ICD 10 for Pain Management: Your Guide to Fewer Denials
If your pain management claims keep getting denied, the problem usually isn't the procedure. It's the diagnosis story attached to it. ICD-10 for pain management directly affects whether payers see medical necessity fast enough to pay, or kick the claim into denial, rework, and longer A/R.
We've seen the same pattern in independent practices over and over. The physician does solid work, the documentation is clinically sound, and the claim still stalls because the diagnosis is too vague, sequenced incorrectly, or disconnected from the treatment plan. That's not a coding nuisance. It's revenue leakage.
Why Your Pain Management ICD-10 Codes Cause Denials
A denied pain claim often starts with a simple mistake. The chart says “chronic pain,” the claim goes out with a broad diagnosis, and the payer's edits don't see enough specificity to support the visit, procedure, or medication management. Your staff then burns time on resubmissions, appeals, and status calls instead of moving clean claims through the door.
That gap between what coding guidance says and how payers behave is real. One documented blind spot is that ICD-10 guidelines prioritize documentation accuracy, while payers often deny claims that lack specificity, especially in chronic pain syndromes and long-term opioid therapy contexts, as discussed in QPro's analysis of pain coding and payer behavior. Practice owners feel that gap in cash flow, not in theory.
We've seen high-performing groups treat diagnosis selection as a front-end revenue control. Struggling groups treat it like a clerical step after the visit.
Where the money gets stuck
Three issues usually drive the damage:
- Vague chronic pain reporting means the payer can't easily tell etiology, chronicity, or treatment context.
- Weak support for medication status creates confusion when long-term opioid management appears on the claim without a clearly supported pain diagnosis.
- Poor documentation flow forces billing staff to guess what the physician meant, which slows submission and increases avoidable edits.
If your notes are inconsistent, tighten the process before claims ever leave the practice. Standardized templates for streamlining clinic documentation can help physicians capture the details that protect revenue, such as location, duration, laterality, and treatment rationale.
Practical rule: The cleaner the diagnosis logic in the chart, the less your billing team has to “interpret” after the encounter.
A single denied claim is irritating. A recurring pattern of diagnosis-based denials steadily inflates A/R and ties up staff time every week. If you want to identify those patterns fast, review your denial workflow against a practical framework for reducing claim denials in physician practices.
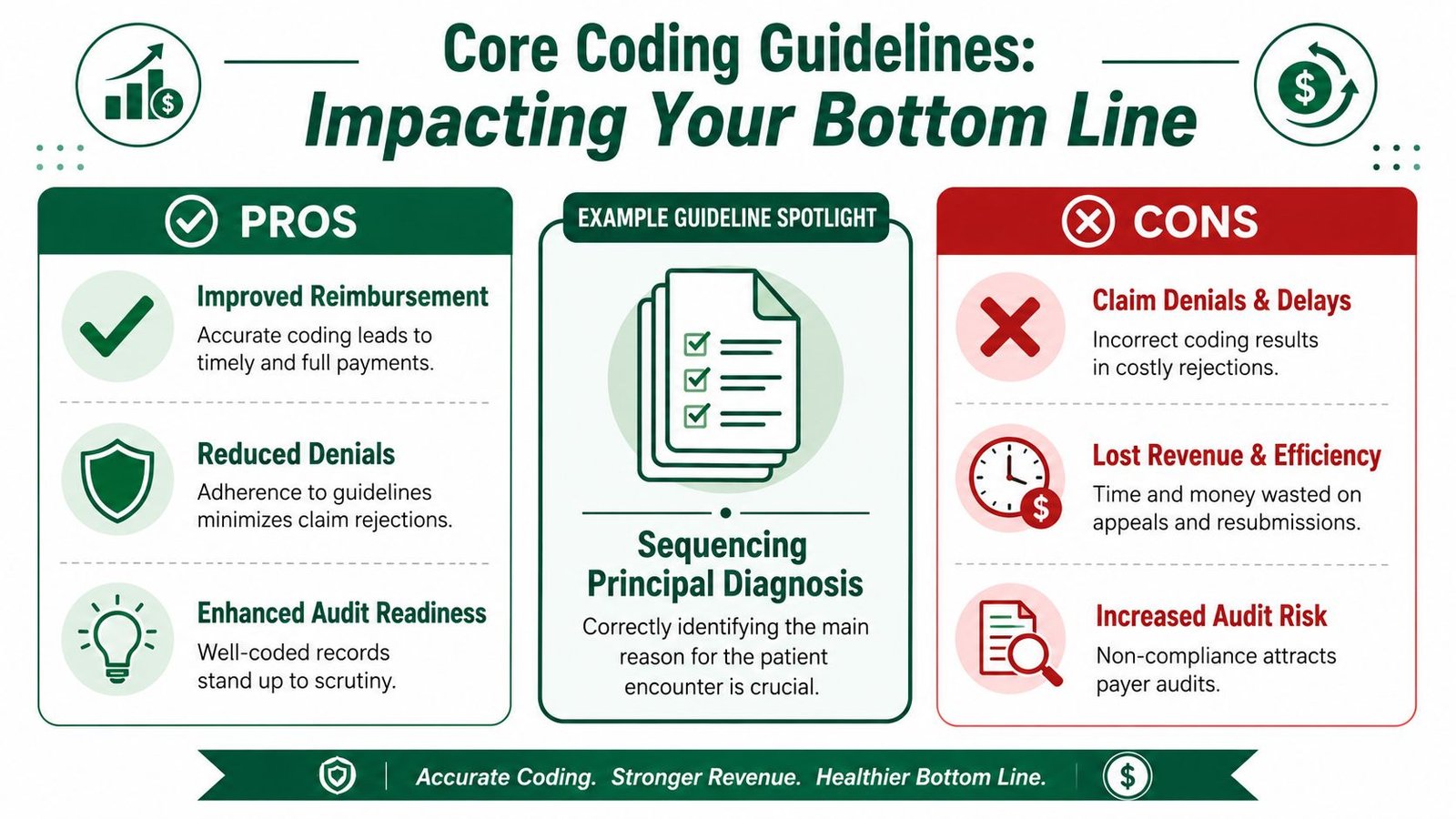
Core Coding Guidelines That Impact Your Bottom Line
The most important rule in ICD-10 for pain management is simple. Code based on the reason for the visit, not on what seems most likely to get paid. That sounds obvious, but practices lose money when the claim doesn't reflect the encounter's true purpose.
For pain-management encounters, sequencing turns into a reimbursement issue immediately. MedCare MSO's pain management coding guidance states that if the encounter is primarily for pain control, the G89 pain code is sequenced first. If the patient is being seen for another principal condition, that underlying condition is coded first and pain is reported second. The same guidance also notes that documentation should include pain location, laterality, duration, exam findings, and whether the pain is acute or chronic, especially when an E/M service is billed the same day as a procedure.
Sequencing errors are expensive
When sequencing is wrong, the payer may not understand why you billed the visit, why the procedure was necessary, or why a same-day E/M should stand separately. That's how practices end up with bundled services, medical necessity denials, or requests for records.
A few operational rules matter here:
- Pain control first when pain is the reason for the encounter. If the visit is for pain management itself, lead with the pain diagnosis.
- Underlying condition first when that condition drives the visit. If the encounter is mainly for another problem, sequence that first.
- Support the record for same-day E/M. If your physician bills an office visit with a procedure and appends modifier 25, the note has to show work beyond routine pre-procedure assessment. Your team should verify that standard against your payer rules and CPT documentation expectations.
Specificity is not optional
Laterality and duration aren't coding trivia. They're claim defense. A chart that identifies right versus left, acute versus chronic, and exam findings gives the payer fewer reasons to challenge the claim.
Better documentation doesn't just satisfy compliance. It protects the payment path.
If your leadership team is reviewing broader operational risk, this guide to healthcare compliance for regulated organizations is useful context for how documentation controls affect downstream financial performance.
Practices also need discipline around modifier usage. If your team frequently bills distinct services, review modifier logic against a payer-aware resource on modifier 59 and distinct procedural services. Coding rules only help revenue when your staff applies them consistently.
Essential ICD-10 Codes by Pain Etiology
Most practice owners don't need a giant code list. They need to know which diagnosis families consistently support payment and what the chart must prove for each one. In pain medicine, the G89 series is where many of the financially important decisions happen.
According to Training Leader's review of chronic pain ICD-10 coding, chronic pain coding in ICD-10-CM is built around specific diagnosis families rather than one generic code. That includes G89.21 for chronic pain due to trauma, G89.22 for chronic post-thoracotomy pain, G89.28 for other chronic post-procedural pain, G89.29 for other chronic pain, G89.3 for neoplasm-related pain, and G89.4 for chronic pain syndrome. The same guidance emphasizes pairing G89 codes with site-specific diagnoses when appropriate and using Z79.891 to identify long-term current use of opiate analgesics.
Chronic pain and chronic pain syndrome
A common oversight for many practices occurs here. They document long-standing pain, then default to a broad chronic pain diagnosis without identifying the source or the clinical context.
For revenue protection, your chart should make these points obvious:
- Etiology matters. Chronic pain due to trauma is not the same as chronic post-procedural pain.
- Site still matters. If the pain is low back, shoulder, or another identifiable location, pair the chronic pain code with the site-specific diagnosis when supported.
- Medication status should fit the narrative. If long-term opioid therapy is clinically relevant, Z79.891 may help complete the claim story when documentation supports it.
Neoplasm-related pain
G89.3 can be powerful when the record clearly supports neoplasm-related pain. It also attracts scrutiny if the documentation is thin. We've seen practices create avoidable denials because the assessment references “cancer history” without clearly tying the current pain management encounter to neoplasm-related pain.
That distinction matters because payers aren't reading your physician's intent. They're reading the coded claim and the documentation that supports it.
Post-procedural and trauma-related pain
These categories are often under-documented. If the pain stems from trauma, use the trauma-related chronic pain pathway when the chart supports it. If the pain is post-procedural, identify that relationship clearly instead of dropping the patient into a generic pain bucket.
The claim should answer three questions without guesswork: what kind of pain, why this pain, and why this treatment now.
High-performing practices teach physicians to document in that order. Not because coders like it. Because payers pay cleaner when the etiology is obvious.
Site-Specific Codes for Musculoskeletal Pain
Generic musculoskeletal pain coding is one of the easiest ways to sabotage a valid pain claim. If your physicians perform injections, blocks, or ongoing medication management, the diagnosis needs to localize the problem. Broad symptom reporting weakens medical necessity.
One practical example appears in ICD-10 education on pain billing. A visit may include a chronic pain diagnosis, Z79.891 for opioid therapy, and a site-specific code such as M54.5 for low back pain or M25.511 and M25.512 for shoulder pain, as outlined in DoctorPapers' overview of pain management billing logic. That approach helps payers understand where the pain is and why the treatment fits.
Why specific M codes pay better than vague ones
If your claim says “back pain” in a vague way, the payer has room to question the procedure. If it identifies low back pain or a specific joint complaint supported by the exam, the claim is stronger on its face.
That doesn't mean every site-specific code guarantees payment. It means vague coding invites unnecessary friction.
Compare the operational difference:
- Specific site coding gives your billing team a cleaner link between diagnosis and treatment.
- Unspecified pain coding creates manual review risk and more follow-up work.
- Consistent laterality and location reduce clarification requests before or after submission.
Don't confuse pain source with pain intensity
A common documentation failure is overemphasizing severity while ignoring etiology. Payers don't reimburse because pain is described as severe. They reimburse when the record shows what the pain is, where it is, how long it's been present, and why the billed service was reasonable.
A separate distinction matters in post-surgical cases. HPC Billing's guidance on post-surgical pain coding notes that G89.18 is used for other acute postprocedural pain or discomfort only when the discomfort is directly related to surgery and not explained by complications such as infection or another postoperative problem. The same guidance stresses selecting chronic pain codes based on documented etiology, not pain intensity alone.
If your practice performs procedures in orthopedic settings, this becomes even more important because diagnosis specificity affects how the entire surgical claim package holds together. For a related example on procedure-side claim logic, review this breakdown of knee arthroscopy CPT coding and billing considerations.
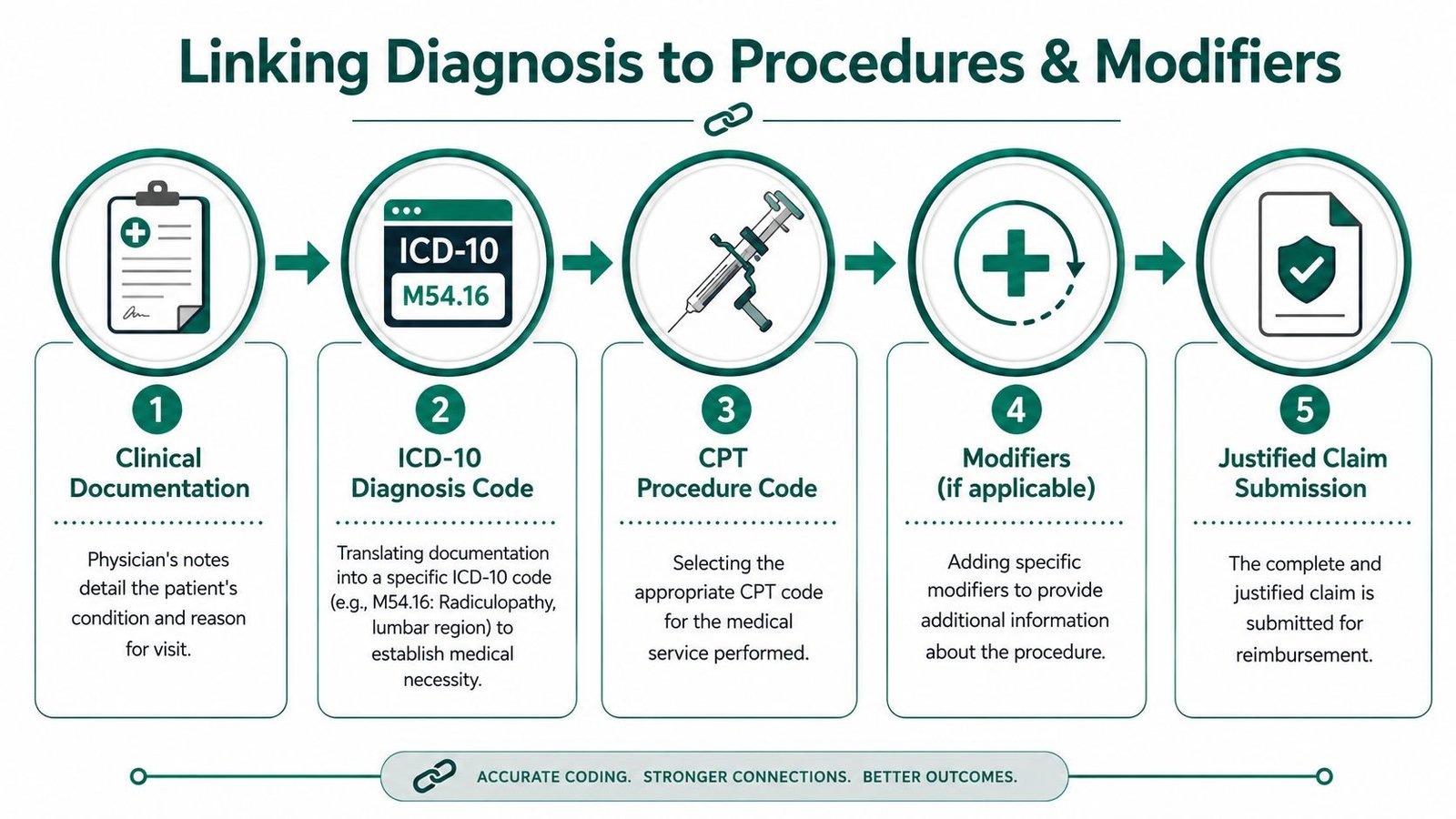
Connecting Diagnosis to Procedures and Modifiers
A pain claim gets paid when the payer sees a coherent chain. The physician documents the condition. The diagnosis code translates that condition. The CPT code reflects the service performed. The modifier explains any unusual billing circumstance. Break that chain anywhere, and reimbursement slows down.
Diagnosis is the financial foundation
In practical terms, your ICD-10 code is the “why.” Your CPT code is the “what.” If the “why” is weak, the “what” becomes harder to defend.
Take a common pain practice scenario. If your physician performs an interventional service and the diagnosis only reflects vague pain, the payer may not see a strong enough reason for the procedure. If the diagnosis precisely describes the pain source and site, the claim is easier to justify.
That matters even more for same-day E/M services.
Modifier 25 is where many practices lose money
When you bill an E/M service on the same day as a procedure, modifier 25 may be appropriate if the physician performed a significant, separately identifiable evaluation beyond the usual pre-procedure work. However, payers frequently challenge such billing.
Your practice owner takeaway is simple:
- A strong diagnosis helps defend the E/M. The more clearly the assessment explains the condition being evaluated, the better.
- The note must show separate work. History, exam, and decision-making beyond routine procedural prep need to be visible.
- Weak diagnosis coding invites bundling. If the payer can't distinguish the evaluation from the procedure, they often collapse payment into the procedure.
We've seen practices think they have a modifier problem when they have a diagnosis-story problem. The modifier is only as strong as the documentation and diagnosis logic behind it.
If the chart doesn't clearly separate the evaluation from the procedure, the payer won't do that work for you.
Pain groups that bill a range of interventions should regularly review the diagnosis-to-procedure relationship across their fee schedule. This resource on pain management CPT codes and billing strategy is a useful starting point for that review.
Top Payer Denial Traps We See Every Day
A payer requests records for a procedure your physician performs every week. The treatment was appropriate. The claim still gets denied because the diagnosis story is thin, the visit purpose is muddy, and the chart leaves the reviewer room to say no. We've seen practices lose far more to this kind of preventable denial than they lose to fee schedule cuts.
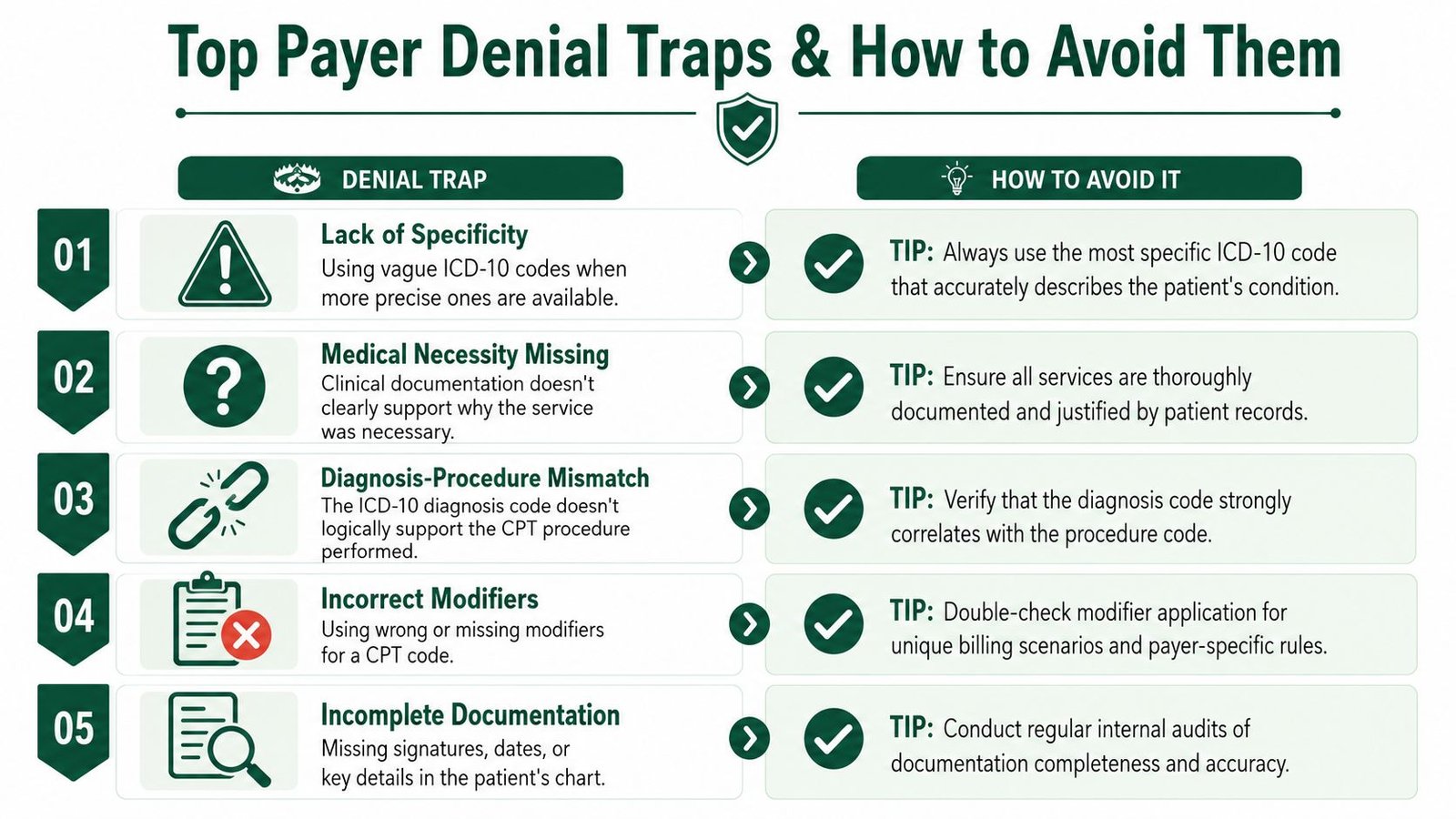
Trap one with unclear visit purpose
If the note does not clearly say whether the encounter was for pain control, medication management, follow-up after intervention, or treatment of the underlying condition, the payer gets an opening to deny medical necessity. Your billing team should never have to guess what problem the physician evaluated and why that service happened on that date.
We've seen this show up in routine follow-ups where the assessment lists several chronic conditions, but the plan focuses on pain relief. The claim goes out with diagnosis coding that does not match the actual reason for the visit. That creates avoidable denials, appeal work, and slower cash.
Your fix is operational, not theoretical. Require providers to state the visit purpose in one plain sentence at the top of the assessment and plan.
Trap two with diagnosis and treatment mismatch
Interventional pain claims often fail because the procedure and diagnosis do not line up cleanly on paper. The service may be clinically justified. The claim still pays at zero if the diagnosis submitted is vague, incomplete, or disconnected from the treatment performed.
We've seen the same pattern repeatedly:
- A general pain code leads the claim when a more specific etiology or site-based code is supported in the note
- Medication management appears isolated because the chart does not tie opioid use or monitoring back to the condition being treated
- Laterality, chronicity, or pain source is missing so the payer cannot connect the procedure to a defined problem
Revenue leaks. Staff then spend time on reconsiderations that should never have been necessary. Owners feel it in days in A/R, extra touches per claim, and write-offs that get shrugged off as payer behavior instead of fixed as coding discipline.
Trap three with modifier overconfidence
Some practices use modifier 25 like insurance against a weak claim. It is not. It increases scrutiny.
We've seen high-performing groups use a simple pre-submission standard. Before releasing the claim, they confirm that the diagnosis supports the physician work, the note proves any separate E/M service, and the chart would hold up if records were requested today. That standard protects cash because it catches bad claims before the payer does.
If denial volume keeps climbing, stop treating it as a billing-office cleanup problem. It is a revenue cycle control problem that starts with physician documentation, diagnosis selection, and claim review rules. A focused review of your revenue cycle workflow for physician practices usually shows exactly where those failures repeat.
How Better Coding Improves Your RCM Workflow
When a practice gets ICD-10 for pain management right, the benefit isn't limited to cleaner diagnosis coding. The whole revenue cycle moves better. Claims go out cleaner, staff spends less time on preventable rework, and physicians get fewer documentation queries after the fact.
We've seen the strongest practices build a simple operating rhythm. Providers document the reason for the visit clearly. The diagnosis captures etiology, site, and chronicity. The procedure coding matches that story. The billing team then submits a claim that doesn't need detective work. That's what lowers friction in the system.
What changes operationally
Better coding discipline improves workflow in ways owners notice quickly:
- Cleaner claim submission means fewer avoidable edits before the claim reaches the payer.
- Less denial rework frees staff for higher-value tasks such as A/R follow-up and authorization management.
- Stronger audit posture reduces the scramble when a payer asks for records.
- More predictable cash flow gives the practice a better handle on staffing and growth decisions.
For groups in procedure-heavy specialties, coding precision is an operational advantage. That's especially true in pain management and orthopedic revenue cycle workflows, where diagnosis specificity influences everything downstream.
If you're assessing the bigger picture, this guide to RCM for physician practices is a practical companion. Better coding isn't a back-office cleanup project. It's a financial control system.
Frequently Asked Questions
Should my practice lead with a G89 code or a site-specific code
Lead with the code that reflects the reason for the visit. If the encounter is for pain control, the pain diagnosis may need to come first. If the visit is primarily for the underlying condition, that condition comes first. The mistake we see is trying to game payer behavior instead of coding the documented encounter correctly. That usually backfires in denials and appeals.
Is Z79.891 helping my claims or making them riskier
It depends on whether the chart supports it in context. If the patient is on long-term current use of opiate analgesics and that status matters to the encounter, it can help complete the claim story. If your team adds it automatically without a clearly documented chronic pain context, it can make the claim look disjointed and invite scrutiny. Your biller should verify when it adds value versus when it's redundant.
Why do payers deny claims even when the diagnosis follows ICD-10 guidance
Because payer behavior and coding guidance don't always align neatly. ICD-10 principles focus on documentation accuracy. Payers still deny claims when they don't see enough specificity or medical necessity support. That's why practice owners need to look beyond “is this code technically valid” and ask “does this diagnosis hold up under this payer's edits, review logic, and audit posture.”
When should I worry that my pain coding process is hurting revenue
Worry when you see recurring patterns, not isolated mistakes. If the same denial reasons keep showing up, if staff spends too much time correcting diagnosis issues after encounters, or if same-day E/M claims are routinely bundled or challenged, you have a process problem. At that point, fixing one claim at a time won't solve it. You need tighter physician documentation habits, stronger pre-bill review, and better alignment between coding and payer expectations.
If your practice is losing revenue to diagnosis-driven denials, Happy Billing can help you find exactly where the leakage starts and how to fix it. Their team works with high-stakes specialties to tighten coding logic, reduce avoidable rework, and protect cash flow. If you want a clear picture of what your claims are doing right now, request a free RCM audit for your practice.