5 units.
- CPT 00567: Anesthesia for a heart transplant, assigned a massive base value of 20 units.
This base unit is just the starting point. To get to the final billable amount, you have to add time units and any applicable modifying units before multiplying by the payer's conversion factor. It requires a deep knowledge of not just the procedures, but also the maze of payer-specific rules. For a deeper dive, you can learn more about specialized anesthesiology billing services that are built to handle these exact complexities.
According to CMS guidelines and AAPC analysis, improper coding is a leading cause of claim denials, responsible for a significant percentage of all rejected anesthesia claims. That's a staggering amount of revenue at risk from what might seem like minor errors. Mastering each piece of the anesthesia formula isn't just a best practice—it's a financial necessity.
Navigating the Anesthesia CPT Code Ranges
Anesthesia CPT codes, which live in the 00100-01999 range, aren’t just a random list of numbers. They’re meticulously organized by anatomical location, creating a logical map of the human body that’s your first defense against mismatched claims.
Think of it like this: the code set starts at the head and moves systematically down the body. By cross-referencing the surgical procedure’s location, your coder can immediately zero in on the correct anesthesia code block. Getting this right from the start prevents a cascade of downstream billing errors.
This structure is the first piece of the anesthesia billing formula, which ultimately determines your final payment.
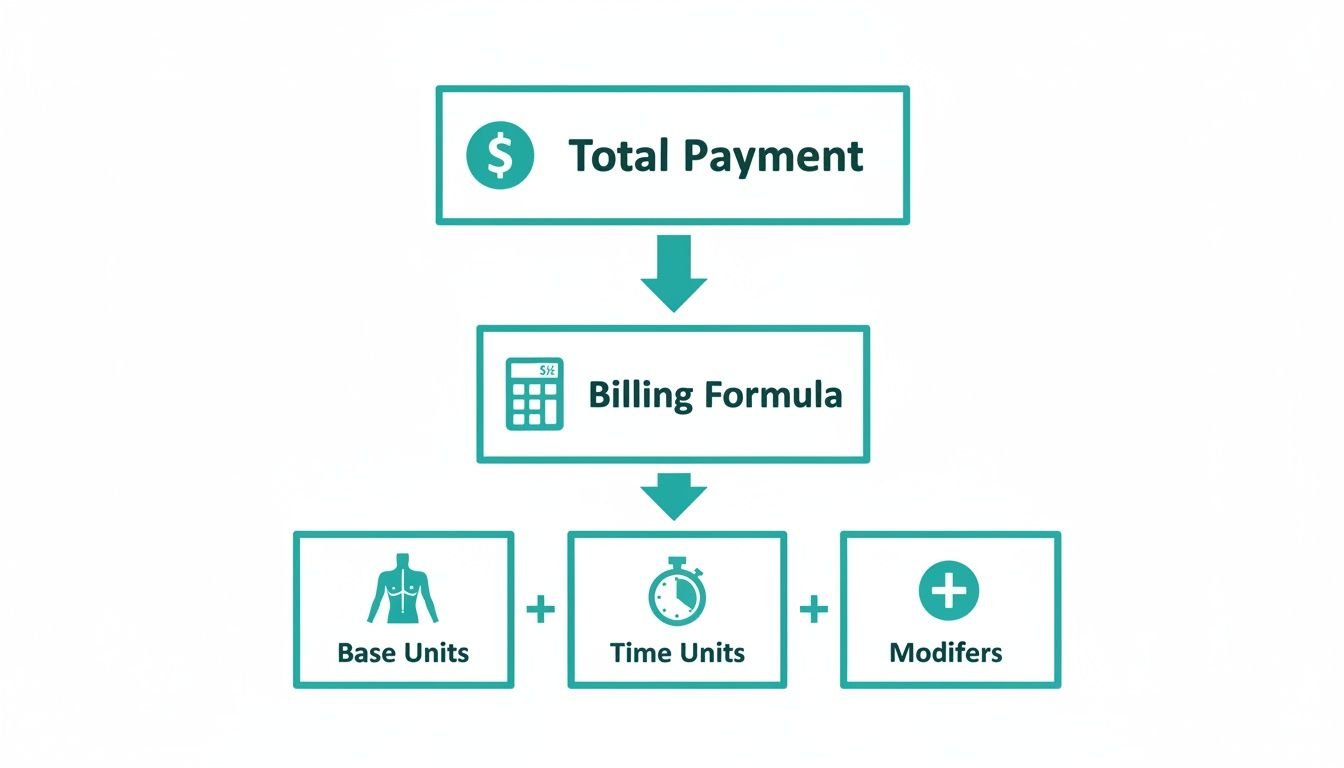
As you can see, total reimbursement hinges on correctly capturing not just the base procedure code but also all time units and applicable modifiers. Each component directly impacts your final payment, and a mistake in one can tank the value of the entire claim.
Anesthesia Code Ranges by Body Area
Mastering anesthesia billing starts with knowing how these codes are grouped. Here’s a high-level breakdown of the main categories you’ll work with inside the 00100-01999 series:
- Head (00100-00222): This range covers everything on the head, from intracranial work to procedures on the eyes, ears, nose, and throat. For example, CPT 00142 is for lens surgery, which is completely distinct from CPT 00170 for intraoral procedures.
- Neck (00300-00352): These codes are exclusively for procedures performed on the neck, such as thyroidectomies (CPT 00320) or radical neck dissections.
- Thorax (00400-00474): This section is for anesthesia involving the chest wall, pleura, and diaphragm. A partial pneumonectomy, for instance, uses CPT 00470.
- Intrathoracic (00500-00580): A highly complex and high-value category, these codes are for procedures inside the chest cavity. This is where you’ll find codes for open-heart surgeries like coronary artery bypass grafts (CPT 00566).
- Spine and Spinal Cord (00600-00670): Covering all spinal procedures from the cervical to lumbar regions. A common lumbar laminectomy, for example, would fall under CPT 00630.
- Upper Abdomen (00700-00797): Procedures on organs like the liver, stomach, and pancreas belong in this range.
- Lower Abdomen (00800-00882): This group is for surgeries on lower abdominal organs, including common procedures like appendectomies and hernia repairs.
- Perineum (00902-00952): These codes are specific to procedures on the perineum, often for urological and gynecological surgeries.
By starting with the anatomical location, you drastically narrow the potential CPT code choices. This simple step is critical for preventing the common, costly mismatches between surgical and anesthesia claims that lead to denials.
The Critical Need for Annual Code Updates
The CPT code set is not static; it changes every single year to keep up with new procedures and clinical practices. Using an outdated code isn't a small mistake—it's a guaranteed denial.
For example, the CPT 2026 update brought significant editorial changes, including new codes, deletions, and revisions. While the 00100-01999 range remains exclusive to anesthesia, any changes to the surgical codes have a direct ripple effect on how you bill for your services.
For any anesthesia practice, staying on top of these annual updates is non-negotiable. You can find a full overview of the 2026 CPT code set changes on agshealth.com.
Calculating Anesthesia Base and Time Units
The core of anesthesia billing isn't just one number; it's a formula. Getting paid correctly starts with nailing two critical inputs: base units and time units. While the math looks simple on paper, a small error in either part can silently drain thousands from your practice’s revenue each month.
Base units are the fixed value assigned by the American Society of Anesthesiologists (ASA) to every anesthesia CPT code. Think of it as the foundational risk and complexity score for a procedure. Then you have time units, which account for the duration of the anesthetic service. Getting the time capture right is just as vital as choosing the correct CPT code, as it often makes up the largest portion of the total billable units.
Understanding Anesthesia Base Units
Base units create a standardized starting point for valuing an anesthetic service. The difference between a low-risk procedure and a high-risk one is stark, and the base unit value reflects that gap from the get-go, ensuring more demanding cases are compensated appropriately.
Just look at these two examples:
- CPT 00100 (Anesthesia for procedures on salivary glands): This code carries a base value of 5 units, reflecting a relatively low-complexity procedure.
- CPT 00567 (Anesthesia for heart transplant): In contrast, this code is assigned a base value of 20 units, acknowledging the extreme skill, risk, and intensity involved.
A simple mismatch between the surgical CPT and the anesthesia crosswalk code can mean losing 15 base units before time is even factored in. This is a classic source of revenue leakage that meticulous pre-bill audits are designed to catch.
Calculating Anesthesia Time Units
Once you have the correct base unit, you have to calculate your time. The industry standard, which CMS and most commercial payers follow, is one time unit for every 15 minutes of anesthesia care. Be careful, though—some payers have their own rounding rules, so you always have to verify individual policies.
The real challenge is documenting exactly what counts as billable time. According to CMS guidelines, anesthesia time officially starts when the anesthesiologist begins preparing the patient in the operating room or an equivalent area.
This time officially ends when the anesthesiologist is no longer in personal attendance because the patient has been safely placed under post-anesthetic care.
That means time spent in the Post-Anesthesia Care Unit (PACU) is also billable right up until that handoff is complete.
Meticulous documentation of start and end times—down to the minute—is non-negotiable. Vague or missing time entries are a primary target for payer audits and a frequent cause for claim denials. Your anesthesia record must be an indisputable source of truth for every time-based calculation. As you can see, the intricacies go far beyond just codes; understanding these nuances is key, as we detail in our guide on medical billing complexities. Getting your team aligned on these definitions is critical for compliant and successful billing.
Getting Anesthesia Modifiers Right: A Guide for Compliant Billing
Anesthesia billing isn't like standard procedural coding. It's a different beast altogether, built on a formula where multiple parts have to work in perfect sync. While base units and time units lay the groundwork for a claim, it’s the modifiers that tell the full story, communicating specific circumstances that directly impact how much you get paid and whether you stay compliant. Getting these wrong is one of the fastest ways to trigger costly billing errors, claim denials, and painful payer audits.
Modifiers are essential for painting a complete picture of the service provided. For a quick overview, this table outlines the most common modifiers and their specific roles in anesthesia billing.
Common Anesthesia Modifiers and Their Usage
| Modifier | Description | When to Use |
|---|---|---|
| P1–P6 | Physical Status Modifiers: Indicate the patient's overall health and pre-operative risk. | Required on every anesthesia claim. Describes patient condition, from P1 (healthy) to P6 (brain-dead organ donor). |
| +99100–+99140 | Qualifying Circumstances (QC) Codes: Add-on codes for services performed in unusually difficult circumstances. | Used with a primary anesthesia code for factors like extreme age (+99100) or emergency conditions (+99140). |
| AA | Anesthesiologist Performed: Anesthesia services personally performed by an anesthesiologist. | When the anesthesiologist handles the entire case solo. Pays 100% of the fee schedule amount. |
| QK | Medical Direction: Anesthesiologist medically directs 2, 3, or 4 concurrent procedures. | Standard for care team models where an anesthesiologist oversees multiple CRNAs. |
| QX | CRNA Medically Directed: CRNA service performed with medical direction from an anesthesiologist. | Billed by the CRNA when working under an anesthesiologist in a QK scenario. |
| QZ | CRNA, No Direction: CRNA service performed without medical direction. | When a CRNA practices independently. Allows the CRNA to bill 100% of the allowable fee. |
Each of these modifier types serves a distinct, non-negotiable purpose. Let’s break down when and how to apply them correctly.
Defining Patient Health with Physical Status Modifiers
Physical Status (PS) modifiers, ranging from P1 to P6, are mandatory on every single anesthesia claim. They give payers a snapshot of the patient’s overall health at the time of surgery, which is a critical piece of the risk puzzle.
- P1: A normal, healthy patient.
- P2: A patient with mild systemic disease.
- P3: A patient with severe systemic disease.
- P4: A patient with severe systemic disease that is a constant threat to life.
- P5: A moribund patient who is not expected to survive without the operation.
- P6: A declared brain-dead patient whose organs are being removed for donor purposes.
While CMS doesn't add extra base units for these, many commercial payers absolutely do—especially for higher-risk patients (P3 and above). A payer might add one additional unit for a P3 status, two for P4, and three for P5. Forgetting to append the correct PS modifier is a guaranteed denial, but just as importantly, under-reporting patient severity means leaving earned money on the table.
Using Qualifying Circumstances Codes for Added Complexity
Don't mix these up with modifiers. Qualifying Circumstances (QC) codes are add-on CPT codes that you report alongside the primary anesthesia code when specific, challenging conditions arise. They exist to capture the increased difficulty and risk that the base units alone don't account for.
It's crucial to remember these are add-on codes, marked with a "+" symbol. That means they can never be billed alone. They must always accompany a primary anesthesia code from the 00100-01999 series.
Common QC codes include:
- +99100: Anesthesia for a patient of extreme age (under 1 year or over 70).
- +99116: Anesthesia complicated by total body hypothermia.
- +99135: Anesthesia complicated by controlled hypotension.
- +99140: Anesthesia complicated by an emergency. Payers like CMS define an emergency as a situation where delaying treatment would lead to a significant threat to life or a body part.
Your documentation must be rock-solid to support any QC code. If you bill for an emergency with +99140, the anesthesia record must explicitly describe the emergent nature of the procedure. For more in-depth examples, you can explore our other resources covering various anesthesia modifiers.
Specifying Provider Involvement with Pricing Modifiers
Pricing modifiers are absolutely essential for telling payers who performed the anesthesia service and under what level of supervision. These are especially vital for staying compliant with Medicare’s complex concurrency rules, which can make or break your reimbursement.
- AA: Anesthesia services performed personally by an anesthesiologist. This modifier secures 100% of the allowable fee.
- AD: Medical supervision by an anesthesiologist for more than four concurrent procedures. This results in a significant payment reduction.
- QK: Medical direction of two, three, or four concurrent anesthesia procedures. This is the standard for most care team models.
- QX: CRNA service with medical direction by an anesthesiologist. This is billed by the CRNA.
- QY: Medical direction of one CRNA by an anesthesiologist.
- QZ: CRNA service without medical direction by an anesthesiologist. This allows the CRNA to bill 100% of the allowable fee.
Applying these modifiers correctly isn't just a billing chore; it’s a compliance mandate that directly dictates your payment and audit risk. The sheer number of moving parts—base units, time, PS modifiers, QC codes, and pricing modifiers—is precisely why so many anesthesia practices leak revenue without even realizing it.
Stopping Common Anesthesia Coding Denials in Their Tracks
Even the sharpest anesthesiology practice will see claim denials. The real question is whether you have a strategy to stop the most common and costly errors before they ever leave your system. Preventing denials isn't just about getting paid faster; it's about plugging significant revenue leaks that quietly drain your practice’s profitability month after month.
The financial hit from bad anesthesia coding is staggering. In fact, improper coding is the root cause of nearly 25% of all anesthesia claim denials. For a mid-sized group that files 10,000 claims a year, that’s 2,500 claims that need to be reworked, resubmitted, and tracked by your staff. Targeting the source of these rejections is the only way to strengthen your revenue cycle and shrink your days in A/R.
Mismatched Anesthesia and Surgical Codes
One of the most frequent—and easily avoidable—denials comes from a mismatch between the anesthesia CPT code (00100-01999) and the surgical CPT code submitted by the surgeon. Payers don’t review these manually; their automated systems are built to cross-reference these codes. If the anesthesia service doesn't logically align with the surgical procedure, the claim gets an instant rejection.
For example, billing CPT 00790 (Anesthesia for intraperitoneal procedures in upper abdomen) for a surgical claim of CPT 58150 (Total abdominal hysterectomy) is a guaranteed denial. Why? Because the hysterectomy is a lower abdomen procedure. The correct anesthesia code would come from the lower abdomen range, like CPT 00840.
The Fix: Implement a mandatory pre-bill audit where every single anesthesia claim is cross-walked against its corresponding surgical code. This simple verification step ensures the codes match before the claim goes out the door, dramatically boosting your clean claim rate.
Incorrect Time Unit Calculation
Mistakes in calculating and documenting anesthesia time are another huge source of both denials and chronic underpayments. Billable anesthesia time isn't "skin-to-skin"—it starts the moment the provider begins preparing the patient and ends only when the patient is safely handed off to post-anesthetic care. Any vague or incorrectly documented start and end times are red flags for payer auditors.
Common time-related mistakes we see include:
- Rounding Errors: Incorrectly converting total minutes into 15-minute time units.
- Missing Documentation: Failing to clearly record both start and end times on the anesthesia record.
- Billing Surgical Time: Confusing the surgeon’s operating time with the full, billable anesthesia time.
These errors add up fast. Miscalculating by just 10 minutes on a few cases a day can easily translate into thousands of dollars in lost revenue over a year. A simple but powerful solution is using EHR templates that make start and end time fields mandatory.
Fixing these upstream issues is a core part of effective medical billing denial management.
Optimizing Your Revenue with a Specialized RCM Partner
Trying to manage the tangled rules of anesthesia CPT codes, modifiers, and time units is more than a full-time job—it's a constant drain on your practice's focus and profitability. Even with a sharp in-house team, just keeping up with payer whims, concurrency rules, and yearly code changes is a monumental task.
This is where a dedicated revenue cycle management (RCM) partner for anesthesiology isn't just an operational choice; it's a financial necessity.
A partner steeped in anesthesiology goes far beyond just submitting claims. They act as your financial defense, using a combination of smart technology and seasoned human expertise to guard your revenue. At Happy Billing, we match AI-powered claim scrubbing with hands-on audits by certified coders to hit a 98%+ first-pass clean claim rate. This one-two punch catches the expensive errors that software alone always misses.
Deep Expertise in Anesthesia Nuances
A general billing company might know CPT codes, but they almost never grasp the high-stakes details that define anesthesia reimbursement. An expert partner lives and breathes these nuances:
- Base Unit Validation: We make sure every claim starts with the correct anesthesia CPT code that crosswalks to the surgical procedure. This maximizes your base unit value right out of the gate.
- Modifier Accuracy: Physical status (P1-P6) and pricing modifiers (AA, QK, QX) must be applied flawlessly to reflect the real-world circumstances of care and satisfy strict payer rules. We get it right every time.
- Time Unit Precision: We verify that every billable minute of anesthesia time is captured and documented according to rigid CMS guidelines, from pre-op prep straight through to PACU handoff.
The bottom line is that a one-size-fits-all approach to billing is a recipe for failure in this field. Anesthesiology's entire formula—base units, time, and modifiers—demands a completely different RCM strategy than what works for cardiology or mental health.
Accelerating Cash Flow and Reducing Burdens
When you hand your billing over to experts, you immediately lift a massive administrative weight off your practice manager and clinical staff. They can finally get back to high-value work like patient scheduling, operational improvements, and strategic planning.
A specialized partner puts your cash flow on the fast track by slashing denials and aggressively working your A/R, turning complex claims into predictable income. To see how this works, you can learn about our dedicated anesthesia medical billing services and the way they fuel financial performance. This single shift turns your revenue cycle from a costly headache into a powerful engine for practice growth.
What Is the Difference Between Anesthesia Time and Surgical Time?
Anesthesia time is the total duration the anesthesia provider is medically responsible for the patient. According to CMS, it begins when the anesthesiologist starts preparing the patient in the operating room (or equivalent area) and ends only after the patient is safely placed under post-anesthetic care and the provider is no longer in personal attendance. Surgical time, defined by incision-to-closure, is irrelevant for anesthesia billing. Your reimbursement is based exclusively on accurately documented anesthesia time.
How Do I Bill for a Discontinued Procedure?
When a procedure is terminated after anesthesia induction, you must bill for the services rendered. Report the anesthesia CPT code for the originally planned procedure and append modifier -53 (Discontinued Procedure). Reimbursement is typically based on the full base unit value plus the time units accrued before the procedure was stopped. Your documentation must clearly state the medical reason for the cancellation to justify the claim.
How Is Monitored Anesthesia Care (MAC) Billed Differently?
Monitored Anesthesia Care (MAC) is billed using the same anesthesia CPT codes as a general anesthetic, but requires the QS modifier to be appended. Payers, particularly Medicare, enforce strict medical necessity criteria for MAC. The provider’s documentation must clearly articulate why the patient’s condition or the procedure’s complexity necessitated the presence of an anesthesia professional. Failure to provide this justification is a common reason for denial.
Managing the dense maze of anesthesia billing rules is a major drain on any practice. Happy Billing uses a powerful combination of agentic AI and expert human auditors to make sure every single base unit, time unit, and modifier is captured and coded correctly. We stop revenue leakage before it starts.
Operating right within your existing EHR, we deliver a 98%+ first-pass clean claim rate. This frees your team to focus on patient care, not fighting with payers. Explore how our specialized approach can transform your revenue cycle at happybilling.co.