A Practice Owner’s Guide to Mental Health Revenue Cycle Management

Effective mental health revenue cycle management (RCM) is the specialized financial process that ensures your practice gets paid correctly and on time for the services you provide. It involves managing patient intake, verifying benefits, securing authorizations, coding claims with specificity, and resolving denials for mental health services. Unlike standard medical billing, it requires deep expertise in time-based CPT codes like 90837, complex payer rules for prior authorizations, and navigating mental health parity laws.
This isn’t just medical billing with a different label. It demands deep expertise in the frustrating world of prior authorizations, the nuances of time-based CPT codes, and a complex web of mental health parity laws.
The Financial Lifeblood of Your Practice

Think of your RCM process not as a back-office chore, but as the central nervous system of your practice’s financial health. It’s the complete journey a patient's account takes, where every touchpoint is an opportunity for either predictable revenue or painful, costly leakage. A well-managed system ensures you get paid correctly and quickly for the vital care you provide.
Standard medical billing rarely deals with the session-by-session authorization headaches, the strict documentation needed for time-based codes, or the confusing patchwork of payer rules for telehealth that are just another Tuesday for a mental health provider.
Why Standard RCM Fails Mental Health
A generic, one-size-fits-all approach to RCM simply can't handle the unique demands of a behavioral health practice. The financial stability of your clinic hinges on mastering these specific challenges:
- Intensive Authorization Workflows: Payers often require prior authorization not just for an initial intake (CPT 90791) but for ongoing blocks of therapy sessions. Without a bulletproof system to track and renew these, claims for follow-up sessions are dead on arrival—guaranteed denials.
- Time-Based Coding Scrutiny: The difference between billing a 45-minute session (CPT 90834) and a 60-minute session (CPT 90837) isn't just 15 minutes. It’s a higher reimbursement that requires obsessive documentation of start and end times to survive an audit.
- Mental Health Parity Compliance: Navigating the Mental Health Parity and Addiction Equity Act (MHPAEA) means proving that a payer's limits on mental health care are no more restrictive than their rules for medical/surgical benefits. An expert RCM process is your best tool for identifying and fighting non-compliant denials.
The global Revenue Cycle Management market, which reached USD 85.2 billion in 2025, is projected to grow at a CAGR of 11.53% through 2034. This explosive growth underscores a universal truth: effective financial management is a strategic necessity. For mental health practices, it’s a flashing sign that specialized expertise is critical to survival.
At its core, specialized mental health revenue cycle management transforms the billing process from a source of frustration into a predictable engine for growth. It’s about building a financial framework that allows your providers to focus entirely on patient care, confident that the administrative side is secure.
Ultimately, a finely tuned RCM system solves the specific pain points that keep practice owners up at night. It leads to cleaner claims, fewer denials, and the stable cash flow you need to sustain and grow your practice. For a broader look at the fundamentals, check out our guide on healthcare revenue cycle management.
Navigating Critical Mental Health Billing and Coding
Success in mental health RCM isn't about generic advice. It comes down to mastering the specific, often tricky, coding and billing rules that govern behavioral health. If your billing process treats a therapy session like a standard office visit, you're leaving money on the table and inviting audits.
Protecting your revenue means getting granular at the code level. This is where theory ends and real-world practice begins.
The heart of the challenge lies in time-based Current Procedural Terminology (CPT) codes. Since the end of the PHE, payers have been scrutinizing claims, demanding precise documentation to back up session length. A simple note that says "45-minute session" just doesn't cut it anymore. That's a direct invitation for a denial or a painful takeback.
To get paid correctly for psychotherapy, your clinical notes absolutely must record the exact start and end times of the session. Think of it as the non-negotiable foundation for surviving any payer review.
Differentiating Time-Based Psychotherapy Codes
The real difference between billing CPT 90834 (a 45-minute session) and CPT 90837 (a 60-minute session) isn't just the 15 minutes. It's the documented proof that you met the required time thresholds.
According to CMS guidelines, which most commercial payers follow, you have to meet or exceed these minimums:
- CPT 90834: The session must last at least 38 minutes.
- CPT 90837: The session must last at least 53 minutes.
Billing for a 60-minute session when the note only supports 50 minutes is one of the most common—and easily preventable—reasons for denials and recoupments. The best practice is to make start and end time fields mandatory in your EHR templates. It makes compliance automatic for your clinicians.
For a deeper dive, you can learn more about the differences between CPT 90837 and 90834 in our detailed guide.
Justifying Add-On Codes and Telehealth Modifiers
Add-on codes can increase your reimbursement, but they demand rock-solid justification. A perfect example is the add-on code +90785 for interactive complexity. You can’t just add it; you have to prove why it was necessary.
To justify using CPT +90785, the provider’s note must paint a clear picture of what made the session complex. For instance, documenting that a child was nonverbal and the therapist had to use play instruments to communicate, or that a session with a patient with dementia required a caregiver's constant help to redirect them. That’s the kind of detail payers need to see.
Telehealth billing requires the same level of precision, especially now that the public health emergency is over. While telehealth is here to stay, payer rules are all over the map.
Key Telehealth Billing Rules:
- Place of Service (POS) Code: For any session where the patient is at home, you must use POS 10. Using the wrong code, like POS 02 (which implies the patient is at another medical facility), is a guaranteed denial.
- Modifier 95: This is the standard modifier for most synchronous telehealth services. However, some major payers like Aetna or UnitedHealthcare have their own specific policies, sometimes preferring modifier GT. You have to check each payer's rules.
Preventing Prior Authorization Denials
One of the biggest sources of lost revenue in mental health is a denial for "lack of prior authorization," particularly for higher-value services. Psychological and neuropsychological testing codes (CPT 96130-96133) are the most frequent offenders. Payers almost always require pre-approval for these.
A proactive authorization workflow isn't optional; it's essential. Your front-desk or admin team must have a system to verify benefits and secure an authorization before the service is even scheduled.
Getting an authorization number, the specific CPT codes approved, and the number of approved units or hours turns a common point of failure into a secure revenue stream. This front-end discipline is a cornerstone of a healthy mental health revenue cycle.
Building an Optimized RCM Workflow
Stop thinking of your revenue cycle as a series of reactive fixes. An optimized workflow is a proactive system designed to secure your revenue, moving beyond simply solving problems as they pop up. It’s a financial blueprint that maps the entire patient journey, from the first phone call to the final payment.
This blueprint isn’t just about submitting claims. A truly effective process starts long before the first session and ends with smart analysis that helps you continuously improve. When one stage fails, it creates expensive headaches downstream.
Stage 1: Patient Access and Authorization
Most denials are born at the front desk. This Patient Access stage is where you build the financial foundation for the entire patient relationship. It's far more than just collecting a name and address; it’s about clearing financial hurdles before they become problems.
Before a patient’s first appointment, your team has to run real-time eligibility and benefits verification. This confirms the patient has active coverage and—more importantly—tells you if their plan requires a prior authorization for the services you plan to provide. This step is non-negotiable for codes that payers love to gatekeep, like 90791 (psychiatric diagnostic evaluation).
Once you know an authorization is needed, the next step is to get it. This means getting an authorization number, confirming the approved CPT codes, knowing the exact number of approved sessions, and tracking the valid date range. A lapsed authorization is one of the most common—and completely avoidable—reasons for mid-treatment denials.
Stage 2: Charge Capture and Coding
This is where your clinical work gets translated into billable data. The goal of Charge Capture and Coding is simple: make sure your therapist’s documentation is strong enough to support every single CPT code you bill. Vague notes are a direct invitation for payers to downcode or deny a claim during an audit.
For instance, if you bill for crisis psychotherapy using CPT 90839, you need more than a note saying the patient was "in distress." The documentation has to paint a clear picture of a life-threatening or hazardous situation that required immediate, urgent intervention. This connection between the session, the code, and the justification is critical.
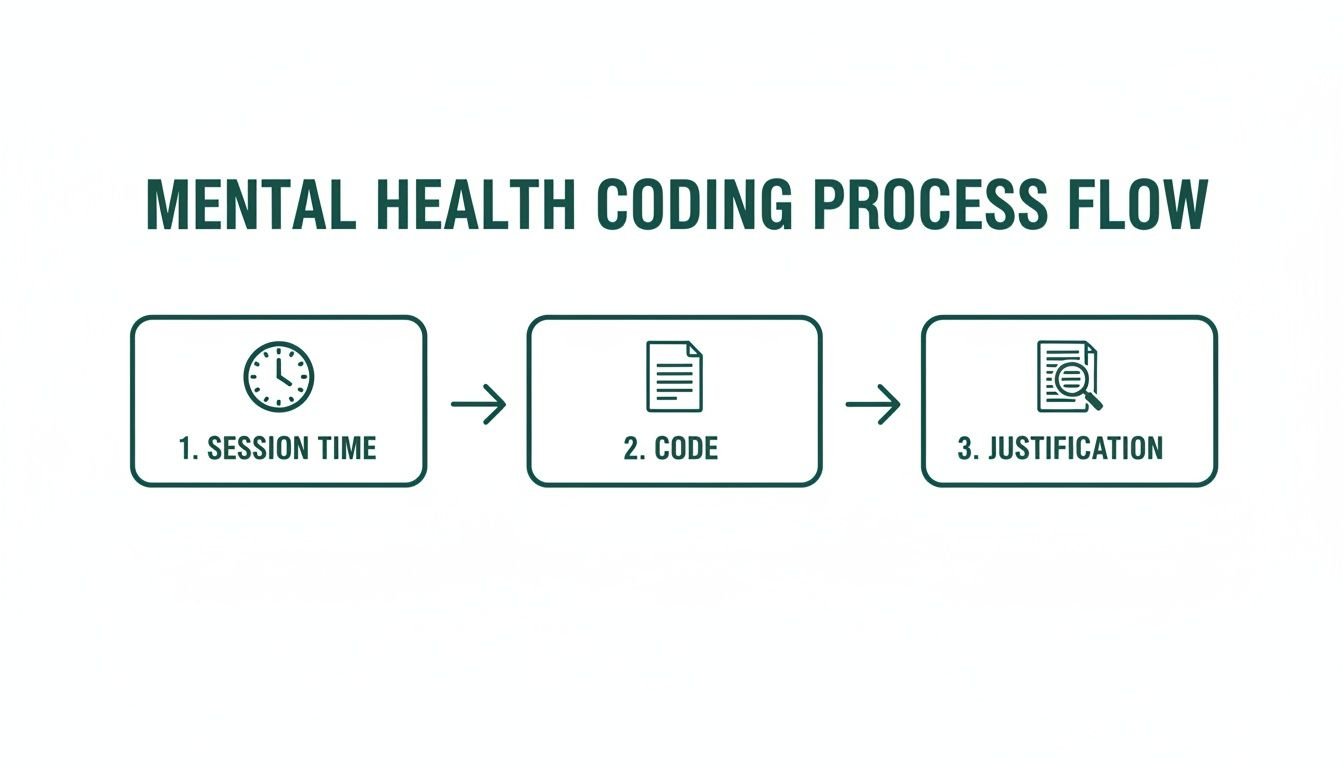
The flow from session time to code selection to detailed justification is the backbone of compliant billing. It makes every claim audit-proof.
Stage 3: Claim Submission and Scrubbing
Once a clean charge is captured, it’s time to submit the claim. But sending it straight to the payer without a final check is a huge mistake. A modern RCM workflow uses an automated claim scrubbing process as a final quality control gate.
Think of a claim scrubber as an expert proofreader for your billing. It's an AI-driven tool that checks each claim against a massive database of payer rules, flagging potential errors before the claim ever leaves your system.
This technology can spot thousands of issues, from a simple typo in a patient's birthdate to a complex coding error. For example, it will instantly flag a telehealth claim that’s missing the required Modifier 95 or has the wrong Place of Service (POS) code. Catching these mistakes before submission is the single most important factor in achieving a high first-pass clean claim rate.
Stage 4: A/R Management and Denial Resolution
Even with a perfect front-end process, some denials are going to happen. The final stages—Payment Posting, A/R Management, and Denial Management—are all about efficiently managing incoming cash and aggressively chasing down unpaid claims.
As payments get posted, your system should automatically flag any underpayments where the payer didn't meet the contracted rate. Your Accounts Receivable (A/R) team then needs to work these accounts systematically, starting with the highest-value and most recent claims first.
When a denial comes back, the goal isn't just to fix it and resubmit. The real goal is to understand why it was denied in the first place. A sophisticated mental health revenue cycle management process uses analytics to find trends. If you see UnitedHealthcare is repeatedly denying CPT 90847 (family psychotherapy), that’s not a string of bad luck—it’s a systemic issue that needs a targeted fix, like a team-wide documentation review or a direct call with your payer representative.
This turns frustrating denial data into powerful business intelligence. You can learn more by exploring our detailed guide to key revenue cycle workflow improvements that can strengthen your practice.
Measuring Success with Key Performance Indicators
You can't fix what you can't see. For a mental health practice, Key Performance Indicators (KPIs) are the financial vital signs that expose the health and efficiency of your revenue cycle. Tracking the right numbers moves you beyond guesswork and into strategic action, providing a data-driven look at your real performance.
Think of these metrics as diagnostic tools. A high denial rate or ballooning days in A/R aren't just numbers on a spreadsheet; they are symptoms of specific, fixable problems in your mental health revenue cycle management process—like broken authorization workflows or a disorganized approach to claim follow-up.
Getting a handle on these KPIs is the first step toward building a more resilient and profitable practice.
Core RCM Metrics Every Mental Health Practice Must Track
A handful of core KPIs tell the financial story of your practice. Practice managers should watch these relentlessly to spot negative trends before they snowball into major cash flow crises.
The goal isn't just to know the numbers but to understand what they're telling you. For instance, a low First-Pass Clean Claim Rate is a direct indictment of your front-end process, pointing to problems in how you handle patient registration, eligibility checks, or claim creation.
According to recent analysis, payer denials have become the single biggest threat to practice revenue. Nearly two-thirds of healthcare leaders now see them as the top barrier to growth, a problem felt acutely in mental health where practices now spend 50 to 75 hours per week on denial management alone. You can learn more from the full findings on RCM revenue risks.
Interpreting Your KPI Dashboard
Hitting industry benchmarks isn't an accident; it's the result of disciplined tracking and a clear understanding of what your data means. We've laid out the most important KPIs below, including how to calculate them and the performance goals you should be aiming for.
| Essential RCM KPIs and Industry Benchmarks |
| :— | :— | :— |
| KPI | How to Calculate | Industry Benchmark (Goal) |
| First-Pass Clean Claim Rate (FPCR) | (Claims Paid on First Submission / Total Claims Submitted) x 100 | 98% or Higher |
| Days in Accounts Receivable (A/R) | Total Accounts Receivable / Average Daily Charges | Under 35 Days |
| Denial Rate | (Total $ of Denied Claims / Total $ of Submitted Claims) x 100 | Under 5% |
| Net Collection Rate (NCR) | (Payments Received / Total Allowed Charges) x 100 | 95% or Higher |
Achieving these benchmarks is the difference between a practice that's thriving and one that's just surviving. Let’s break down what each of these numbers reveals.
First-Pass Clean Claim Rate (FPCR)
This is the ultimate report card for your front-end efficiency. A high FPCR means your patient registration, eligibility verification, and claim-scrubbing processes are working in harmony, catching errors before they turn into costly denials. The goal is to submit a perfect claim the first time, every time.
Target: Aim for 98% or higher.
Days in Accounts Receivable (A/R)
This KPI measures the average time it takes for you to get paid for your services. A high number is a red flag, often signaling bottlenecks in your prior authorization process, weak denial management, or a simple failure to follow up on aging claims.
Target: Keep this number under 35 days.
Denial Rate
Your denial rate directly measures revenue leakage. When this number creeps up, it's time to dig into the reasons. Analyzing denial codes—like "lack of medical necessity" for a 90837 CPT code or a "missing modifier" on a telehealth claim—gives you a clear roadmap for where to focus corrective action and staff training.
Target: Strive for a rate under 5%.
Net Collection Rate (NCR)
This metric reveals how much of the money you are rightfully owed you are actually collecting. After all contractual adjustments are made, this shows your effectiveness. A low NCR can point to problems with collecting patient responsibility or a failure to appeal underpayments from payers who don't pay what their contract requires.
Target: Target 95% or higher of the allowed amount.
By consistently monitoring these four metrics, you can transform your RCM from a reactive, fire-fighting function into a proactive, performance-driving engine. For a deeper dive, our team has put together a comprehensive resource on the most critical medical billing KPIs to track. These numbers are the foundation of a financially secure practice.
Blending Automation and Expertise for Modern RCM
Trying to manage your mental health revenue cycle with purely manual processes is like trying to do surgery with a butter knife—it’s clumsy, inefficient, and you're bound to do some damage. The most financially healthy practices aren’t just working harder; they're working smarter. They combine powerful automation with the irreplaceable judgment of human experts.
This hybrid model gives you the best of both worlds: the raw speed of technology and the critical thinking of seasoned RCM specialists.
Think of automation as the engine of your RCM. It’s built to handle the high-volume, repetitive tasks that burn out your staff and introduce costly human errors. Its greatest strength is on the front end, where it can stop revenue leaks before they even happen.
Where Automation Delivers Unbeatable Value
Modern RCM tech isn't here to replace your team. It’s here to free them up from soul-crushing administrative work so they can focus on tasks that actually require a brain—like fighting complex denials. Automation is best suited for the predictable, rules-based parts of your workflow.
Here’s where it shines:
- Real-Time Eligibility Checks: An automated system can instantly verify a patient’s coverage before they even walk in the door. It flags problems like an inactive policy, unmet deductibles, or specific session limits, allowing your team to have the financial conversation upfront, not after a denial comes back.
- Prior Authorization Initiation: Instead of having staff waste hours navigating clunky payer portals, automation can kick off authorization requests for common services. The system populates the required data, submits the form, and tracks its status, alerting your team the moment a decision is made.
- Automated Claim Scrubbing: This is a big one. Before a claim goes out, AI-powered scrubbers check it against thousands of payer-specific rules. They instantly catch common mistakes like a missing Modifier 95 on a telehealth claim or an outdated diagnosis code, which dramatically boosts your clean claim rate.
The potential here is huge. Across the healthcare industry, AI and automation could unlock up to $360 billion in annual savings. For behavioral health, this is a direct shot at cutting the administrative waste that comes from authorization and coding errors. It’s no wonder the outsourced RCM market is set to nearly double, with 70% of health systems planning to outsource more to cut costs.
The Irreplaceable Role of Human Expertise
For all its power, technology has a ceiling. An algorithm can tell you a claim was denied, but it can’t get a clinical reviewer from Cigna on the phone and argue a nuanced appeal. This is where your “human-in-the-loop” becomes your most valuable asset.
Automation can handle the what, but it takes a human expert to understand the why. When a payer denies a claim for extended psychotherapy (CPT 90837) for "lack of medical necessity," an algorithm can't read between the lines of a therapist’s notes to build a winning appeal. A person can.
An expert biller dissects complex denials, spots subtle patterns in payer behavior, and crafts compelling appeals that connect the dots between clinical documentation and billing codes. This human touch is the only way to overturn wrongful denials and recover revenue that technology alone would leave on the table.
This balanced approach—automation for speed, human expertise for precision—is the core of effective mental health revenue cycle management. It creates a system that’s both efficient and intelligent, ensuring you get paid faster while maximizing every dollar you’ve earned. To see how these tools work in practice, explore our guide on leveraging technology for your revenue cycle.
What Should a Mental Health Practice Owner Know About Choosing the Right RCM Partner?
When you’re vetting an RCM partner, confirm they use a hybrid model. Ask for proof. They should be able to show you detailed reports on their first-pass claim acceptance rate and their denial rates. Ask them to walk you through their process for appealing a complex, clinically-based denial. A great partner will be transparent about how automation handles the grunt work and where their expert team steps in to fight for your money.
How Does Automation Help with Prior Authorizations?
Automation is a game-changer for prior authorizations. It can automatically check if an auth is needed for specific services, like a 90791 (intake) or 96130 (psychological testing). If one is required, the system can auto-populate and submit the request to the payer’s portal. From there, it tracks the status and alerts your staff when it's approved or if more information is needed. In many practices, this cuts the manual labor involved by over 80%.
Can Technology Alone Solve All My Billing Problems?
Absolutely not. Technology is not a silver bullet. While automation is fantastic for preventing common errors and accelerating workflows, it can't handle every situation. Complex denials that demand clinical interpretation, negotiations with payers, or appeals built on nuanced documentation still require an experienced human biller. The most effective model is a "human-in-the-loop" approach, where tech does the routine work and experts handle the exceptions.
Ready to stop chasing claims and focus on patient care? At Happy Billing, we combine intelligent automation with expert human oversight to deliver a 98%+ clean claim rate and keep your days in A/R under 35. Learn how we can optimize your revenue cycle.
How can we reduce denials for lack of prior authorization?
The most effective way to reduce these denials is to implement a robust front-end workflow. Before a patient's first appointment, your administrative team must perform real-time eligibility and benefits verification to confirm if prior authorization is required for the planned services, especially for high-scrutiny codes like 90791 (psychiatric diagnostic evaluation) or psychological testing codes (96130-96133). For any service needing it, you must obtain an authorization number, confirm the specific CPT codes and number of sessions approved, and track the authorization's expiration date. Using a tracking system to alert your team of expiring authorizations at least two weeks in advance is a critical best practice to prevent mid-treatment denials.
What is the biggest mistake practices make with time-based CPT codes?
The single biggest and most common mistake is inadequate documentation of time. To bill for psychotherapy codes like CPT 90834 (45 minutes) or CPT 90837 (60 minutes), your clinical notes must contain the exact start and end times of the session. According to CMS and AAPC guidelines, simply stating "45-minute session" is insufficient and a major audit risk. To be compliant and justify the code billed, the documentation must prove you met the time threshold (e.g., at least 53 minutes for 90837). The best practice is to make start/end time fields mandatory in your EHR templates to enforce compliance.
When should we use Modifier 25 with psychotherapy?
Modifier 25 should only be appended to an Evaluation and Management (E/M) code (e.g., 99213, 99214) when a psychiatrist performs a significant, separately identifiable E/M service on the same day as a psychotherapy service (e.g., 90833, 90836). The classic, compliant use case is for medication management (the E/M service) performed in addition to a distinct psychotherapy session. Your documentation must clearly separate the two services, with the E/M portion having its own distinct history and medical decision-making documented apart from the psychotherapy note. Payers scrutinize this modifier heavily, so it should never be used routinely without compelling, separate documentation for both services. For more insights on rules like this, see our work with leading mental health practices.