Fixing Medical Billing Denials: A Practice Owner’s Guide
Stopping medical billing denials takes a system, not a patch. In Experian Health's 2025 State of Claims survey, 41% of respondents said at least one in ten claims is denied, which is why practices that combine front-end prevention, fast denial triage, and disciplined appeals protect revenue far better than practices that only react after remits arrive.
Last month, a specialty group asked why cash was tightening even though visit volume looked stable. The answer wasn't production. It was a stack of denials tied to intake errors, authorization mismatches, and appeals that sat too long before anyone owned them.
For an independent practice owner, medical billing denials aren't a back-office annoyance. They slow payment, push claims deeper into A/R, consume physician attention, and force staff to spend time reworking revenue you already earned. In some payer segments, denial rates are materially high. A compiled 2026 review reported that about 19% of in-network claims submitted through HealthCare.gov insurers were denied in 2023, with initial denial rates of about 15.7% for Medicare Advantage and 13.9% for commercial payers. The same review also noted that roughly 38% to 41% of organizations reported denial rates of 10% or higher (compiled U.S. denial statistics review).
If you're deciding whether to keep billing in-house, replace a vendor, or tighten your existing revenue cycle, the standard should be simple. Your billing operation should prevent avoidable denials before claim submission, route unavoidable denials immediately, and recover the claims worth fighting. Anything less leaks cash.
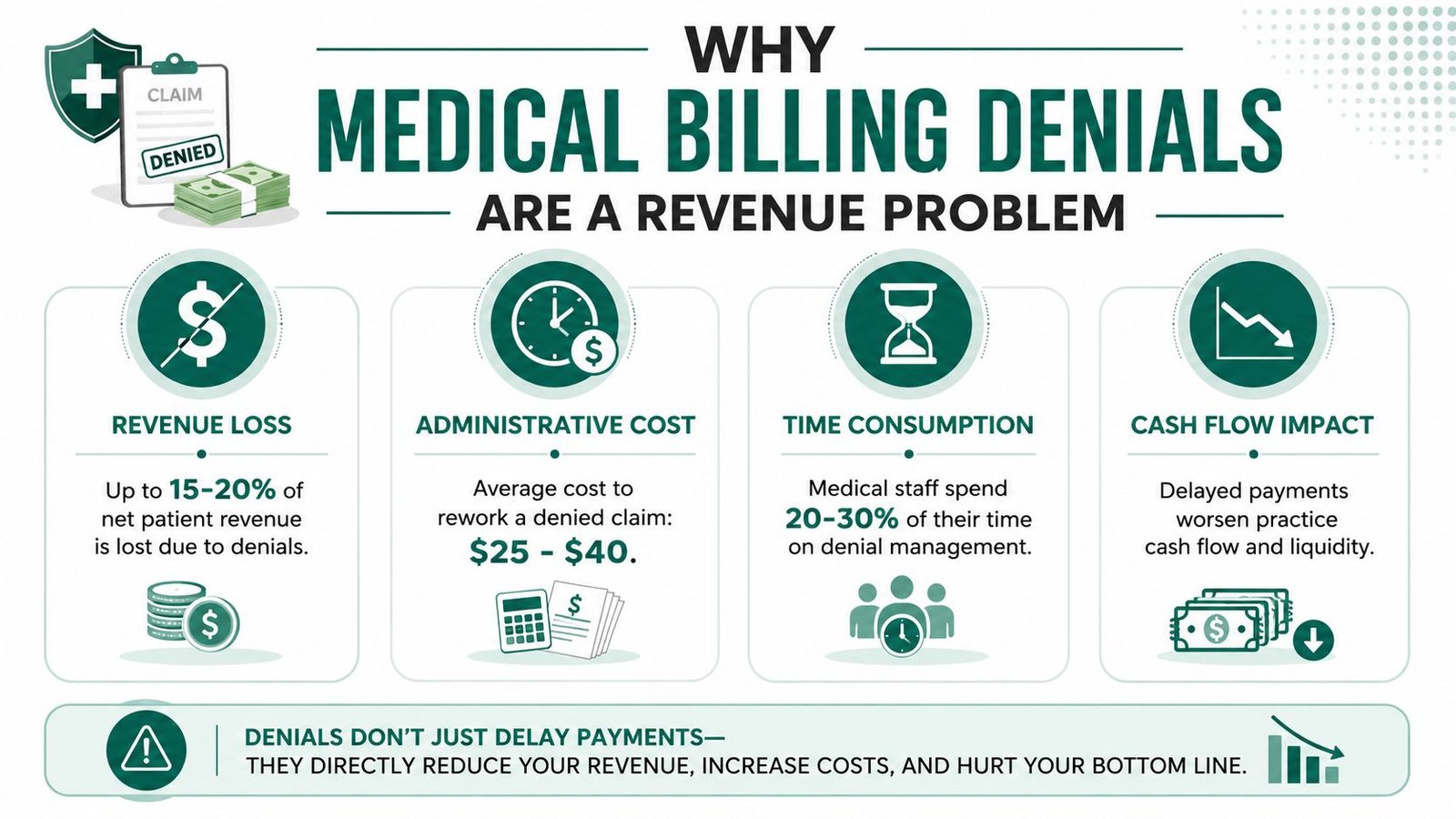
Why Medical Billing Denials Are a Revenue Problem
Medical billing denials hurt practices because they delay or block payment on work you've already performed. They also create a second labor cost. Someone has to research the remit, correct the claim, gather records, appeal it, follow up, and monitor whether the payer reprocesses it.
Experian Health's 2025 State of Claims survey shows how widespread the problem has become. 41% of respondents said at least one in ten claims is denied, and the leading denial drivers were missing or inaccurate data, authorization problems, and incomplete patient information (Experian Health's 2025 denial findings). For owners, that's the key point. A large share of denials begins before the claim ever reaches coding review.
A practice with recurring denials usually sees the same operational pattern:
- Cash arrives later: Denied claims don't just sit unpaid. They often move into secondary work queues and miss the normal payment cycle.
- A/R gets older: Each extra payer touchpoint extends the time from date of service to final payment.
- Leadership loses visibility: Gross charges may look fine while net collections soften.
- Staff effort shifts to rework: Front desk, authorization, coding, and billing teams all spend time correcting preventable mistakes.
Practical rule: If a denial trend is coming from registration, eligibility, or authorization, you don't have an appeals problem first. You have a workflow problem first.
Practice owners sometimes treat a denial rate in the low teens as normal because everyone around them seems to tolerate it. That's expensive thinking. If one out of every ten claims requires rework, your team is spending time financing payer friction instead of collecting cleanly the first time.
This is why owners need to understand the full revenue cycle management process, not just posting and collections. Denials are where weak intake controls, weak documentation controls, and weak follow-up controls all show up at once.
Revenue risk shows up before the bank balance does
The first sign usually isn't a dramatic collapse in collections. It's smaller and more dangerous. An increase in unresolved remits. More payer callbacks. More "needs records" tasks. More claims waiting on authorization proof. More physician interruptions to answer preventable documentation questions.
Those are not billing department inconveniences. They're early indicators that revenue is slipping out of process.
Owners should look at denials like a margin leak
Every denied claim creates a decision. Correct it, appeal it, or write it off. If your team can't make that decision quickly and consistently, the practice pays twice. Once in delayed reimbursement, and again in administrative drag.
Diagnosing the Root Cause of Your Denials
Most practices don't have one denial problem. They have three or four recurring failure points that keep producing the same denials under different payer names. The fastest way to fix medical billing denials is to separate upstream failures from downstream failures.

Recent analysis shows that eligibility denials often come from coverage changes not caught at registration and that authorization-related denials arise when approvals aren't verified before the visit or when the billed service doesn't match what was authorized (analysis of common denial causes and upstream prevention). In practice, that means scheduling and intake often control more collectible revenue than owners realize.
Start with the intake side
The front end creates a surprising share of denial risk. Not because staff are careless, but because payer rules keep shifting and high-volume intake is easy to underestimate.
Watch these pressure points closely:
- Eligibility verification at each encounter: Coverage changes, plan terminations, and network changes need to be caught before the patient is roomed.
- Authorization reconciliation: Approval on file isn't enough. The approved service needs to match what will be performed.
- Demographic accuracy: Small data errors can send a clean clinical encounter into avoidable payer friction.
- Referral requirements: Some plans still require PCP referral logic that front desks miss when they rely on outdated payer assumptions.
A lot of authorization packets, referral documents, and payer notices still arrive as PDFs. Practices that handle large specialty volumes often improve turnaround by using tools for extracting data from PDF files so staff can pull authorization numbers, dates, service descriptions, and payer references into a usable work queue instead of retyping everything by hand.
Then separate coding issues from coverage issues
Owners often hear "coding denial" and assume the coding team is the source. That can be true, but not always. Sometimes the code set is correct and the denial is really a coverage rule issue, a plan edit, or a mismatch between the approved service and the billed service.
Use a simple diagnostic split:
| Denial category | Usually starts where | What the owner should ask |
|---|---|---|
| Eligibility | Scheduling or registration | Was coverage rechecked close to date of service? |
| Authorization | Scheduling, precert, clinical coordination | Did approved service, date, and provider match the final claim? |
| Documentation | Provider documentation or chart completion | Did the chart support the billed service at submission time? |
| Coding and modifier use | Coding or claim editing | Was the code set technically correct and payer-appropriate? |
| Timely follow-up | Billing follow-up | Did the denial sit unworked too long? |
The best denial meetings aren't debates over blame. They're route-mapping exercises that show exactly where a bad claim entered the system.
If you want a sharper owner-level checklist, review the most frequent categories in this breakdown of the top 10 denials in medical billing. It helps frame whether your problem is concentrated at intake, coding, payer follow-up, or all three.
What usually doesn't work
Blanket retraining rarely works if you haven't identified the exact break point. Neither does telling the billing team to "appeal more aggressively" when the claim lacked verified eligibility before the visit. A denial rooted in bad intake data isn't fixed by a better appeal letter. It's fixed by changing the front-end workflow that created it.
A Practical Denial Triage and Management Workflow
Once a denial hits the 835, speed matters. Not frantic speed. Directed speed. The practices that recover more revenue don't work denials in whatever order staff happen to see them. They run a triage model.
AHIMA recommends a structured denial management process that includes quantifying and categorizing denials, conducting performance audits of remittance advice and write-offs, and using trend analysis to find root causes. That approach separates preventable front-end errors from post-adjudication issues and helps teams route denials effectively (AHIMA's structured denial management approach).
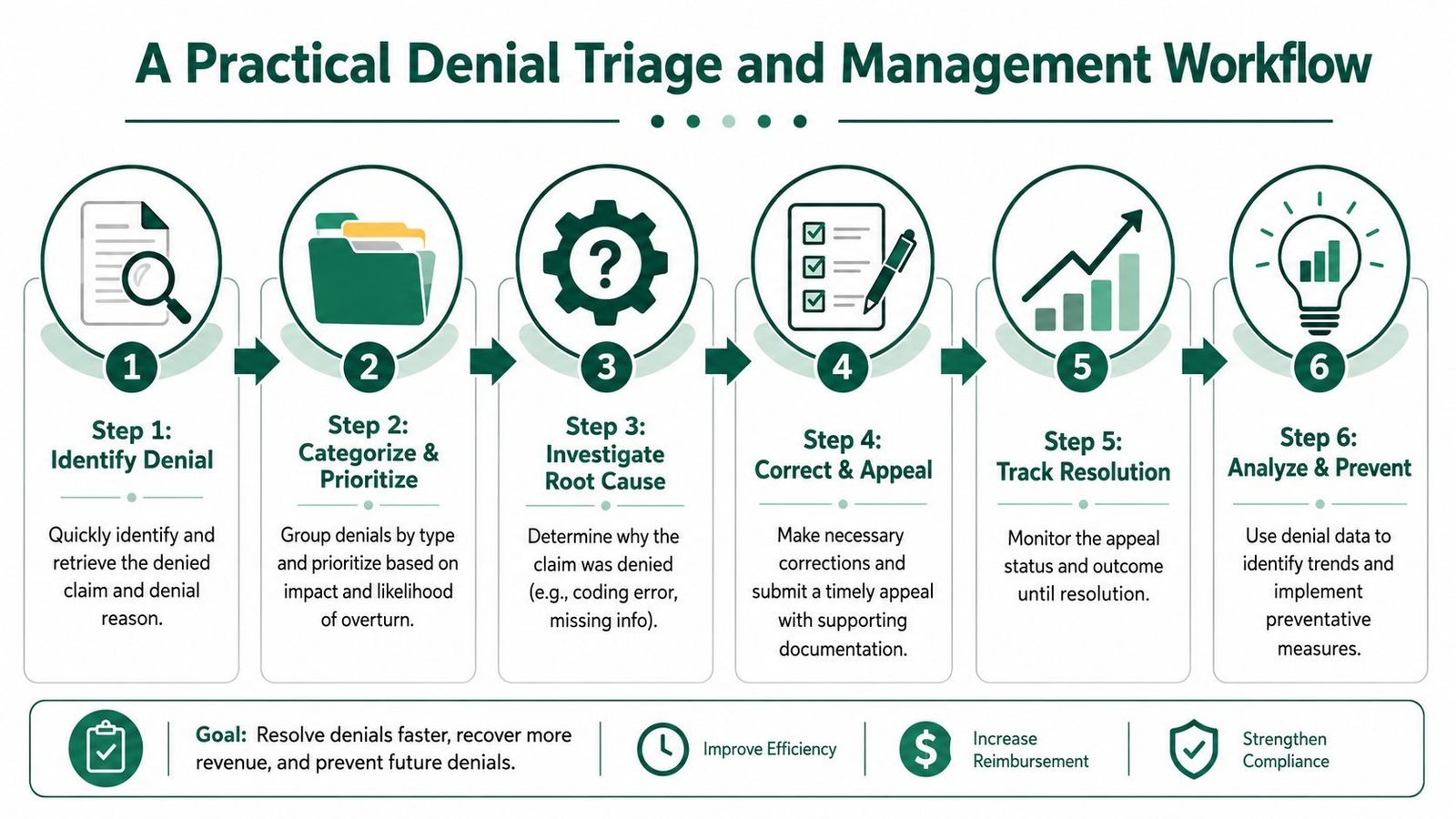
The workflow that works in real practices
Capture every denial immediately
Pull denials from the remit and load them into a queue that shows payer, denial reason, rendering provider, date of service, and claim value. If denials are discovered days later through ad hoc follow-up, you've already lost time.Assign a denial owner
One person should own the next action, even if multiple people touch the claim. Without ownership, denials float between front desk, coder, biller, and provider until the filing window gets tight.Classify by recoverability
Separate claims that need a simple correction from claims that need records, medical necessity support, authorization proof, or payer escalation.Prioritize by business impact
Higher-value claims, repeat denial patterns, and claims near appeal deadlines should rise first. Working only by oldest date or by smallest fix isn't enough.Correct and appeal with a payer-specific packet
A corrected claim isn't the same as an appeal. Some denials need claim correction. Others need a formal appeal with supporting records, authorization documents, operative notes, or modifier rationale.Feed the root cause back upstream
Every resolved denial should teach the system something. If the same payer keeps denying because the authorized service description doesn't match the billed code, that feedback belongs with precert and scheduling, not just A/R follow-up.
Build separate lanes for different denial types
A blended work queue slows everyone down. Create at least these operational lanes:
- Fast-correct lane: Demographic fixes, payer ID updates, missing member data, or claim form corrections.
- Documentation lane: Missing notes, unsigned records, or chart support issues.
- Authorization lane: Missing approvals, mismatched service approvals, wrong servicing provider, or wrong date span.
- Clinical appeal lane: Medical necessity and coverage disputes that need a more formal argument.
Claims age out when everyone can touch them and no one owns them.
What the denial owner should review every day
A denial owner doesn't need to do all the work personally. The role is control, not clerical volume. The daily review should answer:
- Which claims are closest to timely filing or appeal deadlines
- Which denials are repeating by payer or location
- Which claims need provider documentation today
- Which claims should be corrected instead of formally appealed
- Which denials should be escalated because the payer response conflicts with prior approval or prior processing
A simple operational dashboard often beats a complicated one. If the team can see open denials, next action, deadline, and assigned owner, that's enough to reduce avoidable stagnation.
Audits should include write-offs, not just appeals
Revenue often goes unaccounted for by many owners. The billing team may have an appeal process, but write-offs can still conceal recurring leakage. AHIMA specifically points to audits that include remittance advice, write-off adjustments, zero-payment claims, registration quality, and insurance verification quality. That's the difference between managing denials and merely reacting to them.
If your current workflow still depends on manual memory, payer-by-payer tribal knowledge, and inbox reminders, it's time to redesign it. A cleaner revenue cycle workflow improvement plan usually starts with queue design, ownership rules, and deadline discipline before any software change.
Winning Appeals in High-Stakes Specialties
High-stakes specialties don't lose money on generic denials alone. They lose money when complex claims are submitted correctly from a clinical standpoint but fail against payer logic, modifier logic, credentialing status, or diagnosis-to-procedure correlation.
HealthySteps' guidance highlights common technical denial drivers such as provider credentialing issues, non-covered services, and medical necessity failures. It also makes a critical point for specialty practices: if ICD-10 diagnosis codes don't correlate with the procedure code, insurers may reject the claim without review (technical denial drivers in medical claims). That's why specialty appeals fail when they argue generally instead of proving the exact billing relationship the payer says is missing.
The specialty appeal mindset
In high-value specialties, appeals need to do three things well:
- State the denial issue precisely
- Show the documentation and coding logic that supports payment
- Answer the payer's edit, not the practice's frustration
A weak appeal says the claim should be paid because the service was necessary. A strong appeal says the service was authorized, documented, coded to the performed service, billed with the correct modifier logic, and submitted with records that support the diagnosis-procedure relationship.
Specialty-Specific Denial & Appeal Tactics
| Specialty | Common Denial Reason | Example (CPT/Modifier) | Appeal Strategy |
|---|---|---|---|
| Anesthesiology | Modifier or concurrency dispute | 00840, QK, QX, AA | Submit the anesthesia record, time documentation, provider role documentation, and staffing pattern for the case. If the denial challenges concurrency logic, the appeal should explain who medically directed the case and how the billed modifier reflects the documented provider arrangement. For anesthesiology billing, this is often the difference between collectible payment and avoidable write-down. |
| Cardiology | Bundling or medical necessity denial | 93458, 93000, 99214 | Use the cath report, imaging interpretation, order, and diagnosis support to show why the interventional or diagnostic service met payer policy. If an E/M was separately identifiable, the appeal should explain the work beyond the procedure and document modifier use when appropriate. Practices dealing with recurring cath and imaging edits should also review these patterns in cardiology billing denials. |
| Mental health | Authorization mismatch or visit limit issue | 90837, 90834, 90853 | Include authorization number, approved service type, approved date span, and treatment documentation that matches the billed service. For mental health billing, denials often turn on whether the visit length, rendering provider, and authorized service category align exactly. |
| Orthopedics | Global period or modifier dispute | 27447, 20610, 99213, 25, 59 | Submit operative notes, post-op timeline, and documentation proving whether the service fell inside or outside the global package. If a separate E/M or injection was appropriate, the appeal should identify the distinct problem addressed and support the modifier with chart detail. In orthopedic billing, weak modifier support often turns collectible work into delayed cash. |
Four examples owners should recognize
Anesthesiology
An anesthesia group may perform the case correctly and still get denied because the payer questions modifier selection or concurrency reporting. In that scenario, the appeal should not ramble about medical necessity first. It should start with the anesthesia record, provider assignment, time record, and the exact basis for modifier use. If the payer denied QK or QX logic, answer that issue directly.
Cardiology
A cardiology group may see a denial on CPT 93458 tied to bundling or diagnosis support. The appeal should align the cath indication, findings, order, and final billed code set. When we review these accounts, the common mistake isn't lack of documentation. It's that the documentation isn't organized around the payer's stated reason for denial.
An appeal wins more often when it reads like a response to an edit, not a complaint letter.
Mental health
Behavioral health clinics often lose time chasing denials that are really authorization control failures. If 90837 was billed but the authorization supports a different service pattern or date span, no amount of generic resubmission will fix it. The appeal packet has to prove the visit matched the approved service, provider, and time expectation.
Orthopedics
Orthopedic groups frequently run into global package disputes. The payer says the service is included. The practice says it was separate. The appeal succeeds only if the chart clearly shows a distinct problem, separate decision-making, or a service outside the global package. Modifier 25 and modifier 59 aren't persuasive by themselves. The note has to earn them.
What doesn't work in specialty appeals
- Sending records without an argument
- Using the same appeal template for every payer
- Appealing low-recovery claims with high labor burden
- Ignoring credentialing and enrollment status when the denial points there
- Assuming the payer will infer diagnosis-to-procedure support from a large chart
Owners should expect specialty appeals to be selective, fast, and evidence-led. That is where recovery happens.
Tracking KPIs to Measure Denial Management Success
A denial management system isn't real until you can measure whether it's improving. Most practices track charges and collections. Fewer track whether denials are becoming more preventable, more recoverable, or more expensive to work.
AnnexMed points to a major gap in denial strategy: many teams don't segment soft denials such as eligibility issues from hard denials such as medical necessity disputes, even though appeal decisions should consider probability of recovery and staff time invested, not just dollars at risk (soft versus hard denial strategy).
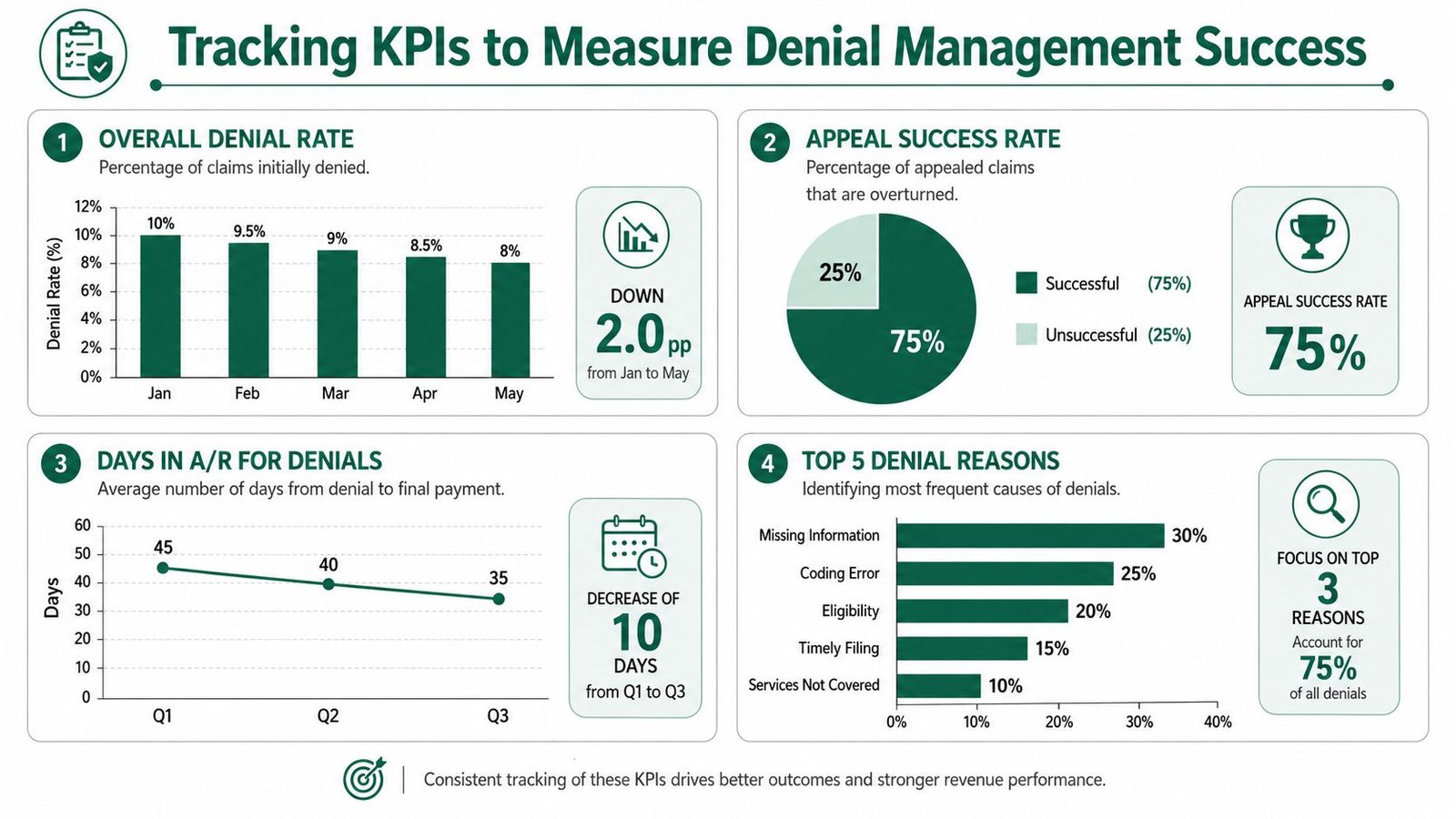
The KPIs that matter to an owner
Start with a monthly report your team can produce and defend.
| KPI | Why it matters | What to look for |
|---|---|---|
| Overall denial rate | Shows how much revenue is entering rework | Whether the trend is rising, stable, or improving by payer |
| First-pass resolution rate | Reflects claim quality before submission | Whether clean claim controls are working upstream |
| Appeal success rate | Shows whether appeals are targeted and supported | Whether staff are working winnable denials or just working everything |
| Average days to resolution | Measures cash delay on denied claims | Whether denials are aging because of poor ownership or payer friction |
| Top denial reasons | Reveals process failure patterns | Whether root causes sit in intake, coding, auth, or payer follow-up |
Soft denials and hard denials should not share the same strategy
Soft denials are often operationally fixable. Think eligibility verification gaps, missing data, or claim corrections. Hard denials tend to involve coverage policy, medical necessity, non-covered services, or more difficult payer positions.
That distinction matters because the staffing model is different:
- Soft denials: Work for speed, correction, and resubmission.
- Hard denials: Work for selectivity, documentation strength, and escalation discipline.
Owner question to ask every month: Are we spending our best staff time on the denials most likely to convert into cash?
If the answer is unclear, your reporting is too vague.
A practical monthly denial report
Ask your team or vendor for one page that includes:
- Top denial categories by payer
- Open denials by age bucket
- Appeals filed and appeals resolved
- Write-offs tied to denied claims
- Repeat denials tied to the same root cause
- Claims waiting on provider documentation or authorization proof
This doesn't need to be fancy. It needs to be usable. A strong denial report tells you where revenue is stalling and whether your team is fixing causes or just processing symptoms.
For a broader scorecard, this guide to medical billing KPIs to track is useful for owners who want tighter accountability from an internal team or outsourced partner.
Take Control of Your Practice Revenue
A surgeon once told me, "We are busy every day, so why does cash still feel tight?" The answer showed up in the denial trail. Staff were correcting claims late, appealing low-value cases, and missing the few denials that should have been escalated fast. Revenue was leaking at every handoff.
That is why denial management has to run as a system, not a rescue project.
For high-stakes specialties, one preventable denial rarely stays isolated. It delays payment, adds staff labor, pushes claims into older A/R, and distracts providers and managers from work that should produce revenue. The financial hit is not only the denied claim. It is the rework cost, the appeal burden, and the claims behind it that age while the team is tied up.
Practice owners should expect a full-cycle process that starts before the visit and stays disciplined after adjudication. Scheduling, eligibility, authorization, coding, charge review, denial routing, appeal decisions, and write-off controls should connect to one workflow with clear ownership. If no one owns the handoff points, cash will stall there.
Start with three questions:
How much denied revenue is sitting unresolved right now?
Which specialty-specific denial patterns are repeating?
Who is accountable for fixing the cause, not just touching the claim?
If your team cannot answer those questions quickly, the practice does not have a denial management system yet. It has denial activity.
The goal is simple. Reduce avoidable denials, recover the dollars worth pursuing, and stop spending skilled staff time on work with poor return. That is how a practice gets more predictable cash flow and more control over revenue.
Frequently Asked Questions for Practice Owners
What denial rate should make me worry as a practice owner
Worry starts when denials stop being isolated and start changing cash behavior.
If payments are slowing, older A/R is climbing, or experienced staff are spending too much time correcting claims instead of preventing errors, the practice has a revenue control problem. I do not advise owners to fixate on one benchmark alone. A lower denial rate with poor follow-up can still hurt cash. A higher rate in a complex specialty may be manageable if the team can show which denials are preventable, which are recoverable, who owns each category, and how quickly those claims move to resolution.
Should my team appeal every denied claim
No. That approach wastes labor and usually lowers net recovery.
Appeals should follow a clear decision rule. Start with claim value, filing and appeal deadlines, documentation support, payer history, and the staff time required to win. In high-stakes specialties, a denied surgical case, infusion series, or advanced imaging claim may justify fast escalation because the dollars are large and the appeal record matters. A low-value denial with weak support may need correction, not appeal, or a write-off after review. The goal is margin, not motion.
How do I know whether my denials are a front-end problem or a billing problem
Follow the denial pattern back to the handoff where the error first entered the claim.
Eligibility failures, wrong subscriber data, missing referrals, and authorization mismatches usually start before the visit or at intake. Modifier errors, diagnosis-to-procedure conflicts, bundling edits, and missing documentation support usually point to coding, charge capture, or provider documentation. Many practices have both. That is why I recommend a denial map by department, payer, specialty, and root cause instead of broad conversations about where the problem "probably" sits.
When should I consider outsourcing denial management
Consider it when leadership is still asking basic questions the team cannot answer quickly.
If repeat denials keep showing up, appeals are aging past timely filing windows, payer follow-up has no clear owner, or specialty-specific rules are outpacing your internal staff, outside support may produce a better return than continuing to patch the process. The right partner should work inside your current systems, separate preventable denials from payer behavior, and show the financial effect in plain terms: dollars at risk, dollars recovered, labor saved, and the upstream fixes needed to keep the same denials from coming back.
If your practice needs a sharper denial management system, Happy Billing can review your workflow, identify where denials begin, and show you what to fix first. Request a free audit of your billing and denial process if you want a clear view of what is hurting collections, slowing A/R, and creating avoidable rework.