PR 119 Denial Code: What It Is and How to Fix It
A PR 119 denial code means the payer says the patient has reached a benefit maximum for that service, and the balance shifts to patient responsibility, not provider write-off. If you are looking at a remittance with 119 on it, the first question is not “How do we rebill this?” It is “Is this PR, and did the payer count the benefits correctly?”
That distinction matters fast. In a busy orthopedic, therapy, cardiology, anesthesia, or behavioral health operation, PR 119 can either be a legitimate patient balance or a recoverable denial caused by unit errors, duplicate service history, missing modifiers, or payer miscounts. The teams that handle it well do two things better than everyone else. They read the remittance line by line, and they tie the denial back to the exact CPT, modifier, date of service, and payer rule that triggered it.
What Is Denial Code PR 119
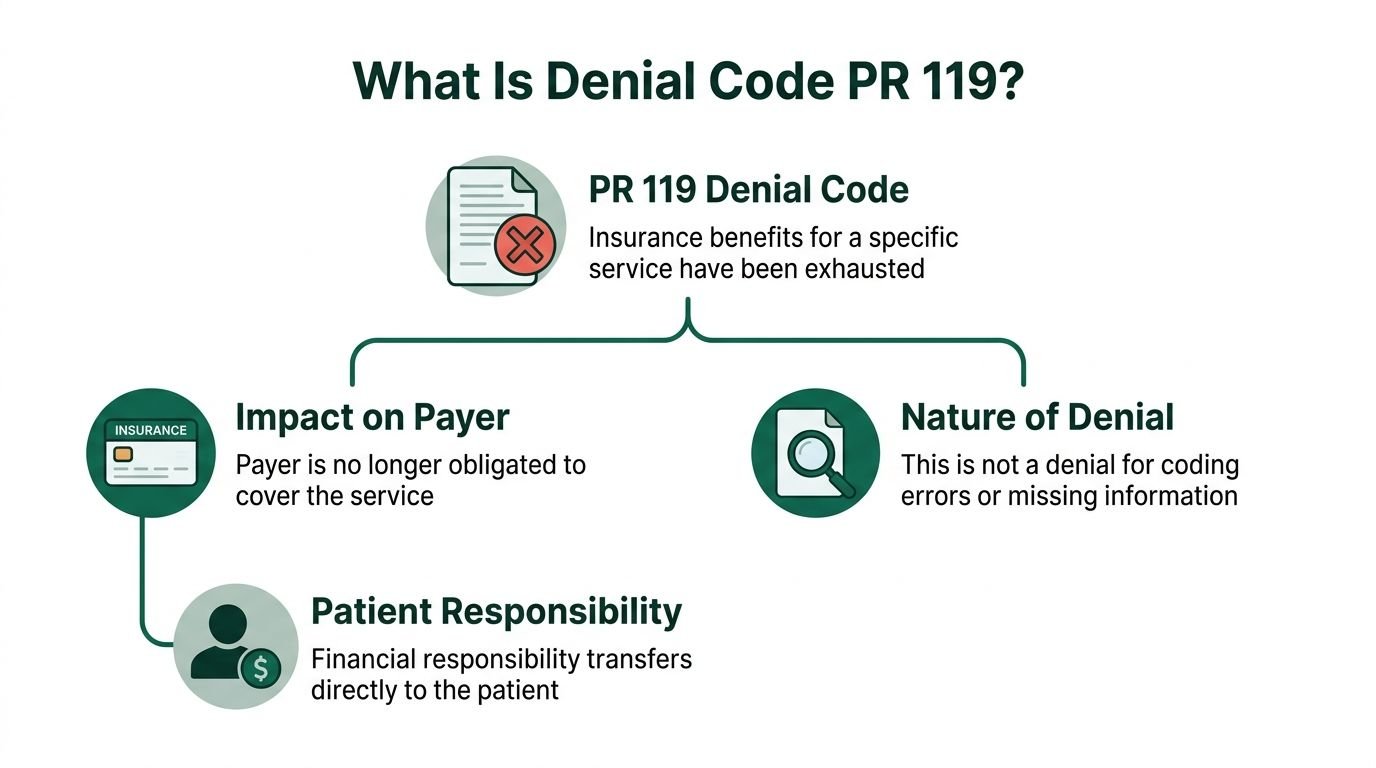
PR 119 tells you the payer has assigned the denied amount to the patient because the plan’s benefit maximum for that service, time period, or occurrence has been reached. That is the operational meaning your billing team should use.
The financial distinction is the first thing to train on. PR means patient responsibility. CO means contractual obligation. With PR 119, you may have a collectible patient balance if your documentation and financial policies support it. With CO 119, the practice is generally looking at a write-off under payer contract terms. A useful refresher on how these denial categories affect reimbursement sits in this breakdown of medical billing complexities explained.
A simple analogy helps staff remember it. Think of a mobile data plan. Once the included data is used, the carrier stops covering additional usage under the standard benefit. PR 119 works the same way. The plan says the covered bucket is empty.
According to EZMD Solutions’ explanation of PR 119, this denial commonly appears when patients exceed plan limits for services such as therapy, including plans with specific physical therapy visit limits or mental health benefits capped at a certain amount annually.
What PR 119 is not
This code is not automatically a coding error denial. It does not mean your CPT was invalid, your NPI was wrong, or your documentation was absent. It means the payer is framing the problem as a benefit maximum issue.
That said, billing mistakes can still trigger it indirectly. A wrong unit count on 97110, a duplicate line for 97140, or a date of service keyed into the wrong benefit period can make the payer think the patient exhausted benefits sooner than expected.
What to read with the code
PR 119 rarely stands alone in a useful way. The remittance context matters.
Look for remark codes such as:
- N362 when the payer says the number of days or units exceeds its maximum
- N30 when eligibility timing or coverage status affects the benefit count
- M86 when the payer is treating the service as already paid on a same or similar claim within the relevant time frame
Tip: Train front-desk and A/R staff to stop saying “denied for no coverage” when they see PR 119. That wording creates bad patient conversations and misses appeal opportunities.
Common Triggers for PR 119 Denials Across Payers
PR 119 sits in the denial bucket that looks simple on paper and messy in production. It is one of the top 10 most common medical billing denials, driven by exhausted visit limits, dollar caps, and procedural errors, according to Zee Medical Billing’s denial analysis. That same source notes payer caps are common across therapy services, and Medicare’s 2026 therapy thresholds are $2,480 each for PT/speech and OT.

The cleanest way to diagnose PR 119 is to split causes into two buckets. The first is true benefit exhaustion. The second is administrative distortion, where the payer or provider record makes it look like the limit was reached when it was not. If your team confuses the two, it wastes appeal time or, worse, bills patients incorrectly. For contrast with the contractual version, compare it to this guide on CO 119 denial code.
Legitimate benefit exhaustion
Some denials are exactly what the payer says they are.
A few common examples:
- Therapy services: CPT 97110, 97140, 97530, and related rehab codes often hit annual visit caps under commercial plans.
- Behavioral health: CPT 90837 can run into session or dollar maximums under some plans.
- Speech and occupational therapy: benefit limits may aggregate by discipline or by combined annual spend.
- Chiropractic and injection-based care: frequency limits can trigger the same denial logic when the payer allows only a certain number of occurrences.
Payer rules matter more than coding purity in this context. You can submit a technically perfect claim with the right diagnosis pointers, correct place of service, and complete rendering data, and still receive PR 119 because the plan maximum has already been met.
Administrative triggers that create false PR 119 denials
This is the category many groups underwork.
The code says “benefit maximum reached,” but the actual cause is often one of the following:
| Trigger | How it creates PR 119 | Example |
|---|---|---|
| Duplicate billing | Payer counts the same service twice | Two claims for 97110 on the same date |
| Wrong units | System thinks more benefit was used than provided | 93015 or therapy units entered incorrectly |
| Wrong dates of service | Claim falls into the wrong benefit period | December service entered in January |
| Missing prior auth beyond limits | Payer uses the cap denial path instead of a cleaner authorization denial | Additional therapy visits without extension approval |
| Coverage lapse | Payer reduces or invalidates available benefits | Mid-course insurance change |
| Multi-provider utilization | Visits across separate practices consume the same plan bucket | PT at one clinic, OT at another |
Specialty-specific patterns
The denial pattern changes by specialty.
Orthopedics and pain management often see PR 119 after post-op rehab or repeated procedural lines create frequency issues. Global periods can confuse internal staff, especially when follow-up care and separately billable therapy services overlap in the scheduler’s view but not in the payer’s logic.
Behavioral health runs into it when session counts are not checked before scheduling recurring 90834 or 90837 visits.
Cardiology usually sees this less as a classic “visit cap” and more as frequency edits, same or similar logic, or cumulative benefit issues on repeated diagnostic services.
Anesthesiology sees a different version of the problem. The payer may not be capping anesthesia in the same way it caps therapy, but incorrect time units, duplicate submission, or modifier misuse such as QK, QX, or AA can alter how the claim is processed and make the payer’s historical count unreliable.
Key takeaway: The phrase “benefit maximum reached” is a payer conclusion. It is not yet a root cause.
The first diagnostic move that works
When PR 119 hits, pull four items before doing anything else:
- The exact denied CPT code
- Any modifiers on that line, such as KX, GP, GO, QK, or 59
- The payer’s remittance remark code
- Your utilization history across all providers and dates in the same benefit period
That combination tells you whether you have a valid patient balance, a corrected-claim situation, or an appeal.
How to Read a PR 119 Denial on a Remittance Advice
Teams often lose time on PR 119 because they read the remittance at the claim level, not the service-line level. PR 119 is a line-level problem first. The line tells you which CPT was denied, how the payer assigned liability, and whether a remark code gives you a path forward.
If your staff still struggles to identify where denial liability sits on an ERA, this primer on what is a clean claim in medical billing is useful because PR 119 often starts with a line that was “clean” technically but failed a benefit rule.
Follow the service line, not the total claim
Start with the denied procedure code.
Examples that deserve immediate review include:
- 97110 Therapeutic exercise
- 97140 Manual therapy
- 97530 Therapeutic activities
- 90837 Psychotherapy
- 93015 Cardiovascular stress test
- 93306 Echocardiography
- anesthesia lines with time reporting and modifiers such as AA, QK, or QX
Find the line item, then confirm:
- billed charge
- allowed amount
- paid amount
- adjustment amount
- CARC showing 119
- group code showing PR
- accompanying RARC such as N362, N30, or M86
If the group code is not PR, stop there. You may be dealing with a different financial outcome.
What the PR label changes operationally
When the adjustment group is PR, your next move is not always appeal first. Sometimes it is patient balance transfer, but only after validating the payer’s count.
A useful internal audit sequence is:
- compare the denied CPT and date of service to your PM and EHR records
- confirm whether another provider under the same plan used the same benefit bucket
- check whether the line was submitted with the expected modifiers
- review whether a prior corrected claim or void created duplicate history
How remark codes narrow the problem
Remark codes perform important functions.
| Code on remittance | What it usually means for your team |
|---|---|
| N362 | The payer believes units or days exceeded a maximum |
| N30 | Coverage or eligibility timing may be part of the issue |
| M86 | The payer believes payment was already made for the same or similar service within the policy window |
If you see M86, do not let staff default to “benefits exhausted.” Often the better question is whether the payer matched your current claim to a prior claim incorrectly.
What experienced billers document immediately
Teams that move these denials well build a short internal note the same day:
- denied CPT and modifiers
- date of service
- payer portal benefit response
- prior authorization status if relevant
- internal utilization count
- whether patient responsibility is likely valid, disputed, or pending appeal
Tip: A PR 119 denial without a clear benefit-history note should never move straight to patient statement drop.
That one discipline prevents avoidable patient complaints and reverses many bad balance transfers.
A Step-by-Step Guide to Remediating PR 119 Denials
The best response to PR 119 is a decision tree, not a blanket workflow. Some lines should move to patient responsibility quickly. Others should be corrected and resubmitted. A smaller but important group should be appealed because the payer counted incorrectly or ignored medical necessity.
Many practices treat PR 119 as final. That is a mistake. According to MediBillMD’s review of denial code 119, payer errors account for 5-10% of these denials, and in Medicare DME claims there has been a 15% rise in PR 119 denials tied to stricter time-frame tracking. Their review also notes appeals may succeed, especially when multiple providers are involved. For workflow design, this resource on medical billing denial management is aligned with how high-functioning A/R teams triage these claims.
Step one, validate the denial before touching the balance
Do not post the denial and move on.
Verify:
- the patient’s active plan and benefit period
- the exact service category subject to the limit
- whether the payer counts visits, dollars, units, or occurrence frequency
- whether another rendering provider contributed to the accumulated total
For therapy, review the claim line with discipline modifiers when applicable. For anesthesia, validate time units and direction or supervision modifiers. For cardiology, confirm whether the denied line is subject to a frequency rule rather than a broad annual cap.
Step two, separate valid patient liability from a claim defect
If the payer counted correctly and the benefit is exhausted, move the amount to patient responsibility based on your contract terms and financial policy.
The patient statement should be plain and specific. It should identify the denied service and state that the payer applied the amount to patient responsibility because the plan maximum was reached.
If the line is wrong because your claim was wrong, do not bill the patient.
Common corrected-claim scenarios include:
- wrong unit count on a therapy line
- duplicate submission of the same date of service
- wrong date of service entered into the claim
- missing modifier that changes payer adjudication logic
- incorrect provider sequencing when multiple clinicians or locations are involved
Step three, correct and resubmit when the issue is internal
Code-level discipline matters here.
Examples:
- 97110-KX when the line exceeded the relevant Medicare therapy threshold and documentation supports medical necessity
- 97110-GP-KX or 97530-GO-KX when payer logic requires both therapy discipline and threshold-related modifier handling
- anesthesia claims requiring corrected reporting of time and modifiers such as AA, QK, or QX
- cardiology claims where repeated diagnostic testing was submitted with inaccurate units or overlapping dates
Your corrected claim should fix only what is wrong. Do not rebuild the whole encounter unless necessary. Every extra change creates noise in payer review.
Step four, appeal when the payer count or same-similar logic is wrong
Appeal when:
- another provider’s utilization was counted incorrectly
- a duplicate already voided in your system still sits in payer history
- the payer applied same or similar logic to a service that is clinically or procedurally distinct
- documentation supports medically necessary services past the stated limit under payer rules
This matters in DME, therapy, orthopedics, and behavioral health, especially when patients receive care across multiple organizations.
A practical appeal package
A strong PR 119 appeal usually includes:
- denial remittance showing PR 119
- payer portal or benefit history printout
- claim form or corrected line detail
- provider documentation supporting medical necessity
- treatment notes showing why continued services were required
- any proof that the alleged duplicate is not the same service
A concise appeal paragraph works better than a long letter. For example:
We request reconsideration of the PR 119 denial for CPT [code] on [date of service]. Our records indicate the service was medically necessary and was either not counted correctly toward the member’s benefit maximum or was denied based on duplicate or same-similar logic that does not apply to this encounter. Supporting documentation includes treatment notes, utilization history, and claim detail reflecting the correct modifiers and service information.
Step five, decide quickly and close the loop
Do not let PR 119 sit in aging while staff debate it.
Use three status buckets:
| Status | Action |
|---|---|
| Valid PR 119 | Transfer to patient responsibility and communicate clearly |
| Correctable claim error | File corrected claim |
| Disputed payer application | Appeal with supporting records |
The faster you put the line in one of those buckets, the less rework your A/R team creates for itself.
Proactive Prevention for High-Stakes Specialties
The biggest PR 119 gains do not come from better appeals. They come from not generating the denial in the first place. In operations terms, this is a front-end control issue tied to eligibility, utilization tracking, coding accuracy, and specialty-specific payer behavior.
Noridian’s Medicare guidance indicates that in therapy billing, exceeding the 2026 threshold of $2,480 triggers a PR 119 denial unless the KX modifier is applied to the claim line, and practices without automated benefit tracking can see denial rates from benefit exhaustion as high as 15-25%, compared with under 5% for proactive RCM workflows, as summarized in Noridian’s denial resolution guidance for M86/N119.

For cardiology groups, the denial pattern often overlaps with imaging and repeated diagnostics, which is why teams should also tighten controls around cardiology billing denials.
Orthopedics and physical medicine
Orthopedic groups see PR 119 most often around rehab utilization and post-procedure follow-up workflows that are not coordinated tightly enough between clinic and therapy.
Focus on these lines:
- 97110
- 97140
- 97530
- occupational and speech therapy lines when your group bills those services
What works:
- real-time visit counting by payer and benefit period
- front-desk alerts before scheduling the next visit near the limit
- checking whether the service is subject to annual cap, frequency rule, or medical necessity review
- applying KX correctly when Medicare threshold rules are met and documentation supports continued treatment
What does not work:
- relying on the patient to tell you how many visits are left
- tracking therapy counts in a spreadsheet no one reconciles
- adding KX after denial without reviewing the clinical note
- assuming the surgeon’s office and therapy department are looking at the same benefit history
Mental health and behavioral health
Behavioral health clinics run into PR 119 when recurring therapy visits keep moving with no hard stop in scheduling.
Common lines include:
- 90834
- 90837
The control point is not claim submission. It is the appointment workflow.
Use a scheduling rule that forces staff to verify session availability and any authorization requirement before the next recurring appointment is released. This is especially important when the patient also receives care from another behavioral health provider under the same plan.
Tip: If your behavioral health team only checks benefits at intake, you are inviting PR 119 later in the course of care.
Also watch for payer policy behavior that frames a missing authorization for visits beyond the standard allowance as a benefit issue. That can create a PR 119 pathway even when the core problem was not extending approval in time.
Cardiology and imaging-heavy groups
Cardiology practices do not always think of PR 119 as “their” denial, but they should. Repeated diagnostics can trigger frequency edits, same-similar logic, and annual benefit questions, especially when care is spread across locations.
Watch these CPTs closely:
- 93015
- 93306
The most effective preventive habit is to query eligibility with service specificity before repeat testing. A generic “active coverage” response is not enough. Staff need to know whether the payer applies utilization limits or prior review to the exact diagnostic category.
This gets missed in multi-site groups. The ordering physician may think the patient had no prior test in your office, while the payer history shows a similar service elsewhere in the same period. What prevention infrastructure needs
Anesthesiology
Anesthesiology has a different prevention profile.
The issue is usually not a straightforward annual visit cap. It is a claim that creates the wrong utilization footprint because of time, provider role, or concurrency reporting errors. Those errors can distort payer history and invite denials that look like benefit exhaustion or same-similar conflicts.
Operational controls should include:
- validating anesthesia time before claim release
- checking medical direction modifiers such as QK
- confirming rendering and supervising provider assignments
- reviewing repeated pain-related procedures when frequency rules may apply
Groups that want a specialty-specific operational benchmark should review the workflow demands on the anesthesiology billing page. The key point is simple. If the base claim is wrong, the next denial often appears in a category that looks unrelated.
What prevention infrastructure needs
You do not need more meetings. You need a usable utilization-control process.
A practical framework looks like this:
| Control point | Owner | What to verify |
|---|---|---|
| Scheduling | Front desk | Remaining visits, applicable auth, benefit period |
| Check-in | Eligibility team | Plan still active, payer rules unchanged |
| Charge entry | Coding team | CPT, units, modifiers, dates |
| Claim scrub | Billing team | Threshold modifiers, duplicate history, line-level edits |
| A/R follow-up | Denials team | PR vs CO, remark code, appeal potential |
When those five handoffs are disciplined, PR 119 stops being a recurring surprise.
Frequently Asked Questions About PR 119
Can I bill the patient when I get a PR 119 denial code
Usually yes, because PR indicates patient responsibility. But do not move the line to patient billing until you confirm the payer counted benefits correctly and the remittance shows PR, not CO. If the denial was caused by your duplicate billing, wrong units, or a missing modifier that should have been on the original line, correct the claim first.
Does PR 119 always mean the patient exhausted benefits
No. Some PR 119 denials are caused by payer error, duplicate claim history, same or similar misapplication, or benefit usage counted across multiple providers in a way that does not match the recorded information. That is why the denial should be validated against the payer portal, your internal claim history, and the exact CPT line before you post patient responsibility.
When should I use the KX modifier for a PR 119 issue
Use KX only when the payer rule calls for it and your documentation supports medical necessity. In Medicare therapy billing, the modifier matters once the relevant threshold is exceeded for the therapy category involved. It is not a general “fix denial” modifier, and adding it after the fact without chart support creates compliance risk.
What is the difference between PR 119 and remark code M86
They do different jobs. PR 119 is the claim adjustment reason framework that puts the denied amount into patient responsibility based on a benefit maximum issue. M86 is a remittance remark that adds context, often indicating the payer believes it already paid for the same or similar service within the relevant time period. When M86 appears, review prior claims before concluding the benefit is exhausted.
Happy Billing helps specialty practices tighten the exact workflows that drive denials like PR 119, from eligibility checks and modifier control to appeals and A/R recovery. If your team is losing time on therapy caps, same-similar edits, anesthesia modifier issues, or multi-provider utilization disputes, Happy Billing can help you build a faster and cleaner RCM process without disrupting your current systems.