CPT Code 93308: The Definitive Guide for Cardiology
If your team is getting paid inconsistently for follow-up or focused echoes, the problem often starts with cpt code 93308. It’s the code for a limited or follow-up transthoracic echocardiogram, and using it correctly is one of the clearest ways to protect revenue while staying out of trouble on audit.
A familiar scenario in cardiology billing looks like this: the physician wanted a targeted reassessment, the report reads like a focused study, but the claim went out as 93306. That mismatch invites downcoding, bundling, or denial. On the other side, billing 93308 without documentation that explains why the study was limited creates the same problem for a different reason.
For practice managers and physician owners, this isn’t academic coding trivia. 93308 sits right at the intersection of reimbursement, modifier strategy, documentation quality, and claim scrubber logic. If your workflows around limited echoes are loose, you’ll see it in clean-claim performance, preventable denials, and delayed cash.
Your Definitive Guide to CPT Code 93308
CPT code 93308 is used to bill a limited or follow-up transthoracic echocardiography study. It’s the correct code when the exam answers a focused clinical question rather than delivering a complete structural assessment of the heart.
That distinction matters because payers don’t reimburse intent. They reimburse the service that was performed and documented. If the encounter was targeted, the code should be targeted. If the study was extensive, a limited code won’t hold up.
In daily operations, 93308 becomes expensive when teams treat it as “just a smaller echo.” It isn’t. It has its own coding logic, its own documentation expectations, and its own bundling traps. A focused study for pericardial effusion follow-up, left ventricular function reassessment, or a valve check after intervention can be entirely appropriate for 93308. A report that drifts into broad language without defining the limited scope can undermine the claim.
Why this code creates so much leakage
The biggest issue is that clinical intent, report wording, and claim construction often fall out of alignment. The physician may order a limited study. The sonographer may capture focused views. But if the interpretation reads like a broad survey, coders are left guessing between 93306, 93307, and 93308.
That guessing costs money.
Practical rule: If the report doesn’t clearly state the focused clinical question and the scope limitation, your billing team is already defending the wrong fight.
A strong 93308 workflow has three parts:
- Order discipline: The indication should support a limited or follow-up exam.
- Report discipline: The interpretation should identify what was examined and what was not intended to be examined.
- Claim discipline: Modifiers, add-on codes, and same-day edits must match the actual service line by line.
Where experienced RCM teams focus
Seasoned cardiology RCM teams don’t just ask whether 93308 is “billable.” They ask whether the claim is defensible. That means the code choice, modifier use, and report language all need to point in the same direction.
When practices tighten that alignment, denials typically shift from recurring operational mistakes to occasional payer disputes. That’s a much better place to be.
Clinical Description and Appropriate Use Cases
CPT code 93308 represents a limited or follow-up transthoracic echocardiography study using real-time 2D imaging with M-mode recording capability. It belongs to a defined subset of echo services and should be used when the exam is intentionally focused, not a full study, as described in this CPT 93308 coding overview.

The easiest way to code 93308 correctly is to think in terms of clinical question density. A complete transthoracic study addresses the heart broadly. A limited study addresses one issue, or a narrow set of related issues, and stops there.
How 93308 differs from 93306 and 93307
The contrast is straightforward:
- 93306 is the complete transthoracic echo with detailed 2D, spectral Doppler, and color flow Doppler components.
- 93307 is 2D imaging without Doppler studies.
- 93308 is reserved for limited or follow-up evaluation.
That means 93308 is not a cheaper version of 93306. It’s a different service category. In practice, the report should read like a focused reassessment, not a full baseline study with abbreviated wording.
A useful administrative checkpoint is pre-service order review. If your front-end team struggles with when a focused exam should move through scheduling and authorization workflows, this guide to prior authorization in healthcare is worth keeping in your internal training library.
Defensible use cases in real cardiology operations
The most defensible 93308 claims usually involve follow-up or surveillance of a known issue. Common examples include:
- Pericardial effusion follow-up: The physician needs to know whether fluid is present, increased, decreased, or stable.
- Left ventricular function reassessment: The clinical question is targeted to ventricular performance rather than full chamber and valve review.
- Post-intervention valve check: The encounter focuses on a specific valve or a narrow post-procedural concern.
- High-acuity bedside cardiac ultrasound: The clinician needs a focused answer that affects immediate decision-making.
These are all situations where a complete study may be unnecessary if the clinical question is narrow and the documentation reflects that.
What doesn’t work
What fails most often is using 93308 when the team really performed a broad evaluation but documented it loosely. Payers usually read that as a coding inconsistency, not as harmless shorthand.
Another common failure is the opposite one. The provider performs a focused reassessment but the report includes generic phrases that imply a full echo template. If the note says “echo performed” without explaining the narrow purpose and limited scope, coders inherit avoidable ambiguity.
A limited study should sound limited on the page. If the report reads comprehensive, the payer will usually code it that way before your staff gets the chance.
There’s also a practical opportunity with advanced imaging combinations. The American Society of Echocardiography specifies that 0439T may be reported with 93308 as the primary procedure in appropriate circumstances, which gives practices added flexibility when the clinical scenario justifies it.
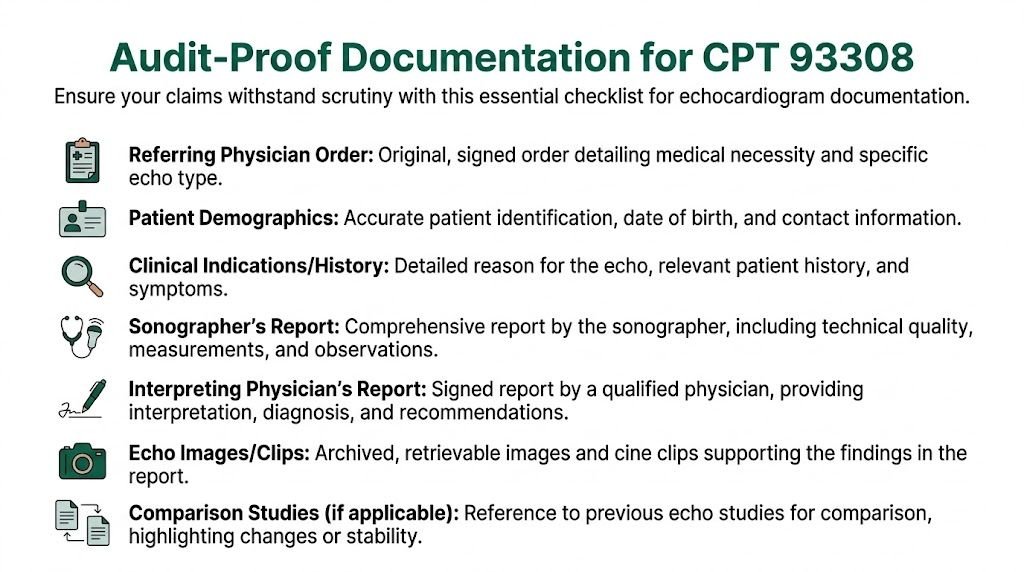
Audit-Proof Documentation Requirements for 93308
For cpt code 93308, documentation is where compliant reimbursement is either secured or lost. CPT guidance states that 93308 “does not evaluate (or document the attempt to evaluate) all the structures that comprise the complete echocardiographic exam,” and payers scrutinize reports that fail to justify why the study was limited, as noted in this AAPC discussion of 93306 vs 93308.
A payer doesn’t need to prove your provider meant to upcode. They only need to show that the record doesn’t support the code billed. That’s why 93308 denials often hinge on scope language more than image quality.
The four elements that should appear every time
At minimum, the interpreting physician’s report should lock down four points:
The medical indication for the limited study
State the focused reason for the exam. “Follow-up pericardial effusion” is stronger than “cardiac evaluation.”The focused imaging protocol used
The record should make clear that this was a targeted exam, not an incomplete complete exam.The specific cardiac structures examined
Name the structures assessed. Don’t leave the payer to infer them.The explicit scope limitation
The report should say that the study was limited or focused and should connect that limitation to the clinical question.
Those are the basics. Without them, your 93308 claim becomes vulnerable even if the service itself was appropriate.
What strong report language looks like
Here’s an important distinction often overlooked: documentation for 93308 shouldn’t just describe findings. It should also explain why a limited exam was clinically appropriate.
Focused transthoracic echocardiogram performed as a limited follow-up study to reassess known pericardial effusion. Imaging was directed to the pericardial space and ventricular function. This was not a complete echocardiographic examination. Findings are limited to the structures evaluated for the stated clinical indication.
That kind of language works because it does three things at once. It states the indication, confirms the scope, and prevents the payer from treating the record like an undocumented incomplete thorough study.
If your internal QA process centers on first-pass accuracy, it helps to train coders and charge posters against the same standards used for a clean claim in medical billing. For 93308, “clean” means the report and the code tell the same story.
A practical documentation checklist for the billing side
Billing leaders should audit 93308 notes against a short checklist before charges drop:
- Clinical question present: The note explains the reason for a limited study.
- Limited scope stated: The report uses language such as limited, focused, or follow-up and makes that meaningful.
- Structures identified: The examined structures are named.
- Interpretation tied to indication: Findings answer the reason the test was ordered.
- No template drift: The report doesn’t accidentally imply a complete study.
What routinely triggers denials
Three report patterns repeatedly create trouble:
- Generic indications like “echo follow-up” with no targeted reason.
- Template overreach where a complete-echo structure remains in the final report.
- Missing limitation language that never explains what was intentionally not part of the study.
The denial isn’t always immediate. Sometimes the claim pays and then gets pulled into post-payment review. That’s harder to fix because the payer is no longer just processing a claim. They’re questioning the integrity of the code selection.
Billing 93308 successfully is less about saying less and more about saying the right narrow things with precision.
Mastering Modifiers and Bundling Rules
The fastest way to lose money on cpt code 93308 is to get the modifier logic wrong. The second fastest is to pair it with an inclusive code and let the payer’s edits reduce the claim automatically.
93308 uses a dual-component billing structure. Modifier TC identifies the technical component, and modifier 26 identifies the professional component. The technical portion reimburses 40% to 50% of the total value, according to this modifier and bundling reference for 93308.
When to use 26 and when to use TC
Use 93308-26 when the physician is billing only for interpretation and report. That’s common when the facility owns the equipment and the cardiologist reads the study.
Use 93308-TC when the entity billing supplied the equipment, staff, and image acquisition, but not the professional interpretation.
Bill 93308 globally only when the same billing entity legitimately owns both pieces of the service and payer rules allow global billing in that setting.
Here’s the clean operational test: ask who owned the machine, who employed the sonographer, and who issued the interpretation. If those aren’t all the same entity, global billing usually needs a second look.
Common modifiers for CPT 93308
| Modifier | Name | When to Use |
|---|---|---|
| 26 | Professional component | Physician bills only for interpretation and report |
| TC | Technical component | Facility or practice bills only for equipment and image acquisition |
| GC | Service performed by resident under supervision | Use when payer rules and teaching setting requirements support it |
For teams that still see confusion between split billing and global billing, this internal guide on modifier 26 vs TC is a practical reference.
Add-on codes and where revenue is won or lost
One of the more valuable features of 93308 is that it can support focused billing with medically necessary add-on services. In high-acuity settings, clinicians may report 93308 with add-on codes such as 93321 for spectral Doppler and 93325 for color flow Doppler when each service is independently performed and documented. In that setting, reimbursement per case may increase 20% to 35% compared with billing a complete echo alone, as described by the American College of Emergency Physicians on emergency echocardiography coding.
That doesn’t mean every focused study should carry add-on codes. It means the service line should reflect what was done. If Doppler or color flow was medically necessary and separately documented, leaving it off the claim can understate the encounter. If it wasn’t separately supported, adding it creates an audit problem.
The payer’s question is simple: was this additional modality distinct, medically necessary, and documented as such? If the answer isn’t obvious in the record, expect bundling pressure.
Same-day combinations that trigger bundling
Claim scrubbers need to be strict; 93308 cannot be submitted on the same date of service as 93014, 93041, 93306, 93307, or as a component of stress echo 93350, because those services are inclusive and can trigger automatic bundling and claim reduction.
That rule has direct workflow implications:
- Don’t let coders “stack” complete and limited echo codes on the same DOS to reflect effort.
- Don’t append modifiers reflexively to try to force payment on combinations that are inclusive.
- Do audit charge capture templates if your EHR makes both complete and limited options easy to click in the same encounter.
What works operationally
The best-performing cardiology groups usually standardize 93308 around a short decision tree:
- Was the study intentionally limited?
- Did the interpretation state the focused question and limited scope?
- Was the bill global, professional-only, or technical-only?
- Were any add-on codes independently documented?
- Did the claim pass same-day bundling edits before submission?
That’s not overengineering. It’s basic margin protection.
Common Claim Scenarios and ICD-10 Pairing
The rules become easier when you look at actual claim construction. CPT code 93308 is the predominant billing code for point-of-care cardiac ultrasound in high-acuity settings, especially in emergency departments, and it can support medically necessary add-on coding when the documentation is separate and specific, as described in the earlier ACEP reference.
The examples below are practical billing patterns, not payer guarantees. Final claim construction should always match the chart, place of service, and contract terms.
Scenario one emergency department focused cardiac assessment
An emergency physician performs a focused bedside cardiac ultrasound to evaluate for tamponade physiology in a high-acuity setting. The physician interprets the study, documents the limited scope, and the facility owns the equipment.
Claim logic
- Professional claim: 93308-26
- ICD-10-CM: I31.3
- Place of service: Facility-specific claim logic applies
This is the classic split-billing setup. The physician bills the interpretation only. The facility would separately evaluate whether it should bill the technical component based on its own operational and payer rules.
What makes this claim hold up is not the urgency of the encounter. It’s the report language showing that the study answered a narrow cardiac question rather than serving as a full echo.
Scenario two outpatient follow-up for known valve disease
A cardiology practice brings back a patient with known aortic stenosis for a focused reassessment tied to a specific clinical concern. The provider performs and interprets a limited transthoracic study in-office, and the documentation stays within the defined scope.
Claim logic
- Global claim: 93308
- ICD-10-CM: I35.0
In this scenario, the same entity may be billing both technical and professional components. The coding risk is less about modifiers and more about over-documentation. If the report reads like a broad structural survey, the payer may question why a complete study wasn’t billed instead.
Scenario three limited echo plus Doppler add-on
A patient returns for focused assessment of ventricular function, and the clinician also performs a medically necessary spectral Doppler evaluation that is separately documented.
Claim logic
- Primary code: 93308
- Add-on code: +93321
- Diagnosis code: Pair the claim with the documented condition or symptom that supports medical necessity
Concerning this, many practices either leave money behind or create denials. If the Doppler work was done and separately supported, the add-on may be appropriate. If the chart treats it like an unspoken part of the limited exam, the payer may bundle or deny it.
A quick pairing framework for coders
Use this mental sequence before release:
- Start with the clinical question: Why was the echo limited?
- Choose the billing structure: Global, 26, or TC.
- Add only distinct supported services: +93321, +93325, or other permitted additions only when separately documented.
- Validate diagnosis linkage: The ICD-10 code should explain why this focused exam was medically necessary.
Clean 93308 claims usually look simple on the claim form and highly specific in the chart. Complicated claims with vague reports are the ones that age in A/R.
Reimbursement Rates Denials and Appeal Strategies
From an RCM standpoint, cpt code 93308 is worth managing closely because the reimbursement spread is meaningful. According to 2026 fee schedule data, major payers reimburse 93308 at national average rates ranging from $131.34 to $169.35, and the variance can reach 22% depending on geography and local MAC interpretation of Medicare policy, as shown in this 2026 CPT 93308 fee schedule reference.
The code is commonly billed in inpatient hospital settings (POS 21) and emergency rooms (POS 23), and reimbursement support depends on documentation of moderate-level medical decision-making in the record.
The denial patterns that matter most
Most 93308 denials fall into a small set of categories:
- Medical necessity not established
- Documentation inconsistent with limited scope
- Bundled with an inclusive same-day service
- Modifier mismatch between professional and technical billing
These denials don’t all deserve the same response. A scope denial is a chart problem. A bundling denial may be a code-pairing problem. A modifier denial may be a charge-entry problem. Treating all of them with the same generic appeal language wastes time.
Appeal language that is usually worth using
For a medical necessity denial, the appeal should make the focused nature of the service explicit:
The submitted claim reflects a limited transthoracic echocardiographic study performed to address a specific documented clinical question. The medical record supports the targeted indication, the structures examined, and the physician interpretation tied to that indication.
For a scope denial, anchor the appeal to the limited design of the service:
The record documents that this was a focused follow-up examination rather than a complete echocardiographic study. The report identifies the specific structures evaluated and states the limited scope of the examination.
For an edit or bundling denial, be direct:
Please reprocess this claim after review of the billed code combination and supporting documentation. The submitted service reflects the documented procedure performed and should be evaluated under applicable payer edit logic and component billing rules.
If your team is seeing recurring cardiology imaging denials, it’s useful to benchmark your workflow against a structured cardiology billing denials process rather than handling each claim as a one-off exception.
Where practices usually recover the most cash
The most recoverable 93308 denials are often not the ones with dramatic clinical complexity. They’re the straightforward limited studies where the chart supported the service, but the claim failed because of sloppy modifier use, template drift, or a same-day code conflict.
That’s why 93308 should be monitored at the workqueue level. If one payer repeatedly rejects 93308-26, or if one clinic location shows a pattern of complete-echo wording on limited studies, that’s an operational signal. Fix the source, not just the denied claims.
RCM Checklist for Optimizing 93308 Claims
For cpt code 93308, the most impactful improvement is consistency. Not better heroics after denial. Better controls before submission.
A practical checklist your team can use
- Before the study: Confirm the order supports a limited or follow-up transthoracic echo, not a complete study.
- At the point of service: Make sure the provider documents the focused clinical question, the structures examined, and the fact that the exam was limited.
- During coding: Choose between 93308, 93308-26, or 93308-TC based on who performed and owned each component.
- Before claim release: Scrub for inclusive same-day combinations, especially 93306, 93307, 93014, 93041, and 93350.
- When add-on services appear: Validate that 93321, 93325, or other permitted additions are separately documented and medically necessary.
- After submission: Trend denials by payer, site, and provider report template.
The operational habit that changes results
The most effective 93308 programs don’t leave this code to coder preference. They build a repeatable pathway between scheduling, imaging, interpretation, charge capture, and denial follow-up.
For cardiology groups that want a broader operational framework, this overview of cardiology revenue cycle management is a useful next read. If you’re evaluating specialty support, Happy Billing’s cardiology billing page is the relevant specialty resource.
Frequently Asked Questions About CPT 93308
Can 93308 be used for a screening exam on an asymptomatic patient
No. 93308 is a diagnostic imaging code and needs medical necessity. If the chart doesn’t show a symptom, known condition, or focused clinical reason for the study, the claim is difficult to defend and may be denied.
For billing teams, the practical issue is diagnosis linkage. A vague or screening-oriented order usually isn’t enough. The order and report should both support why a limited cardiac study was necessary.
How do payer-specific policies affect 93308 billing
CMS rules and coding logic establish the baseline, but private payer policies still shape what gets paid and what gets pended. Some payers apply tighter diagnosis edits, stricter documentation review, or different expectations around add-on code support.
That’s why annual contract and policy review matters. A payer may follow standard component billing principles but still deny claims if your report language doesn’t match its imaging policy language closely enough.
What is the difference between 93308 and 76629
93308 is for echocardiography of the heart. 76629 is for a limited or follow-up ultrasound of the chest that excludes the heart.
That distinction matters because the anatomy drives the code family. If the physician is assessing cardiac structures or function, 93308 is the relevant echo code to evaluate. If the exam targets non-cardiac chest structures, a chest ultrasound code may be the more accurate path.
Is prior authorization typically required for 93308
It depends on the payer and the place of service. In inpatient and emergency settings, prior authorization usually isn’t the operational issue. In scheduled outpatient settings, commercial payer requirements can be more restrictive.
The billing lesson is simple. Don’t assume the setting answers the question by itself. Your staff should verify the payer’s current rules before a scheduled outpatient study and document the authorization status clearly.
Happy Billing helps specialty practices tighten coding accuracy, prevent denials, and accelerate payment without forcing an EHR migration. If your cardiology group needs stronger control over limited echo billing, modifier usage, and denial recovery, Happy Billing is built for exactly that kind of revenue cycle work.