Optimize Medical Billing for Mental Health Practices

Medical billing for mental health is a specialized revenue process built around time-based CPT codes, strict authorization controls, and narrative documentation that has to prove medical necessity. It also became more operationally demanding as telehealth mental health visits rose from about 1% before 2020 to more than 32% in the first half of 2022, which changed payer rules and expanded virtual billing pathways while adding new compliance points to monitor. The choice between the two most-billed session codes, 90837 vs 90834, is where many of these denials begin.
If you’re managing a behavioral health practice, you’ve probably seen the same pattern. The therapist delivered the session. The note exists. The diagnosis is real. The claim still comes back denied, underpaid, or parked in A/R because the payer wanted the claim routed to a behavioral carve-out, the authorization expired, or the note didn’t support the level billed.
That’s what generic billing advice misses. Medical billing for mental health isn’t just standard physician billing with different CPT codes. It runs on a different financial architecture. Session length drives code selection. ICD-10 and, in many workflows, DSM-5 shape medical necessity logic. Payers often require approvals at multiple stages. Narrative notes affect payment more directly than many practice managers expect. And upcoming 2026 ICD-10 SDoH coding updates will push even more reimbursement logic into the documentation-to-coding handoff.
What Is Medical Billing for Mental Health
A lot of practice managers first define the problem the wrong way. They assume denials happen because staff missed a field, chose the wrong code once, or didn’t post payments fast enough. Those things matter, but in mental health billing the bigger issue is that the payer is evaluating a clinical story, not just a transaction.
Mental health billing uses procedure codes, of course, but payment often depends on whether the chart shows why that service level was necessary for that patient on that date. That’s why a claim can be technically complete and still fail. The documentation, diagnosis pairing, authorization status, and payer routing all have to line up.
Why this specialty behaves differently
Behavioral health billing stands apart from most procedure-heavy specialties for three practical reasons:
- Time drives payment: A psychotherapy visit isn’t billed the same way as a discrete procedure. The difference between 90832, 90834, and 90837 can come down to documented session duration and whether the note supports that level.
- Narrative proof matters: Payers look for symptoms, impairment, treatment goals, and clinical rationale. In many practices, the progress note is the strongest billing document.
- Benefits are fragmented: The patient’s insurance card may name one payer, but behavioral health services may have to go to a separate managed behavioral health organization.
Practical rule: If your front desk, clinicians, and billers are each working from different assumptions about payer rules, you don’t have a billing process. You have three partial workflows that collide after the claim is denied.
Most clinics don’t need more generic advice about clean claims. They need tighter operations around authorizations, time capture, documentation standards, and payer identification. That’s the difference between chasing denials and preventing them.
For a deeper operational view, the best starting point is a specialty-specific workflow for mental health revenue cycle management.
Core Codes That Drive Mental Health Reimbursement
Mental health reimbursement starts with code discipline. If your team treats psychotherapy coding as “close enough,” the payer usually won’t.
The codes most practices use every day
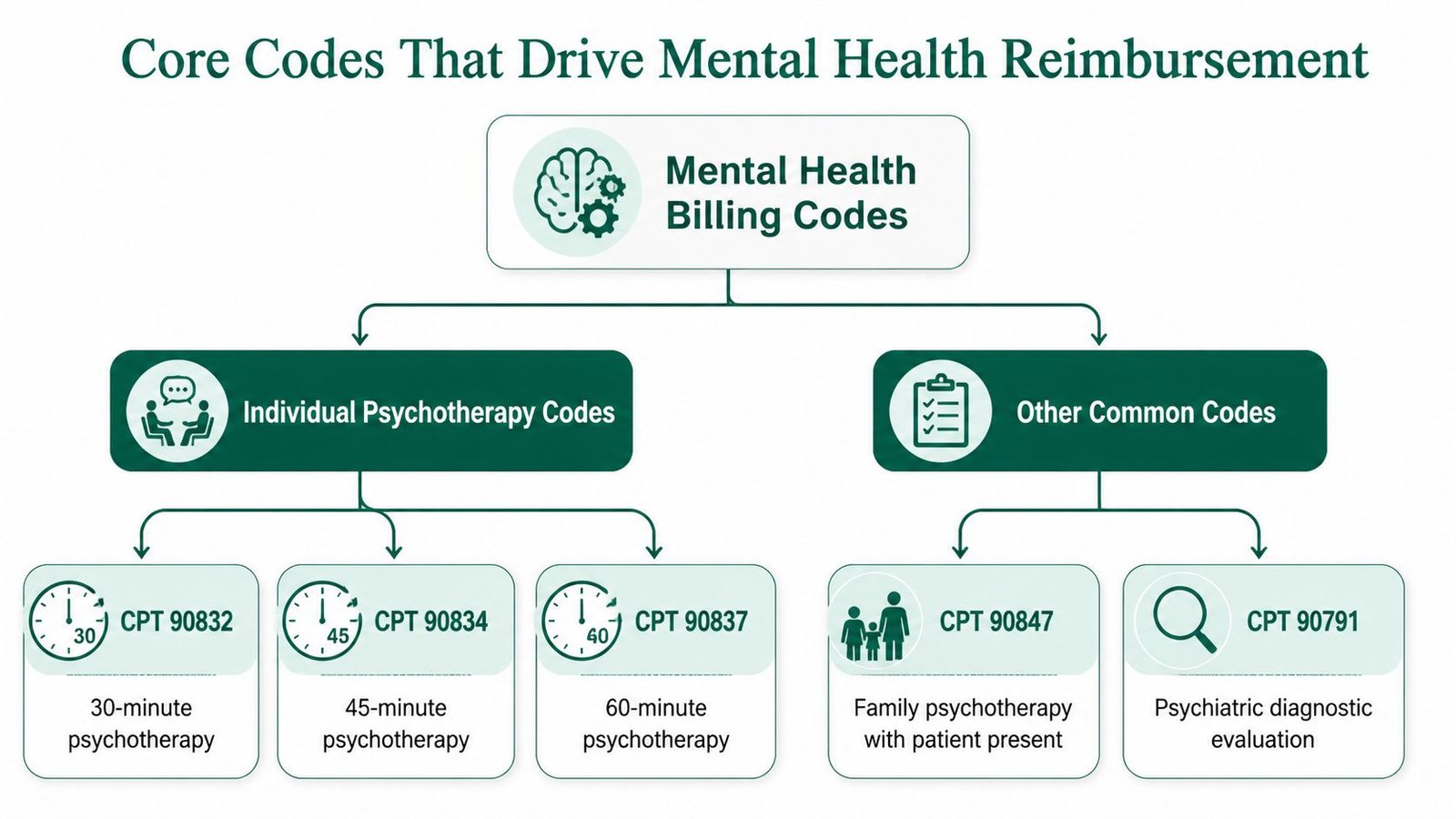
The backbone of outpatient mental health billing usually includes:
- 90791 for psychiatric diagnostic evaluation
- 90832 for 30-minute psychotherapy
- 90834 for 45-minute psychotherapy
- 90837 for 60-minute psychotherapy
- 90853 for group psychotherapy
- 96130 and 96132 for psychological testing services
- 90839 and 90840 for crisis psychotherapy
Those aren’t interchangeable. They each carry their own documentation burden, and psychotherapy codes in particular depend on precise time support in the chart.
Industry guidance summarized by iMed Claims on mental health billing services notes that mental health billing operates on a different model because reimbursement is tied to session duration intervals, and a mismatch between documented time and the CPT billed can trigger denial cascades. The same source also notes that practices not achieving a clean claim rate above 90% often see significantly extended A/R, with the benchmark goal being under 40 days.
The code has to match the diagnosis story
Many practices lose money because while they focus on selecting the right CPT, the payer is also checking whether the ICD-10-CM diagnosis supports the billed service level. In behavioral health, diagnoses often live in a workflow shaped by DSM-5 alongside ICD-10, which adds complexity compared with specialties that work more narrowly from diagnosis-to-procedure logic.
A few practical examples:
| Service pattern | Code concern | Revenue risk |
|---|---|---|
| Individual psychotherapy note supports a shorter session | 90837 billed instead of 90834 or 90832 | Denial or downcoding |
| Group session documented but billed as individual | 90853 omitted | Wrong code, payment delay |
| Psychological testing performed without proper testing code set | 96130/96132 not used correctly | Underbilling or rejection |
| Crisis work documented without crisis code support | 90839/90840 not justified | Missed reimbursement |
The problem isn’t only “wrong code.” It’s unsupported code.
A payer’s editing logic often asks two questions before a human ever touches the claim: did the documented time support the CPT, and did the diagnosis support the medical necessity of that service level?
That’s why code review should happen before submission, not after remittance. Practices that need a detailed breakdown of psychotherapy coding can use this guide to CPT 90837 vs 90834.
Modifiers and telehealth signals still matter
Even in a code-focused section, it’s worth stating one operational truth. The CPT may be correct, but if the service was delivered remotely and the payer expected modifier 95 or a telehealth place-of-service indicator, the claim can still fail. In behavioral health, code selection and claim construction have to work together.
Mastering the Prior Authorization Workflow
Many behavioral health denials are created before the first claim is filed. The visit occurs, the note is signed, the claim goes out, and only then does the practice discover the sessions were never authorized, the approved unit count was exhausted, or the diagnosis on the request didn’t match the diagnosis on the claim.
What a working authorization process looks like
A reliable authorization workflow has to do more than confirm coverage. It should answer six operational questions before the patient is seen:
Is outpatient mental health carved out?
Check whether the medical insurer administers benefits directly or routes them to an MBHO.Does the plan require prior authorization?
Don’t assume recurring therapy is exempt. Many plans want approval by service type, diagnosis, or episode stage.What exactly was approved?
Capture the authorization number, service category, code set if available, session count or units, and date span.Who is approved to render the service?
Make sure the rendering provider is credentialed correctly and linked to the payer or delegated entity.When will the authorization expire?
Expiration-based denials are common because the patient keeps attending and no one rechecks the date range.How will used visits be tracked?
If the plan approved a limited number of sessions, your scheduler and billing team need a shared ledger.
What breaks in real clinics
The biggest weakness I see is handoff failure. Front office staff verify benefits. A coordinator requests authorization. Clinicians keep the patient on the calendar. Billing learns the authorization lapsed only after the ERA posts.
That’s fixable if the practice runs one shared process instead of departmental fragments. Keep an internal tracker that records:
- Payer entity: medical insurer or MBHO
- Approved service type: psychotherapy, testing, crisis, other covered category
- Approved period: start and end dates
- Session usage: visits completed against approved total
- Renewal trigger: internal reminder before exhaustion or expiration
If your staff can’t answer “How many sessions are left under this auth?” in under a minute, your process is too loose.
You don’t need a complicated platform to start tightening this. You need ownership, a shared work queue, and a pre-visit checkpoint tied to scheduling. For a practical framework, review this breakdown of prior authorization in healthcare.
Navigating Telehealth and Digital Care Billing Rules
Virtual behavioral health isn’t a side channel anymore. It’s part of the operating model, and billing teams need to treat it that way.
Telehealth visits for mental health rose from around 1% prior to 2020 to more than 32% in the first half of 2022, and Medicare responded by extending home-based telehealth and audio-only coverage while reimbursing teletherapy codes like 90834 and 90837 at the same rates as in-person care and removing prior geographic restrictions, as described in this review of behavioral health billing trends for 2025.
The claim has to show how the service was delivered
For teletherapy, the billing risk usually isn’t the psychotherapy CPT itself. It’s the service configuration. Your team needs a consistent rule set for:
- Place of Service 02 for telehealth provided other than in the patient’s home
- Place of Service 10 for telehealth provided in the patient’s home
- Modifier 95 when the payer requires a synchronous audio/video indicator
Some payers also have their own telehealth formatting rules, but the point is operationally simple. If the service was remote, the claim has to make that visible in the format the payer expects.
Audio-only and home-based care require policy discipline
CMS policy changes made remote mental health billing more workable, especially for home-based and audio-only care. But “covered” doesn’t mean “bill it however you want.” Your staff should confirm, for each payer:
| Billing question | Why it matters |
|---|---|
| Was the session audio/video or audio-only? | The payer may treat them differently |
| Where was the patient located? | POS selection affects adjudication |
| Was home-based telehealth allowed? | Not every payer mirrors Medicare |
| Did the note reflect remote delivery? | Missing delivery details can create compliance issues |
The practical mistake is assuming telehealth parity solved the workflow. It solved some reimbursement barriers. It did not eliminate modifier logic, payer variance, or documentation requirements tied to remote care.
A useful operations checklist for hybrid practices is this guide on telehealth billing for mental health.
Why Documentation Is Your Best Denial Prevention Tool
Most practices treat documentation as a compliance task and billing as an administrative task. In mental health, that separation doesn’t work. The note is often the strongest evidence that the claim deserves payment.
What payers want to see in the note
According to the guidance in this mental health billing documentation article from ICANotes, inadequate clinical documentation supporting medical necessity is the highest-impact denial driver in mental health billing. That source also states that payers want progress notes to link interventions to treatment goals and justify the billed service level, and that vague records are a leading cause of denials, delays, audit risk, and clawbacks.
In practical terms, a strong note usually does three jobs at once:
- It identifies symptoms and functional impairment
- It ties the intervention to an active treatment plan
- It explains why the billed level fits the session
If you bill 90837, the note should support a full 60-minute psychotherapy service, not just prove that the patient showed up.
Weak notes versus billable notes
Here’s the difference that matters.
Weak phrasing:
“Met with patient. Discussed stress, family conflict, and coping skills. Will continue therapy.”
That may be clinically familiar, but it gives the payer very little. It doesn’t show severity, impairment, treatment-plan linkage, or why the level billed was medically necessary.
Stronger phrasing:
“Patient reported persistent depressive symptoms with impaired concentration, reduced work performance, and increased social withdrawal. Session focused on cognitive restructuring and behavioral activation interventions tied to treatment goal of improving daily functioning and reducing avoidance. Session duration and intervention intensity supported ongoing individual psychotherapy at the billed level.”
That kind of language gives billing and compliance teams something to defend.
Good mental health documentation doesn’t read like billing language. It reads like clinical care that clearly explains why this patient needed this service at this level on this date.
Documentation controls that actually help revenue
The most effective documentation improvements are usually simple:
- Use diagnosis-specific templates: Not canned notes, but prompts that pull symptom severity, impairment, and treatment-goal linkage into the record.
- Require time support: If the service is time-based, the note needs time clarity.
- Audit before claim submission: Spot-check higher-risk claims such as 90837, crisis services, and testing codes.
- Train clinicians on denial triggers: Many providers don’t realize that vague phrasing can sink a correctly coded claim.
When practices want fewer denials, they often ask billing to work harder. In mental health, the better answer is usually to make the note more billable.
Common Denials and How to Fix Them
The most expensive denials in mental health billing usually aren’t mysterious. They repeat. Once you know the pattern, you can design them out of the workflow.
One of the biggest examples is the MBHO carve-out problem. Many commercial plans, including plans associated with Cigna and UnitedHealthcare, may route behavioral health through entities such as Magellan or Optum, and claims have to be sent to the behavioral health organization rather than the primary insurer listed on the patient card, as explained in this article on mental health billing for small group practices. That routing error is a common reason valid claims get denied or delayed.
Common Mental Health Billing Denial Codes and Fixes
| Denial Reason / Code | What It Really Means | How to Fix It |
|---|---|---|
| Wrong payer | You billed the medical carrier, but behavioral health is carved out to an MBHO | Reverify benefits, identify the behavioral payer, update payer routing, and refile to the correct entity |
| Service not authorized | The plan required authorization, or the approved sessions/date span were exceeded | Obtain retro guidance if allowed, confirm auth details, and implement visit tracking before future sessions |
| Medical necessity not supported | The note didn’t justify the diagnosis, treatment intensity, or service level | Audit the chart, strengthen treatment-goal linkage, and appeal with corrected documentation if payer rules permit |
| Time-based code mismatch | The documented session length doesn’t support the CPT billed | Recode to the supported service level when appropriate and retrain clinicians on session-time documentation |
| Telehealth formatting issue | Required POS or modifier detail was missing or inconsistent | Correct POS 02 or 10, add modifier 95 when required, and refile according to payer telehealth rules |
| Provider enrollment issue | The rendering clinician wasn’t properly credentialed or linked | Confirm credentialing, CAQH updates, payer setup, and rendering/billing provider configuration |
The carve-out denial is operational, not clinical
Staff often waste time appealing the wrong issue. If a claim hit the wrong payer, the denial isn’t about diagnosis, coding, or note quality. It’s a routing problem. Fix it at intake and benefits verification.
The best way to reduce these denials is to require a behavioral health-specific verification script that asks:
- Who administers outpatient mental health benefits?
- Where should claims be submitted?
- Does this plan use a separate authorization process?
- Is the rendering provider credentialed with that entity?
When a payer outsources mental health benefits, your claim follows the delegated contract, not the logo on the insurance card.
For practices that need a stronger workflow for appeals and rework, this guide to medical billing denial management is a practical reference. If you’re evaluating specialist support by service line, you can also review the Happy Billing specialties page.
The Decision Framework for Outsourcing Your RCM
Outsourcing mental health billing shouldn’t be framed as “Do we want outside help?” The better question is whether your current team can consistently manage time-based coding, behavioral authorizations, carve-out routing, telehealth claim construction, and documentation-backed appeals without slowing collections.
Start with the economics
Mental health billing companies typically charge 6% to 8% of collections for therapy practices, and for a practice collecting $500,000 annually, a 7% fee equals $35,000, while in-house billing often runs $40,000 to $60,000 once salary, benefits, software, and revenue leakage are included, according to this review of mental health medical billing company pricing.
That doesn’t mean outsourcing is always right. It does mean many owners underestimate the cost of “keeping it in-house.”
The practical scorecard
Ask your team five direct questions:
Are claims leaving the door clean?
If the practice is seeing repeat edits around time-based psychotherapy codes, diagnosis mismatches, or telehealth formatting, capacity may already be stretched.Can staff manage behavioral authorizations proactively?
If session limits are being discovered after denial, the process is reactive.Are clinicians producing billable documentation consistently?
If appeals depend on rewriting notes after the fact, the workflow is unstable.Can your team manage carve-outs and credentialing nuance?
Behavioral health payer structures are less forgiving than many medical specialties.Do you know your internal cost with confidence?
Include salary, benefits, clearinghouse fees, software, management time, and the value of denials that no one works thoroughly.
What a specialist partner should be able to deliver
This isn’t about outsourcing for its own sake. It’s about whether the partner is built for behavioral health complexity.
Look for an RCM partner that can show:
- Behavioral-health-specific authorization controls
- Strong first-pass discipline on psychotherapy claims
- Documentation review tied to medical necessity
- Telehealth billing competence
- Credentialing and payer-routing expertise for carve-outs
Some specialized RCM firms report 98%+ clean claims and under 35 days in A/R when workflows are designed around these exact pain points, particularly in behavioral health environments with tight pre-submission review and denial prevention processes. That standard is worth using as a comparison point when you evaluate vendors or your own internal operation.
FAQs About Medical Billing for Mental Health
How do I know whether a mental health claim should go to the main insurer or an MBHO
Don’t rely on the insurance card alone. Verify benefits and specifically ask who administers outpatient behavioral health. If the plan delegates mental health to an MBHO such as Magellan, Carelon Behavioral Health, Optum Behavioral Health, or ValueOptions, send the claim there and follow that entity’s authorization rules. This is one of the most common avoidable denial sources in medical billing for mental health.
Which CPT codes matter most for a therapy-focused practice
For most outpatient therapy groups, the highest-volume codes are 90791, 90832, 90834, 90837, and 90853. Testing and crisis work may also bring in 96130, 96132, 90839, and 90840 depending on the service mix. The main operational rule is simple: the note, diagnosis, and documented session duration must all support the billed code.
What should I track every week if I manage the revenue cycle internally
At minimum, track first-pass claim acceptance, days in A/R, denial categories, authorization status by active patient, and payer turnaround patterns. In mental health, I’d also add a documentation audit queue for higher-risk codes and a payer-routing check for new commercial patients. If you can’t see those trends quickly, denials will stack up before anyone knows where the leak started.
How do the 2026 ICD-10 SDoH updates affect mental health billing
The operational change is documentation-driven. As 2026 ICD-10 updates bring more attention to social determinants of health coding such as housing instability, financial strain, transportation access, and food insecurity, clinicians and billers need a cleaner handoff so social context documented in the note becomes coded data when payer policy supports it. In value-based environments, that can affect risk adjustment and reimbursement alignment. The mistake is waiting until claim submission to look for SDoH details that were never captured in the chart.
Happy Billing helps behavioral health practices tighten the exact workflows that cause the most revenue leakage in medical billing for mental health, including authorizations, psychotherapy coding, carve-out routing, documentation review, denial management, and A/R recovery. If your team wants a specialist partner that works inside your existing systems and focuses on faster cash flow with fewer preventable denials, visit Happy Billing.