Occipital Block CPT Code 2026 Mastery Guide
CPT 64405 is the occipital block CPT code for a greater occipital nerve block. Accurate billing doesn’t stop there. You also need 64450 for a lesser occipital nerve block, modifier 50 for bilateral greater occipital blocks, and tight control over frequency because claims that exceed three injections per anatomic site in six months are denied by Medicare.
That’s the counterintuitive part. Most denials don’t happen because staff forgot 64405. They happen because the note never clearly identifies whether the physician blocked the greater occipital nerve, the lesser occipital nerve, or both. In occipital block billing, anatomy drives code selection, modifier choice, and payer review.
For anesthesiology and pain practices, this is a high-risk revenue cycle category. The procedure looks simple clinically. It isn’t simple financially. A claim that says “occipital nerve block” without nerve-specific documentation invites payer edits, bundling disputes, and medical necessity challenges.
Decoding Occipital Block CPT Codes Correctly
The phrase occipital block cpt code is misleading because there isn’t one universal code for every occipital nerve injection. There are different codes depending on which nerve was treated. If your providers document “occipital block” and stop there, your billing team is forced to guess. That’s how denials start.
The first rule is straightforward. CPT 64405 is for the greater occipital nerve. The lesser occipital nerve is a different coding path, and payers such as Anthem identify 64450 for therapeutic lesser occipital nerve blocks. That distinction matters because the two nerves are anatomically separate even though they’re close to each other.
Recent background discussed in this anesthesia CPT coding resource aligns with what experienced pain billing teams already know. Claims become vulnerable when documentation fails to specify the exact nerve treated, and ambiguous peripheral nerve block claims have been associated with 20-30% denial rates in industry benchmarks cited in occipital block coding analysis (Aneskey occipital nerve blocks review).
The coding rule your team should enforce
Use this internal rule across scheduling, charge capture, and claim scrub:
- If the physician documents greater occipital nerve, code 64405
- If the physician documents lesser occipital nerve, code 64450
- If both are blocked, treat them as two distinct nerves and bill accordingly with the right modifiers and medical necessity support
- If the note says only “occipital nerve block”, query the provider before claim release
Practical rule: Never let “occipital block” stand alone in the final signed note. Force the chart to identify GON, LON, or both.
That one workflow rule protects revenue better than almost any downstream appeal strategy.
Quick Reference Table for Occipital Nerve Block Coding
Billing teams need a one-screen answer, not a lecture. Use the table below as your pre-submission checkpoint.
Occipital Block Coding At-a-Glance
| Procedure/Nerve Targeted | Primary CPT Code | Common Modifiers | Typical Frequency Limit |
|---|---|---|---|
| Greater occipital nerve block | 64405 | 50 for bilateral, LT, RT depending on payer preference | Medicare denies more than three injections per anatomic site in a six-month period |
| Lesser occipital nerve block | 64450 | LT, RT, 59 when appropriate for distinct procedural reporting | Payers often restrict coverage to 2-4 injections annually |
| Bilateral greater occipital nerve block | 64405 | 50 or payer-preferred LT/RT structure | Subject to the same site-based frequency control |
| Greater plus lesser occipital nerve blocks in one session | 64405 and 64450 | 59 when needed to show distinct nerves, plus laterality modifiers as appropriate | Medicare indicates more than two nerves in one session may trigger medical review |
Keep this table in your billing SOP. It captures the code, the modifier logic, and the payer constraint that most often stalls payment.
Core CPT Codes 64405 vs 64450
Miscode the nerve, and you hand the payer a denial. The code choice for an occipital block starts with one question only: which nerve did the physician inject?
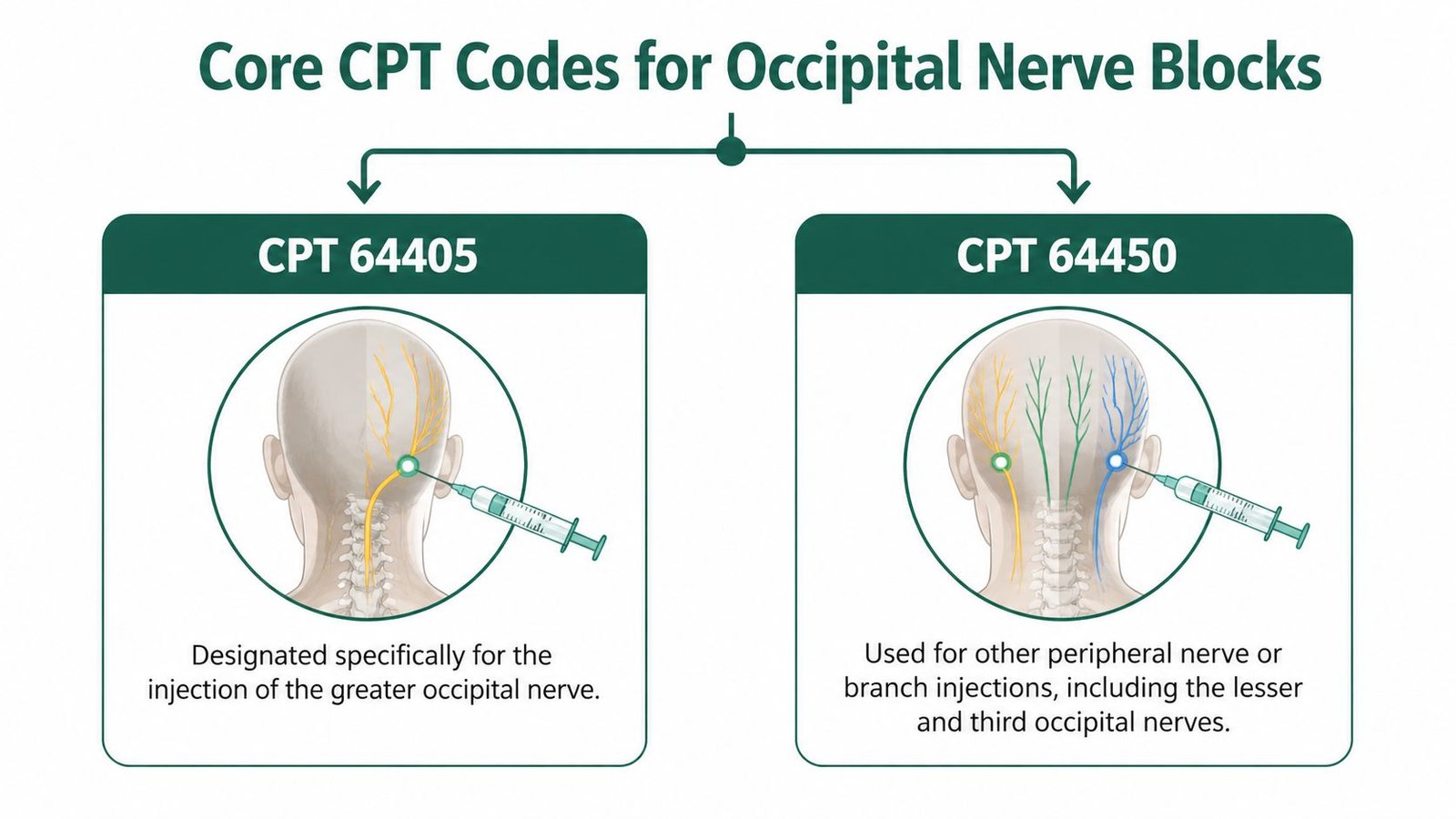
When 64405 is correct
Report 64405 for a greater occipital nerve block. Use it once per treated nerve region, not once per needle stick, not once per medication injected, and not once per physician attempt.
That distinction matters because charge capture errors usually start in the procedure note. A physician may document multiple injection points along the greater occipital distribution. That does not create multiple billable units of 64405. It is still one greater occipital nerve block unless the record supports a separate reportable nerve on the opposite side or a distinct additional nerve.
When 64450 is correct
Report 64450 for a lesser occipital nerve block. This is the coding gap that causes avoidable denials. Too many teams default every occipital injection to 64405 and miss the fact that the lesser occipital nerve is billed as an other peripheral nerve or branch injection.
Anthem addresses that directly in its peripheral nerve block policy. If the note says LON, lesser occipital, or clearly describes the anatomy consistent with the lesser occipital nerve, do not submit 64405.
Fix your intake and audit rules around that point alone. It will save rework.
When both nerves are treated in the same session
A same-day greater occipital nerve block and lesser occipital nerve block can support 64405 + 64450 when the physician documents two distinct nerves. Do not let the claim collapse into a single line just because both services happened on the same side of the head.
Your coding workflow should require four chart elements before you release the claim:
- The specific nerve named for each injection
- The side treated for each nerve
- The clinical indication for treating both nerves in the same encounter
- Clear separation of the services if your payer expects distinct procedural reporting, including proper use of modifier 59 for distinct nerve block reporting
If any of those elements is missing, hold the charge and query the note.
Bilateral logic is where practices lose money
Bilateral greater occipital blocks are commonly mishandled. If both greater occipital nerves are injected, the base code remains 64405, but the claim must reflect bilateral reporting based on payer preference. Some payers want one line with 64405-50. Others want two lines with LT and RT. The wrong structure can cut payment or trigger an edit even when the procedure itself was documented correctly.
The same discipline applies to the lesser occipital nerve. If the physician performs bilateral lesser occipital blocks, start with 64450 and then apply the payer's bilateral or laterality rule. Do not assume the bilateral logic for 64405 automatically transfers to every payer's handling of 64450. Build payer-specific edits into your PM system and train staff to verify them before submission.
One rule should be fixed in your SOP. 64405 is for greater occipital. 64450 is for lesser occipital. Bilateral reporting is a modifier decision, not a code substitution decision.
The financial consequence of getting this wrong
A vague note turns a payable claim into a coding debate. If the documentation says only "occipital block performed," your biller is forced to guess between 64405, 64450, or a combination of both. That guess costs time, appeals, and cash flow.
Require physicians to document the exact nerve treated every time. If the note does not identify greater, lesser, or both, it is not ready for billing.
Applying Essential Modifiers for Occipital Blocks
Correct occipital block coding depends as much on modifiers as on the base CPT code. A clean 64405 claim can still deny if the laterality or distinct procedural logic is wrong.

You should also keep a payer-specific modifier matrix alongside your charge capture rules. Teams that need a deeper refresher on distinct procedural reporting should review modifier 59 billing guidance.
Modifier 50 for bilateral greater occipital blocks
Use modifier 50 when the physician performs bilateral greater occipital nerve blocks. That instruction is explicit in occipital block coding guidance. If both sides of the head are treated at the greater occipital nerve, 64405 with -50 is the standard starting point.
Common pitfall: submitting two unilateral lines when the payer expects one bilateral line with modifier 50.
LT and RT when payer preference overrides 50
Some payers don’t want bilateral reporting through 50. They want LT and RT instead. The coding rule isn’t hard. The operational rule is. Your PM system needs payer-level edit logic so the same clinical event doesn’t get billed three different ways by three different staff members.
Use LT/RT when:
- The payer rejects 50
- The payer’s policy or past adjudication history shows a side-specific preference
- You’re billing unilateral procedures and need precise laterality
Common pitfall: using 50, LT, and RT together without a payer rule supporting that structure.
Modifier 59 for distinct nerves
Use modifier 59 when appropriate to show that two separately reportable services were performed on distinct nerves in the same session, such as a 64405 for GON and 64450 for LON. Many practices often underbill in these situations. They assume proximity equals bundling. It doesn’t.
If the physician treated distinct nerves and documented them separately, you should code them separately and use the distinct procedural modifier where payer edits require it.
Modifier 25 for same-day E and M
NCCI guidance allows E/M to bundle unless the visit involved a significant, separately identifiable service. If the physician performed a true evaluation that led to the decision for the block, append modifier 25 to the E/M code.
Use it only when the documentation stands on its own.
- Appropriate use: new neuralgia evaluation, decision-making, exam, and procedure on the same day
- Bad use: routine pre-procedure discussion dressed up as a billable office visit
QK and anesthesia-specific supervision modifiers
In anesthesiology groups, concurrency and medical direction rules matter. If the service setting and provider structure support it, anesthesia-specific modifiers such as QK may apply. These aren’t occipital-block-specific modifiers, but they absolutely affect anesthesiology reimbursement when the procedure is incorporated into broader anesthesia operations.
Build your edit logic in this order: base code, nerve specificity, laterality, distinct service status, then payer preference.
That sequence prevents most modifier-driven denials before the claim leaves the building.
ICD-10 Crosswalk for Medical Necessity
A technically correct CPT code won’t pay without diagnosis support. In occipital block billing, the diagnosis must match the procedure and the nerve story in the note.
The most important diagnosis in this category is G44.84, which is used for occipital neuralgia in billing guidance tied to greater occipital nerve blocks. If your physician is performing a GON block and documents classic occipital neuralgia findings, that diagnosis should be considered first.
For anesthesiology and pain teams, the practical issue isn’t just selecting a diagnosis code. It’s linking the diagnosis to the right procedure line and making the note clinically coherent. Review the broader pain management ICD-10 coding guide if your team needs a cleaner diagnosis selection workflow.
Diagnosis pairings that usually make sense
Use diagnosis-to-procedure logic, not habit:
- G44.84 with 64405: best fit when the provider documents greater occipital neuralgia findings
- G44.84 with 64450: may support lesser occipital treatment if the note clearly identifies that nerve and the clinical presentation
- G50.0 with trigeminal block codes, not 64405: don’t crosswalk cranial nerve diagnoses to the wrong peripheral block code
What billers should verify before release
Run these checks before claim submission:
Diagnosis supports the procedure
The ICD-10 must justify the exact nerve block performed.Diagnosis pointer is attached to the right line
If more than one procedure is billed, pointer errors can cause automated denials.The note matches the claim
If the claim says GON but the note says only “occipital injection,” the record is exposed.
Medical necessity is established by the diagnosis, but defended by the note.
If your providers are treating headache syndromes that don’t clearly meet neuralgia criteria, don’t assume the payer will accept 64405 just because an injection was performed. The record has to show why that nerve block was indicated.
Documentation Templates for Denial-Proof Notes
Most occipital block denials are documentation failures disguised as coding failures. The code is often right. The chart isn’t strong enough to support it.
For 64405, repeat therapeutic blocks depend on documented benefit from prior injections. Clinical policy guidance cited in payer-oriented material requires proof of improvement, typically through numeric pain scoring and clear response documentation. The strongest pattern is a pre-block score, a post-block score, and a statement that prior injections delivered at least 50% pain relief before repeats are authorized or paid (Horizon BCBSNJ policy discussion).
If you’re already dealing with avoidable denials in this category, tighten the note template before you tighten the appeals process. Teams that need to recover payment after the fact can use a structured denied claim appeal workflow, but the better move is preventing the denial upstream.
What every note must include
Build these fields into the provider template:
Specific nerve targeted
State greater occipital nerve, lesser occipital nerve, or both.Laterality
Document right, left, or bilateral.Medication injected
Record the anesthetic agent and or steroid used.Clinical indication
Tie the procedure to the diagnosis and symptoms.Pain scale before and after
Use a numeric rating scale. Don’t rely on “patient felt better.”Response to prior block if repeating
State prior relief and duration clearly.
A practical note framework
Use a simple, repeatable structure:
Indication: Occipital neuralgia or chronic headache pattern meeting the practice’s medical necessity standard.
Target nerve: Right GON, left GON, bilateral GON, LON, or combined GON and LON.
Technique: Injection performed to specified nerve with documented agent.
Pre-procedure pain score: Numeric score recorded.
Post-procedure pain score: Numeric score recorded after intervention.
Repeat rationale: Prior block produced clinically meaningful temporary relief.
What payers want to see on repeat blocks
Serial injections are where practices lose money. The repeat claim needs to show not just recurrence of pain, but benefit from the last injection. If the first block didn’t help, continuing to repeat the same service becomes much harder to defend.
Use a repeat-block checklist:
- Document prior improvement quantitatively
- State recurrence timing
- Explain why another block is reasonable
- Stop the series when the response pattern fails
A note that says “patient tolerated procedure well” helps clinically. A note that shows pre and post pain scores gets the claim paid.
This is one of the easiest documentation upgrades an anesthesiology or pain practice can make.
Navigating Payer Policies and Frequency Limits
Occipital block billing becomes expensive when the practice follows a clinical schedule but ignores payer frequency rules. Payers don’t care that the physician likes a monthly cadence if the coverage policy doesn’t support it.
Medicare guidance is blunt. More than three injections per anatomic site in a six-month period are denied for occipital nerve block injections, and commercial carriers often narrow coverage further to 2-4 injections annually according to billing guidance focused on peripheral nerve block coding (GoHealthcare billing guide for 64405 and related nerve blocks).
Medicare is stricter than many physicians expect
The biggest operational mistake is counting visits instead of counting injections by site and timeframe. Your scheduler, provider, and billing team should all work from the same frequency tracker. If the patient is approaching the Medicare cap, the chart should be flagged before the appointment happens.
Another issue is session complexity. Medicare guidance discussed in payer policy notes that more than two nerves blocked in one session may trigger medical review. That doesn’t mean the service is automatically nonpayable. It means your documentation burden rises immediately.
Commercial payer variation is where denials multiply
Commercial plans often add their own medical necessity requirements for serial blocks. Some require failed conservative treatment before repeats. Others focus heavily on whether prior injections produced measurable temporary relief. The practical problem is variance. The code may be the same, but the adjudication logic isn’t.
A payer-facing analysis of greater occipital nerve block rules also notes projected 2025 trends in LCD interpretation, including a single diagnostic block first, then three-month intervals only on recurrence, not prophylactic repeat scheduling (AMA CPT Assistant summary via Find-A-Code). Treat that as a coverage posture to watch, not a reason to default every patient into a serial block plan.
The policies your front end should check every time
Before the procedure, verify:
Frequency history
Count prior injections by site and payer rule.Diagnostic versus therapeutic purpose
Some policies scrutinize therapeutic repeats more aggressively.Conservative treatment history
If the payer expects failed conservative care first, have it in the chart.Authorization requirement
Don’t assume office-based nerve blocks are exempt.
For teams refining intake and financial clearance, a structured prior authorization workflow guide is worth standardizing into the front-end process.
The fastest way to lose margin on occipital blocks is to perform a technically correct procedure on a date the payer won’t cover.
That’s not a coding issue. It’s a policy discipline issue.
Coding for Related and Bundled Procedures
Bundling errors on occipital block claims destroy margin fast. The biggest misses are separate billing for work already included in the primary service, and weak differentiation between a true nerve block and another injection performed in the same region.
Ultrasound guidance 76942
Report 76942 only when the payer allows separate reimbursement, the physician used ultrasound for needle guidance, and the note supports it. As noted earlier, some billing guidance treats ultrasound as separately reportable with occipital nerve block coding, but payment still depends on payer edits and documentation quality.
Require these elements in the procedure note:
- ultrasound used for needle guidance
- permanent image retention, if the payer requires it
- relevant anatomy identified
- needle visualization documented
- final injection location documented
If the note says only “ultrasound used,” expect a denial. Billers should hold the claim until the record shows guidance work clearly enough to survive review.
Trigger point injections versus occipital nerve blocks
The anatomic region does not determine the code. The target structure does.
Use 64405 for the greater occipital nerve. Use 64450 for a lesser occipital nerve block when that is the documented target. Use 20552 or 20553 only when the physician injects myofascial trigger points in muscle.
This is a common source of revenue leakage. A note that says “occipital pain treated with injection” is not enough. Your template should force the physician to identify the nerve or confirm that the injection was muscular. If the physician treated both a nerve and trigger points, each service needs separate documentation, separate medical necessity, and clear anatomic distinction.
Local anesthetic is included
Do not bill local skin wheal or infiltration separately when it is performed to place the occipital block. That work is part of the primary procedure.
Teams that try to carve out prep anesthesia create avoidable overbilling risk and invite payer scrutiny across the entire pain service line.
Same-day surgery rules
If the block is performed on the day of surgery, confirm the purpose before billing. For hospital-based anesthesiology groups, the key question is whether the block was for postoperative pain management or whether it served the surgical or intraoperative anesthetic plan. That distinction affects whether separate reporting is appropriate.
Build this edit into charge review. Do not leave it to manual memory.
Escalation beyond repeat injections
Repeated occipital nerve blocks that stop producing meaningful relief should trigger a coding review, not automatic rebilling of the same injection code. In some cases, the physician may shift to 64640 or another destructive procedure, which is a different service with different documentation and coverage expectations.
That handoff often breaks down operationally. Clinical staff see “repeat occipital pain treatment.” The billing team needs to see a different procedure family, different risk profile, and different prior authorization requirements.
Related-procedure checklist for clean claims
Before claim release, confirm five points:
- the note identifies greater occipital versus lesser occipital nerve
- 64405 and 64450 are not used interchangeably
- any separately billed imaging guidance is fully documented
- trigger point codes are used only for documented myofascial injections
- bundled local anesthesia is not billed separately
Disciplined coding safeguards revenue. Occipital block claims usually fail on small technical mistakes, especially when LON blocks are miscoded as 64405 or bilateral work is reported inconsistently across related services.
Common Denial Scenarios and Prevention Strategies
Most occipital block denials are predictable. That’s good news. Predictable denials are preventable denials.
If your group handles these services routinely, build the workflows around specialty-specific edits instead of generic claim scrubbing. That’s especially important for anesthesiology billing operations, where concurrency, modifier logic, and postoperative pain rules all intersect.
Denial for wrong nerve code
Problem: The note says “occipital block,” billing assumes 64405, but the physician treated the lesser occipital nerve.
Prevention: Make nerve identification mandatory in the procedure template. No final signature without GON or LON selected.
Denial for incorrect bilateral reporting
Problem: The payer rejects 50 and wants LT/RT, or the claim uses inconsistent laterality structure.
Prevention: Maintain payer-specific modifier edits in the PM system. Don’t rely on biller memory.
Denial for exceeded frequency
Problem: The service crosses the payer’s allowed interval or count.
Prevention: Put a scheduling hold tied to prior injections by date and anatomic site. This should fire before the patient arrives, not after the claim denies.
Denial for lack of medical necessity
Problem: The diagnosis is vague, prior relief isn’t documented, or the note doesn’t support a repeat therapeutic block.
Prevention: Require pre and post pain scores and prior response details for all repeat injections.
Denial for multiple nerves in one session
Problem: The physician blocks more than two nerves and the chart doesn’t justify it.
Prevention: Add an internal audit trigger whenever more than two nerves are coded on the same date of service.
Claims don’t get paid because the procedure happened. Claims get paid because the chart, code, modifier, and payer rule all agree.
That’s the standard your rev cycle team should enforce.
Frequently Asked Questions About Occipital Block Coding
Can you bill 64405 for a lesser occipital nerve block
No. 64405 is for the greater occipital nerve. A lesser occipital nerve block is generally billed with 64450, and using 64405 for LON is one of the easiest ways to trigger denials or post-payment scrutiny.
Should bilateral occipital blocks always use modifier 50
Not always. For bilateral greater occipital nerve blocks, modifier 50 is the standard instruction. But some payers prefer LT and RT instead. Your billing rule should be payer-specific, not hardcoded to one national assumption.
Can you bill greater and lesser occipital nerve blocks on the same day
Yes, if the physician treated two distinct nerves and documented them clearly. In that case, 64405 and 64450 may both be appropriate, with modifier 59 when needed to show distinct procedural reporting. If the session includes more than two nerves, expect added payer scrutiny.
Is ultrasound guidance separately billable with 64405
It can be. Guidance materials identify 76942 as not bundled with 64405 when ultrasound guidance is used and documented. Payment still depends on payer policy and clean documentation.
Happy Billing helps anesthesiology, pain management, and other high-acuity groups tighten code selection, modifier logic, and denial prevention without forcing an EHR migration. If your team wants cleaner occipital block claims, stronger first-pass accuracy, and fewer avoidable denials, see how Happy Billing supports specialty-specific RCM workflows.