Accounts Receivable in Medical Billing: A 2026 Guide
If your Days in A/R is over 50 days, your cash flow is already under strain. Accounts receivable (A/R) in medical billing is the outstanding revenue owed to a practice by payers and patients for services already delivered but not yet paid, and high-performance revenue cycle teams work to keep it under 35 days.
That definition sounds basic, but the operational reality isn’t. A/R isn’t just a balance sheet line. It tells you how fast your practice turns clinical work into usable cash, how often your claims leave the door clean, and where payer friction is stalling revenue.
For practice owners and managers, the biggest mistake is treating A/R as a back-office cleanup task. It’s a control system. If cardiology claims for CPT 93458 sit because documentation didn’t support the procedure level, if anesthesiology time reporting tied to CPT 00840 doesn’t align with modifiers and concurrency rules, or if behavioral health visits like 90837 go out without required authorization on file, your aging report will show the damage before your bank account does.
What Is Accounts Receivable in Medical Billing
Accounts receivable in medical billing is the total unpaid money your practice is still owed after services have been performed and claims or patient statements have been issued. That includes balances owed by commercial payers, government programs, and patients.
In practice, A/R is the financial lag between care delivered and cash collected. Every claim that’s pending, denied, underpaid, or waiting on patient payment sits inside that number. That’s why experienced operators don’t look at A/R as passive accounting. They treat it as an active measure of billing discipline.
A healthy A/R profile usually reflects strong front-end registration, accurate coding, fast charge entry, timely claim submission, disciplined follow-up, and patient billing that doesn’t create avoidable confusion. An unhealthy profile usually means at least one of those steps is breaking.
Why practice owners should care
A/R determines whether your revenue cycle is moving or dragging. If money stays tied up too long, payroll, vendor payments, staffing decisions, and growth plans all get harder.
You also lose advantage as claims age. Payers ask for records. Timely filing windows tighten. Appeal opportunities narrow. Staff stop working the highest-value accounts first and start reacting to whatever is loudest that day.
Practical rule: A/R should be managed like a clinical exception queue. The older the claim, the more expensive the recovery work becomes.
What A/R is not
It isn’t the same thing as charges. A high charge volume doesn’t mean you have strong collections. It also isn’t just an insurance problem. Patient responsibility now matters much earlier in the cycle, especially when front-desk staff don’t confirm coverage details, copays, or authorization requirements before the visit.
A/R is also different from accounts payable. Payable is what your practice owes others. Receivable is what others owe your practice.
For specialties with coding complexity, that distinction matters fast. In anesthesiology, modifier usage and time units can change reimbursement. In cardiology, procedural edits and documentation support can hold up payment. In mental health, missing prior authorization can convert a collectible claim into a preventable denial.
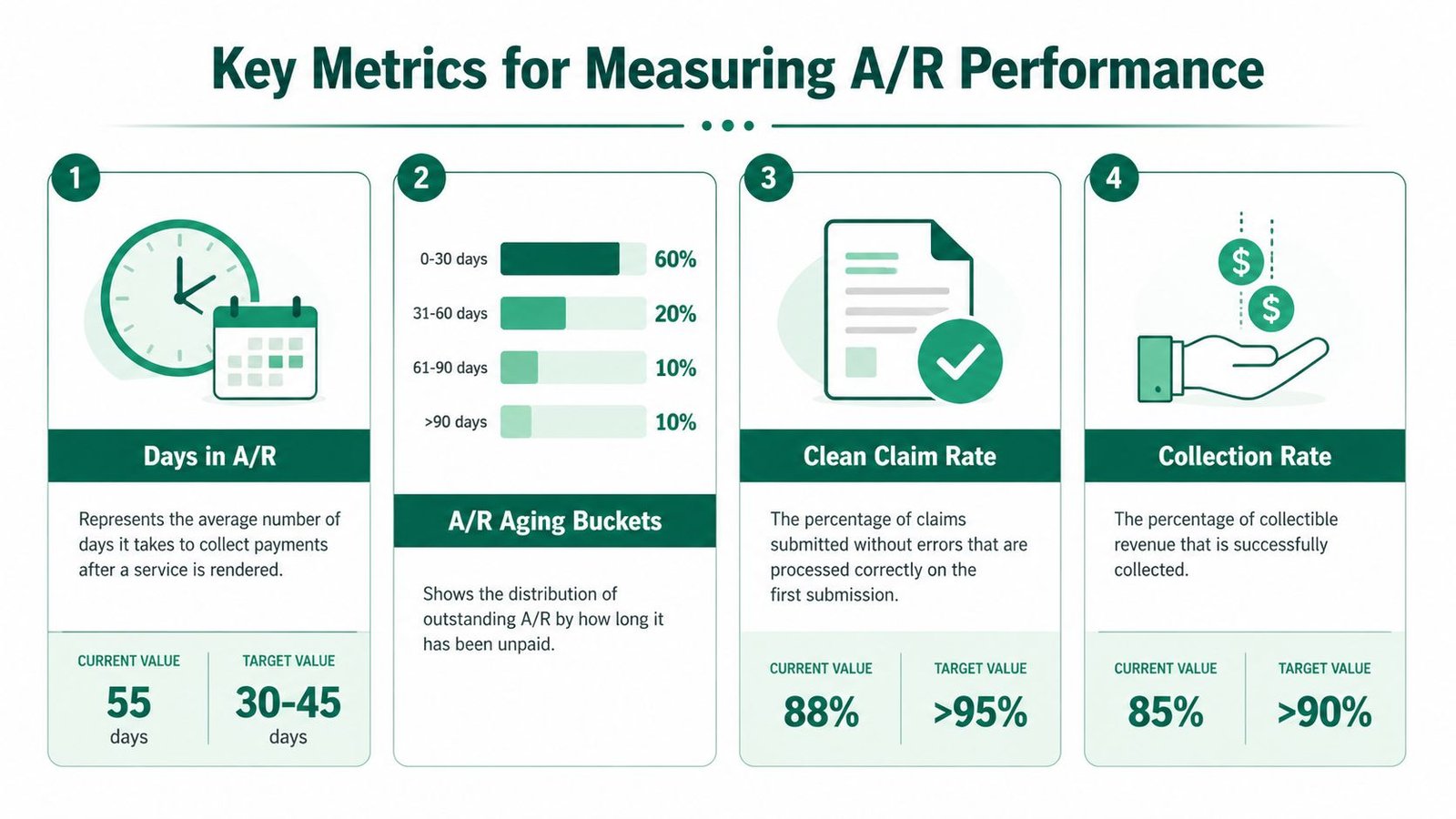
Key Metrics for Measuring A/R Performance
You can’t fix A/R by staring at total outstanding dollars. You fix it by measuring velocity, aging, and claim quality. The most useful metric is Days in A/R, because it tells you how long your practice takes, on average, to turn billed services into cash.
According to Plutus Health’s A/R metric overview, anything over 50 days signals significant cash flow issues, a practice with $500,000 in A/R and $3,000,000 in annual gross charges calculates to 60.8 days, high-performance RCM targets under 35 days, and over 25% of A/R in the 120+ day bucket usually points to serious denial or follow-up failures.
Days in A/R formula
The standard formula is:
Days in A/R = Total A/R ÷ (Gross Charges ÷ 365)
That formula matters because it normalizes your receivables against your production. Without it, a growing practice can mistake bigger A/R for better performance, when the opposite may be true.
Here’s how to read the result:
| Metric | What it tells you |
|---|---|
| Under 35 days | Strong cash conversion and disciplined follow-up |
| 35 to 50 days | Manageable, but likely hiding payer or process friction |
| Over 50 days | Material collection delay that needs operational correction |
If your number is high, don’t jump straight to “our biller is behind.” First check whether the slowdown starts before the claim is submitted.
Aging buckets show where the problem lives
An aging report is more diagnostic than total A/R because it separates balances by time bucket. Common buckets are 0-30, 31-60, 61-90, and 90+ days. The point isn’t just to see what’s old. The point is to ask why each payer, specialty, or claim type is sitting where it is.
Use aging buckets to segment by:
- Payer class: Commercial, Medicare, Medicaid, workers’ comp.
- Location: If one office has weaker eligibility verification, that pattern shows up.
- Provider: Useful when documentation style differs across physicians.
- CPT family: Office visits, anesthesia, cath lab, psychotherapy, imaging.
- Denial reason: Authorization, medical necessity, coding, bundling, missing records.
When teams skip this segmentation, they work accounts randomly. That creates activity, not recovery.
Claims in the oldest bucket rarely age there by accident. They usually sat untouched after a denial, a records request, or a coding correction that nobody owned.
Pair A/R metrics with payer rules
Measurement gets sharper when you line it up with actual payment expectations. The same Plutus Health analysis notes that Medicare enforces a 14-day minimum payment floor and interest on claims unpaid beyond 30 days, while commercial payer timeframes can be shaped by state prompt-pay laws such as Texas’s 30-45 day requirements.
That doesn’t mean every unpaid claim becomes a violation. It means your team should know when an account has crossed from normal adjudication time into avoidable delay. If your staff isn’t tracking payer-specific turnaround expectations, they’ll call too late, appeal too late, and escalate too late.
For practice managers building dashboards, medical billing KPIs to track should be tied to action. A metric without a work queue behind it won’t move cash.
Clean claims matter because rework creates aging
A/R starts deteriorating long before a claim hits the aging report. It starts when charge capture is delayed, diagnosis support is weak, modifiers are misapplied, or payer edits aren’t caught before submission.
In concrete terms:
- A cardiology claim for 93458 may suspend if documentation doesn’t support the selective catheterization and diagnostic components billed.
- An anesthesiology claim tied to 00840 can age if reported time units don’t match the anesthesia record or if concurrency-related modifiers don’t line up.
- A behavioral health claim for 90837 can stall immediately if the payer required authorization and the authorization data never made it onto the claim.
Those are coding and workflow issues first. A/R only shows you the bill after the mistake.
Uncovering Common Root Causes of A/R Backlogs
Most A/R backlogs aren’t caused by one dramatic failure. They build from small misses across the revenue cycle. A wrong member ID at registration. A coding edit nobody updated. A denied claim parked in a shared inbox. By the time the balance reaches an aging bucket that gets leadership attention, the recoverable work is already harder.

Front-end failures that create preventable A/R
The first root cause is weak intake discipline. If your team doesn’t validate demographics, coverage status, ordering provider details, referral requirements, or prior authorization before the visit, you’re feeding bad claims into the system on purpose.
The cost of “almost correct” registration is often underestimated by practice owners. A transposed insurance ID, the wrong payer sequence, an inactive plan, or a missing authorization number doesn’t always create an instant rejection. Sometimes the claim gets into adjudication, then stalls, then denies, then ages.
For example:
- Mental health claims such as CPT 90837 often depend on payer-specific authorization rules.
- Cardiology diagnostics may require order and medical necessity support that must be aligned before submission.
- Surgical follow-up services in orthopedics can age if staff don’t understand whether care falls inside or outside the global package.
According to BillFlash’s discussion of specialty-specific A/R issues, authorization lapses cause 25% of all behavioral health claim denials, and mismanaging the global period in orthopedics can inflate a claim’s A/R by 30% or more.
Mid-cycle coding errors that slow payment
Coding errors are the most misunderstood A/R driver because many practices only count hard denials. Suspended claims, underpayments, medical record requests, bundling edits, and modifier mismatches can all delay payment without showing up neatly as one denial category.
Take anesthesiology. If your team bills 00840 but the anesthesia time doesn’t reconcile with the record, or concurrency modifiers are missing or incorrect, the claim may not process cleanly. That’s not a follow-up problem. It’s a charge integrity problem.
BillFlash also notes that anesthesiology concurrency modifier denials can increase A/R days by 15-20%. That’s a specialty-specific issue, not a generic billing backlog.
In cardiology, a common pain point is procedure coding that doesn’t align with documentation and payer edits. A claim for 93458 can age because the cath report, diagnosis support, or modifier logic didn’t fully support what was billed. Modifier mistakes with 59, 25, or laterality-related coding patterns can produce bundling and payment delays even when the service was medically appropriate.
If a claim needs a coder, a biller, and a nurse to untangle what happened, that claim was already expensive before it ever aged.
Back-end follow-up failures that turn delays into write-offs
The back end breaks when denied or unpaid claims don’t have a clear owner, next action, and deadline. Too many teams still rely on spreadsheets, inboxes, and memory. That’s how claims cross filing limits or sit in “pending documentation” until nobody remembers why they were held.
Warning signs include:
- No payer-specific call scripts: Staff call without the claim number, denial code, or appeal basis ready.
- No next-touch date: Claims get worked once, then disappear.
- No denial categorization: Registration denials and coding denials get mixed together, so nobody fixes the source.
- No escalation path: Underpaid or repeatedly pended claims never move beyond routine follow-up.
A stronger medical billing denial management process separates root cause from resolution. Otherwise, your staff keeps “working A/R” without reducing it.
Proactive Strategies to Reduce Your Days in A/R
Reducing A/R starts before the claim exists. The most effective practices build controls at intake, coding, and claim release so the back office spends less time rescuing old balances and more time preventing them.

Tighten the front end before the date of service
Eligibility verification should be more than a same-day status check. Staff need to confirm active coverage, payer sequence, referral rules, authorization requirements, and whether the rendering provider is in network for that plan.
For behavioral health, that means reviewing authorization requirements before billing 90837, not after denial. Some teams verify coverage but forget to verify whether the payer approved the service frequency, visit count, or provider type. That’s how clean-looking claims become aged claims.
Front-end discipline works best when you hardwire a short checklist:
- Verify subscriber and member identifiers exactly
- Confirm payer-specific authorization rules
- Match rendering and billing provider data
- Collect patient responsibility early
- Document verification results inside the PM or EHR system
When those steps happen outside the system, they don’t scale. Staff leave notes in email, paper, or memory, and the billing team inherits uncertainty.
Scrub claims with specialty logic, not generic edits
A generic claim scrubber will catch missing fields. It won’t always catch the mistakes that matter most in specialty billing.
Anesthesiology needs edits around time documentation, units, modifier sequencing, and concurrency support. Cardiology needs edits for procedural combinations, diagnosis support, NCCI logic, and documentation alignment. Behavioral health needs authorization validation and payer-specific frequency rules. Orthopedics needs review of global periods and modifier use such as 59 when separate procedural services are appropriately supported.
That’s the difference between simple automation and useful automation. The best edit rules are built from your own denial history.
A practical review queue should include:
- Claims with missing modifiers
- Claims with diagnosis-to-procedure mismatches
- Claims involving known payer edits
- Claims missing authorization identifiers
- Claims held for documentation but not yet released
Operational advice: Don’t ask whether the claim can be submitted. Ask whether the claim can be paid without human rescue.
Build a follow-up cadence around claim risk
Not every unpaid claim deserves the same attention. Teams reduce A/R faster when they prioritize by age, balance, denial reason, and filing-limit risk.
A useful work pattern looks like this:
| Claim type | Best immediate action |
|---|---|
| Rejected at clearinghouse | Correct and resubmit same day |
| Denied for authorization | Validate if retro review or appeal is possible |
| Pending medical records | Send records with documented confirmation |
| Underpaid by payer | Compare EOB/ERA against expected contract terms |
| No response within expected window | Contact payer and document reference number |
Here, Days in A/R management practices become operational, not theoretical. If your team works old balances in arbitrary order, you’ll stay busy and still watch cash lag.
Fix the root cause, not just the account
Every appealed or corrected claim should feed a process correction upstream. If a cardiology claim for 93458 denied because the operative report didn’t support what was billed, the solution isn’t just rebilling. It’s tightening coder review criteria and provider documentation expectations. If anesthesia claims tied to 00840 repeatedly stall on modifier logic, build a pre-bill audit for those scenarios.
The same applies to mental health. If denials keep tracing back to authorization lapses on 90837, assign ownership before the appointment, not after adjudication. Revenue cycle performance improves when responsibility sits with the team closest to the cause.
One option some groups use is a specialty-focused RCM partner that works inside the existing system and applies payer-specific edits by specialty, including service lines listed on Happy Billing’s specialty pages. The decision matters less than the operating model. Whatever route you choose, the workflow must connect front-desk verification, coding review, and denial follow-up into one accountable process.
Leveraging Technology and Workflows for A/R Follow-Up
Manual A/R follow-up usually looks productive from a distance. A staff member exports a spreadsheet, sorts by oldest date, opens payer portals one by one, calls when time allows, and adds notes in multiple places. Hours pass. Very little moves.
A modern workflow looks different because it treats follow-up as exception management. Instead of asking staff to scan every account, the system builds work queues based on claim age, payer, balance, denial type, and next action date. The specialist starts the day with a ranked list instead of a blank screen.
What a stronger workday actually looks like
An A/R specialist logs in and sees separate queues for:
- Clearinghouse rejections needing same-day correction
- Claims approaching filing limits
- Medical record requests
- No-response claims beyond payer turnaround expectations
- Denials grouped by root cause
That one change matters. It stops staff from spending the morning on low-value account notes while higher-risk balances continue to age.
The best teams also document every payer touchpoint inside the billing platform, not in side spreadsheets. Reference numbers, portal screenshots, denial codes, rep names, and promised timeframes all stay attached to the claim. When a second specialist picks up the account, they don’t restart the investigation.
Workflow beats raw effort
Technology helps only when the workflow is tight. A claim queue without ownership rules becomes another list nobody trusts.
Here’s a workable model:
- Route by exception type so coding issues go to coding, auth issues go to auth staff, and underpayments go to contract review.
- Set next action dates on every unresolved account.
- Use payer-specific scripts so calls start with the right identifiers and appeal basis.
- Track outcome categories so leadership can see which denials are operational failures versus payer friction.
A good analytics layer then shows whether one payer is delaying cardiology procedure claims, whether one location has repeated demographic errors, or whether one provider’s documentation is creating more edits than the rest. That’s where revenue cycle analytics tools become useful. They help managers direct labor toward the claims most likely to convert into cash.
The goal of A/R follow-up isn’t more touches. It’s fewer touches per paid claim.
Evaluating an RCM Partner for A/R Recovery
Some practices should keep A/R management in house. Others should not. The right answer depends on whether your internal team can control specialty-specific denials, maintain disciplined follow-up, and convert services into cash without constant firefighting.
Signs your current model isn’t working
A practice should seriously review its operating model when:
- Days in A/R stays above internal targets
- Old balances keep growing instead of clearing
- Denials repeat for the same reasons
- Billing staff spend most of their time reacting
- Specialty claims require constant rework before payment
That last point matters most. If your anesthesiology claims repeatedly stall on time-unit and modifier issues, if cardiology procedures need repeated appeals because of coding-documentation mismatches, or if mental health claims keep denying for authorization reasons, you don’t have a staffing problem alone. You have a specialty process problem.
What to ask a potential partner
A real evaluation should focus on operating details, not marketing language. Ask:
| Question | Why it matters |
|---|---|
| Do you have specialty-specific coding depth? | Generic follow-up teams miss claim-level nuances |
| Can you work inside our current EHR and PM? | System disruption can create more A/R before it reduces it |
| How do you segment follow-up work queues? | Queue logic determines recovery speed |
| Who owns denials by category? | Ownership prevents claims from stalling |
| What reporting will we receive? | Transparency shows whether root causes are actually being fixed |
You should also ask for a walkthrough of how they’d handle one anesthesia claim, one cardiology procedural claim, and one behavioral health authorization denial. If they answer only in generalities, keep looking.
A side-by-side review of in-house vs outsourced medical billing is useful here because the trade-off isn’t just cost. It’s control, speed, specialty expertise, reporting quality, and how much management time your internal team is burning to keep collections moving.
The trade-off owners often miss
Outsourcing isn’t automatically better. A disciplined in-house team with strong edits, tight workflows, and clear ownership can outperform a weak vendor. But a vendor with specialty expertise can outperform an internal team that’s stretched thin and working old balances manually.
The deciding question is simple. Can your current model prevent denials upstream and recover aged claims without leadership intervening every week? If not, that gap will keep showing up in your A/R.
Frequently Asked Questions About Medical A/R
What is a good Days in A/R target for a medical practice
A practical target is to keep Days in A/R under 35 days. Once it moves over 50 days, you’re usually dealing with meaningful friction in claim quality, payer follow-up, or both. The exact root cause depends on specialty, payer mix, and how clean claims leave your system, but the number is useful because it forces operational accountability.
How much old A/R is too much
If more than 25% of your A/R sits in the 120+ day bucket, that usually points to severe denial or follow-up failures, as noted earlier from the Plutus Health benchmark. At that point, you shouldn’t just intensify calls. You should separate recoverable balances from process failures and identify where ownership broke.
What is the difference between accounts receivable and accounts payable
Accounts receivable is money owed to your practice for services already delivered. Accounts payable is money your practice owes to vendors, staff, or other parties. In revenue cycle terms, receivable measures how efficiently you collect. Payable measures how you manage outgoing obligations.
How can one modifier mistake increase A/R
A single modifier error can trigger bundling edits, underpayment, or full denial. In anesthesiology, concurrency-related modifier issues can delay adjudication and materially increase aging. In procedural specialties, misuse of modifiers such as 59 or 25 can cause claims to pend, deny, or require manual review. The claim may still be collectible, but it now takes extra touches, extra days, and often extra documentation to get paid.
If your practice is stuck with aging claims, repeat denials, or specialty-specific coding friction, Happy Billing is one option to evaluate. The team works inside existing systems, supports specialty-specific RCM workflows, and focuses on reducing A/R through cleaner claims, tighter denial prevention, and structured follow-up.